Advanced Pelvic Support Osteotomy: Restoring Stability in Complex Hip Deformities
Key Takeaway
Pelvic Support Osteotomy is an advanced orthopedic procedure addressing unstable, chronically dislocated, or severely deformed hips. It aims to restore stability, functional gait, and correct limb length discrepancies by applying Dr. Paley's principles of deformity correction, including CORA and mechanical axis restoration, to achieve biomechanical efficiency.
Introduction to Hip Joint Malalignment and the Unstable Hip
The management of the unstable chronically dislocated or severely deformed hip remains one of the most formidable challenges in orthopedic surgery. Conditions such as neonatal septic arthritis severe neuromuscular disorders paralytic poliomyelitis and failed total hip arthroplasties resulting in Girdlestone resections often leave patients with profound limb length discrepancies severe Trendelenburg gait and debilitating biomechanical inefficiency.
For decades the standard salvage procedures either fell short of restoring functional gait or introduced new equally problematic deformities. However the application of Dr Dror Paley principles of deformity correction specifically the Center of Rotation of Angulation methodology combined with the Ilizarov method has revolutionized our approach to the hip joint.
This comprehensive masterclass will deconstruct the biomechanics preoperative planning and surgical execution of the Pelvic Support Osteotomy. By mastering these advanced hip joint considerations surgeons in training can transform a biomechanically disastrous lower extremity into a stable functional and aligned limb.
Biomechanical Consequences of the Chronically Dislocated Hip
To truly appreciate the power of the Pelvic Support Osteotomy one must first understand the catastrophic biomechanical failure of the chronically dislocated hip. In a normal hip joint the femoral head acts as a stable fulcrum within the acetabulum. The hip abductors primarily the gluteus medius and minimus operate on a lever arm extending from the greater trochanter to the center of the femoral head. This mechanism stabilizes the pelvis during the single leg stance phase of gait.
When the hip is dislocated or absent the fulcrum is lost. The abductor lever arm effectively becomes zero. Consequently the abductor musculature cannot generate the torque required to keep the pelvis level. This results in a severe Trendelenburg gait where the pelvis drops precipitously on the contralateral side during the swing phase.
To compensate the patient must aggressively shift their center of gravity laterally over the dislocated hip during the stance phase resulting in a pronounced lurch. This compensatory mechanism requires massive energy expenditure leading to early fatigue chronic lower back pain and progressive spinal deformities such as compensatory scoliosis. Furthermore the proximal migration of the femur results in a profound functional and structural limb length discrepancy compounding the gait abnormality.
Foundational Paley Principles in Hip Deformity
The correction of complex lower extremity deformities relies entirely on a standardized reproducible geometric framework. Dr Dror Paley established these foundational principles which allow surgeons to map any deformity regardless of its complexity.
Center of Rotation of Angulation CORA
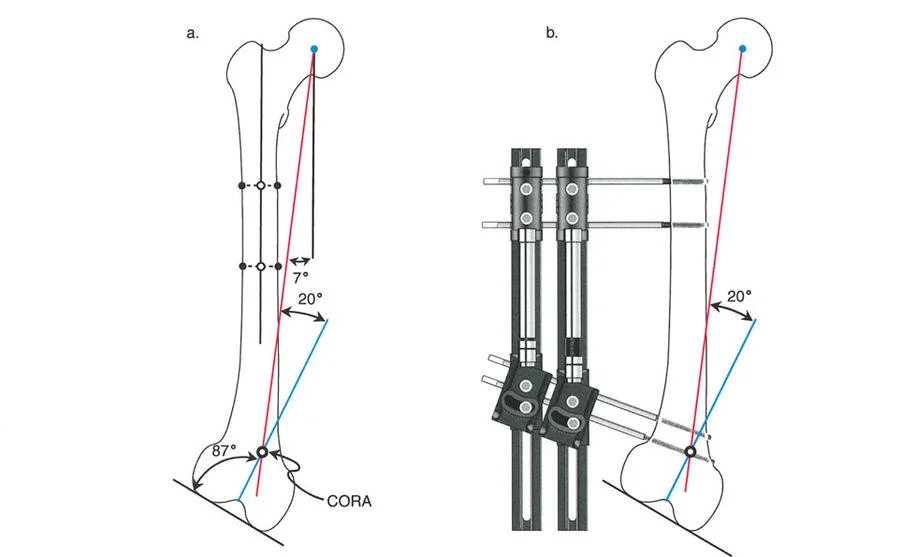
The CORA is the point at which the proximal and distal mechanical or anatomic axes of a deformed bone intersect. In the context of the hip the CORA represents the epicenter of the angular deformity resulting from the dislocation and proximal migration of the femur. Identifying the CORA is the absolute first step in planning a corrective osteotomy. Paley osteotomy rules dictate that if an osteotomy is performed at the CORA and angulated around it the mechanical axis will be perfectly restored without introducing translation.
Mechanical Axis Deviation MAD
The mechanical axis of the lower extremity normally passes from the center of the femoral head through the center of the knee to the center of the ankle. When the hip is dislocated the proximal reference point is lost and the mechanical axis is severely deviated usually shifting drastically medial to the knee joint. This Mechanical Axis Deviation MAD leads to abnormal joint reactive forces premature osteoarthritis of the knee and gross clinical instability. The ultimate goal of the double level pelvic support osteotomy is to restore MAD to neutral while simultaneously providing pelvic stability.
Joint Orientation Angles
Understanding normal joint orientation angles is critical for identifying concomitant deformities in the distal femur or proximal tibia before executing a pelvic support osteotomy.
| Joint Orientation Angle | Abbreviation | Normal Value Range | Clinical Significance in Hip Deformity |
|---|---|---|---|
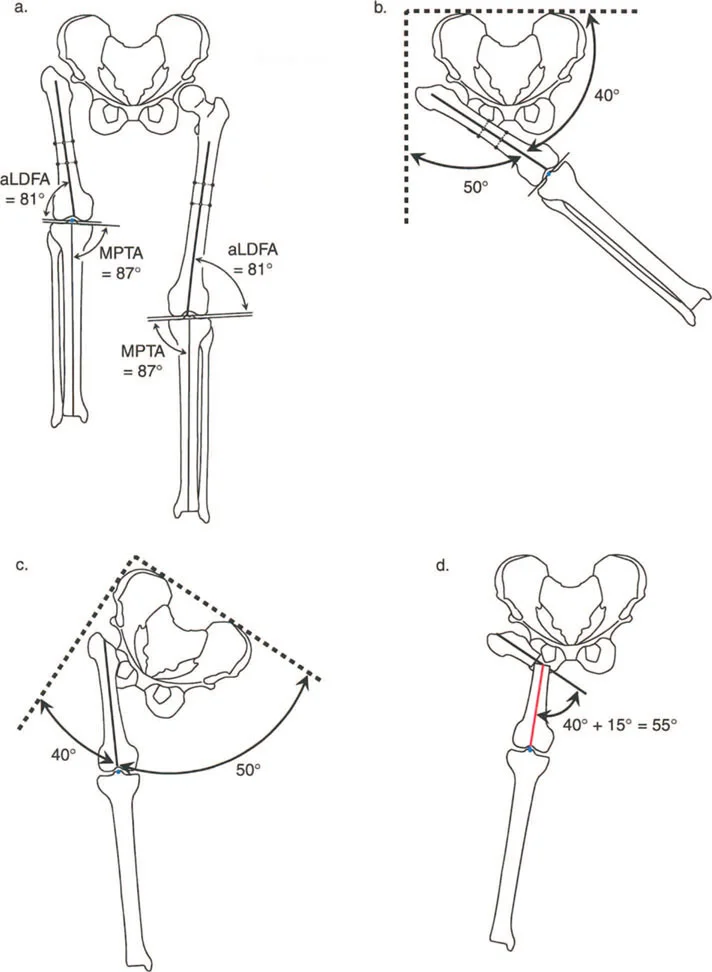
| Mechanical Lateral Distal Femoral Angle | mLDFA | 87 to 90 degrees | Identifies distal femoral varus or valgus which alters the Distal Mechanical Axis |
| Medial Proximal Tibial Angle | MPTA | 87 to 90 degrees | Identifies proximal tibial deformities that must be accounted for in multiapical planning |
| Joint Line Congruency Angle | JLCA | 0 to 2 degrees | Assesses knee joint ligamentous laxity or intra articular deformity |
| Mechanical Lateral Proximal Femoral Angle | mLPFA | 85 to 95 degrees | Normally references the femoral head but is absent or distorted in the dislocated hip |
Establishing Pelvic Reference Lines
Before any deformity correction can be planned accurate radiographic reference lines must be established. The hip joint is unique because its proximal reference is the pelvis itself a complex three dimensional structure that is highly susceptible to rotational and tilt distortions on standard two dimensional radiographs.
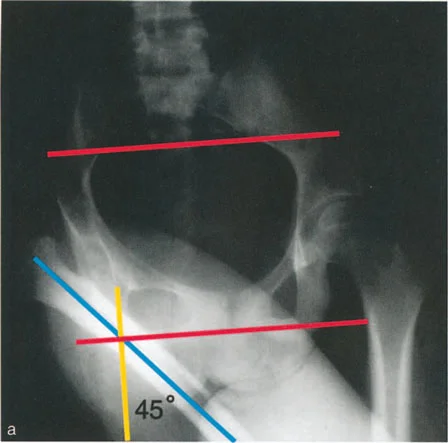
The Horizontal Line of the Pelvis
To accurately assess limb alignment and plan a pelvic support osteotomy the surgeon must first define the true horizontal line of the pelvis. If the pelvis is distorted due to congenital anomalies asymmetric growth and development or previous surgical interventions identifying a reliable horizontal axis is critical.
The most accurate radiographic landmarks for drawing the horizontal pelvic line include
* The Sacroiliac Joints A line drawn across the inferior end of the sacroiliac joints is highly reliable.
* The Sacral Foramina Alternatively a line can be drawn across two corresponding sacral foramina.
* The Triradiate Cartilages In pediatric patients a line connecting the two triradiate cartilages is highly useful provided no previous pelvic osteotomies such as Salter Dega or Pemberton have been performed.
Proximal and Distal Mechanical Axis Lines
Once the horizontal line of the pelvis is established the mechanical axes of the lower extremity can be mapped.
Proximal Mechanical Axis Line The PMA line is drawn strictly perpendicular to the horizontal line of the pelvis passing directly through the center of the acetabulum or the intended center of rotation if the femoral head is absent. This line represents where the mechanical axis of the femur should ideally be located to support the pelvis.
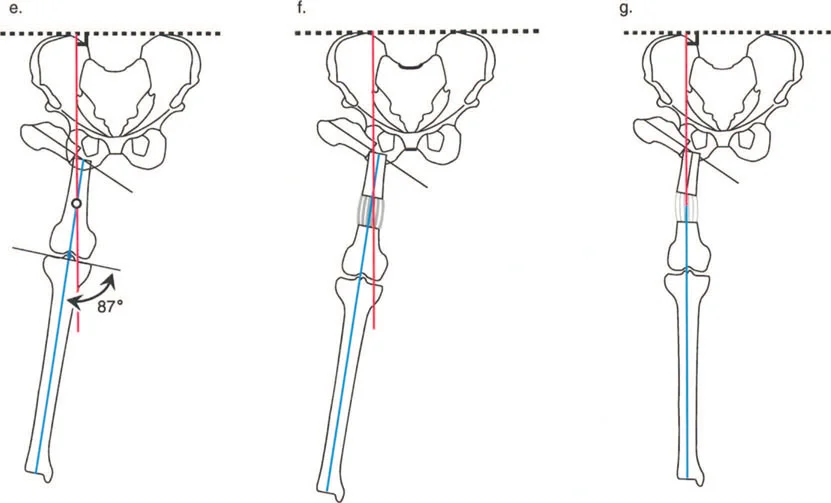
Distal Mechanical Axis Line The DMA line is drawn from the center of the ankle joint through the center of the knee joint and then extended proximally toward the hip. This line represents the current mechanical alignment of the distal segment of the limb.
If there is any preexisting proximal tibial or distal femoral malalignment this must be identified immediately. This is done by performing the Mechanical Axis Deviation Orientation Test between the knee joint line the anatomic axis of the femur and the mechanical axis of the tibia.
If malalignment of distal femoral or tibial origin is present the surgical planning must be approached as a multiapical deformity. The only difference from standard long bone planning is that the proximal reference line of the femur is based entirely off the pelvis rather than the proximal femur itself.
Locating the Hip CORA and Multiapical Considerations
If there is no other CORA in the limb meaning the femur and tibia are straight the line perpendicular to the pelvis PMA and the line generated by the proximal extension of the tibial mechanical axis DMA will intersect.
This intersection point represents the new CORA of the hip deformity. To restore alignment the surgeon must follow Paley osteotomy rules when correcting the deformity relative to this specific CORA.
In cases of a chronically dislocated hip the CORA is typically located in the proximal third of the femur. However because the proximal femur is highly mobile and lacks a stable articulation the exact location of the CORA changes depending on the adduction or abduction of the limb. Therefore the clinical examination plays a critical role in finalizing the radiographic planning.
Surgical Pearls for CORA Identification
* Always obtain a standing full length anteroposterior radiograph of both lower extremities with the patellae facing strictly forward.
* Account for fixed flexion deformities of the knee or hip as these will distort the coronal plane projection of the mechanical axis.
* If a distal femoral deformity exists map its CORA first and simulate its correction before mapping the proximal hip CORA.
Evolution of the Pelvic Support Osteotomy
A variety of pelvic support osteotomies were attempted during the first half of the twentieth century by pioneers such as Hass and Milch. The original rationale was simple. If the hip is dislocated and unstable angle the proximal femur into extreme valgus so that it rests against the pelvis thereby providing a bony buttress to support the patient body weight.
The Flaws of Single Level Osteotomies
These early single level osteotomies were fundamentally flawed. While they provided some pelvic support they created massive secondary problems that often left the patient worse off biomechanically.
- Severe Knee Valgus The extreme valgus angulation of the proximal femur shifted the mechanical axis drastically lateral to the knee joint. This resulted in severe genu valgum leading to rapid degeneration of the lateral compartment of the knee and stretching of the medial collateral ligament.
- Exacerbated Limb Shortening The angulation further shortened an already compromised limb. Because the osteotomy was purely angular without any lengthening component the functional limb length discrepancy worsened requiring the patient to wear massive shoe lifts.
- Loss of Pelvic Support Over Time Because the mechanical axis was not restored the sheer forces across the proximal osteotomy site often led to remodeling and loss of the valgus buttress over time resulting in a recurrence of the Trendelenburg gait.
With the advent of Total Hip Arthroplasty these single level osteotomies were largely abandoned. However THA is not a viable option for young patients with neonatal septic hips active infections severe neuromuscular paralysis or massive bone loss following multiple failed revisions.
The Ilizarov Double Level Modification
The Ilizarov method sparked a renewed interest in the pelvic support osteotomy by solving the critical flaws of the Milch procedure. Gavriil Ilizarov revolutionized the concept by introducing two major modifications.
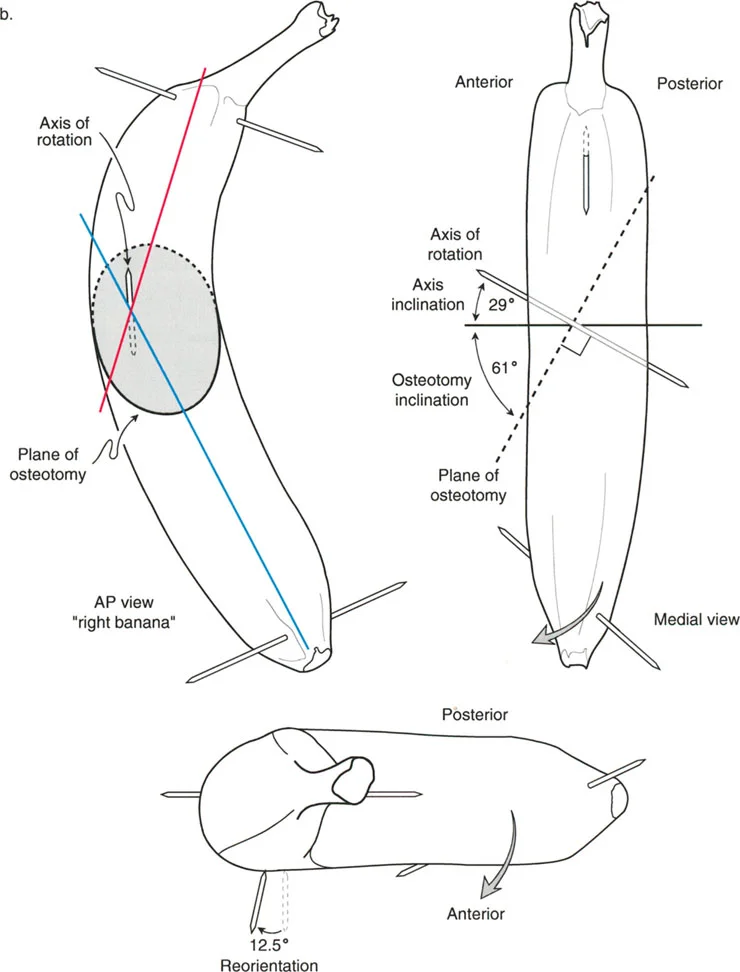
- Three Dimensional Correction He considered not only the frontal coronal plane but also the sagittal and axial planes. The proximal osteotomy was designed to incorporate extension to correct fixed flexion deformities and rotation to optimize the foot progression angle.
- The Second Distal Osteotomy Ilizarov added a second osteotomy located distal to the first. The sole purpose of this distal osteotomy is the realignment of the mechanical axis curing the knee valgus and the equalization of limb length through distraction osteogenesis.
This double level approach remains the definitive and perhaps the only way to stabilize a neonatal septic hip without resorting to massive endoprosthetic reconstructions or arthrodesis. The proximal osteotomy eliminates the Trendelenburg gait by providing a stable fulcrum against the pelvis while the distal osteotomy restores the mechanical axis and equalizes limb length.
Preoperative Planning for Double Level Pelvic Support Osteotomy
Meticulous preoperative planning is the cornerstone of a successful double level pelvic support osteotomy. The planning process integrates clinical examination findings with precise radiographic templating.
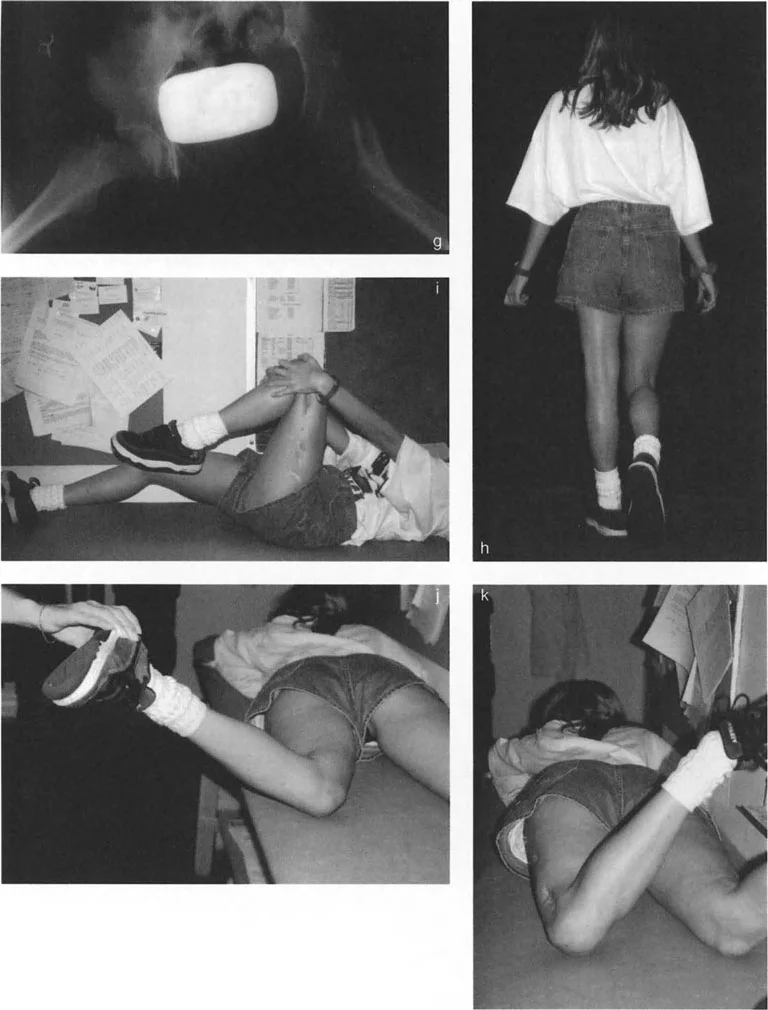
Clinical Examination and Maximum Adduction Angle
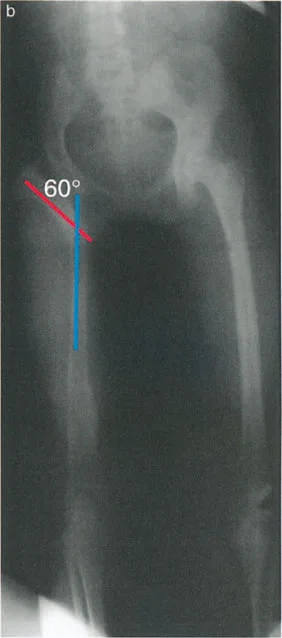
The most critical clinical measurement is the Maximum Adduction Angle. This angle determines exactly how much valgus must be engineered into the proximal osteotomy to provide adequate pelvic support.
To measure the Maximum Adduction Angle
1. Place the patient in a supine position on a firm examination table.
2. Abduct the contralateral normal leg out of the way to clear the path for the affected leg.
3. Palpate the anterior superior iliac spines to monitor pelvic tilt.
4. Slowly adduct the affected leg across the midline.
5. Stop adduction the exact moment the pelvis begins to tilt.
6. The angle formed between the affected femur and the midline of the body is the Maximum Adduction Angle.
The required valgus angle for the proximal osteotomy is calculated as the Maximum Adduction Angle plus an additional 15 degrees.
Why add 15 degrees? During normal human gait the pelvis drops approximately 15 degrees on the swing side. By overcorrecting the valgus by 15 degrees the surgeon ensures that the proximal femur remains in contact with the lateral wall of the pelvis even when the pelvis tilts during the dynamic phases of gait. This overcorrection is the secret to completely eliminating the Trendelenburg lurch.
Radiographic Templating and Osteotomy Rules
Once the required proximal valgus angle is determined the surgeon must template the distal osteotomy to restore the mechanical axis.
- Draw the Proximal Osteotomy On the anteroposterior radiograph mark the planned proximal osteotomy site. This is typically located at the level of the ischial tuberosity when the hip is maximally adducted. Apply the calculated valgus angle MAA plus 15 degrees at this level.
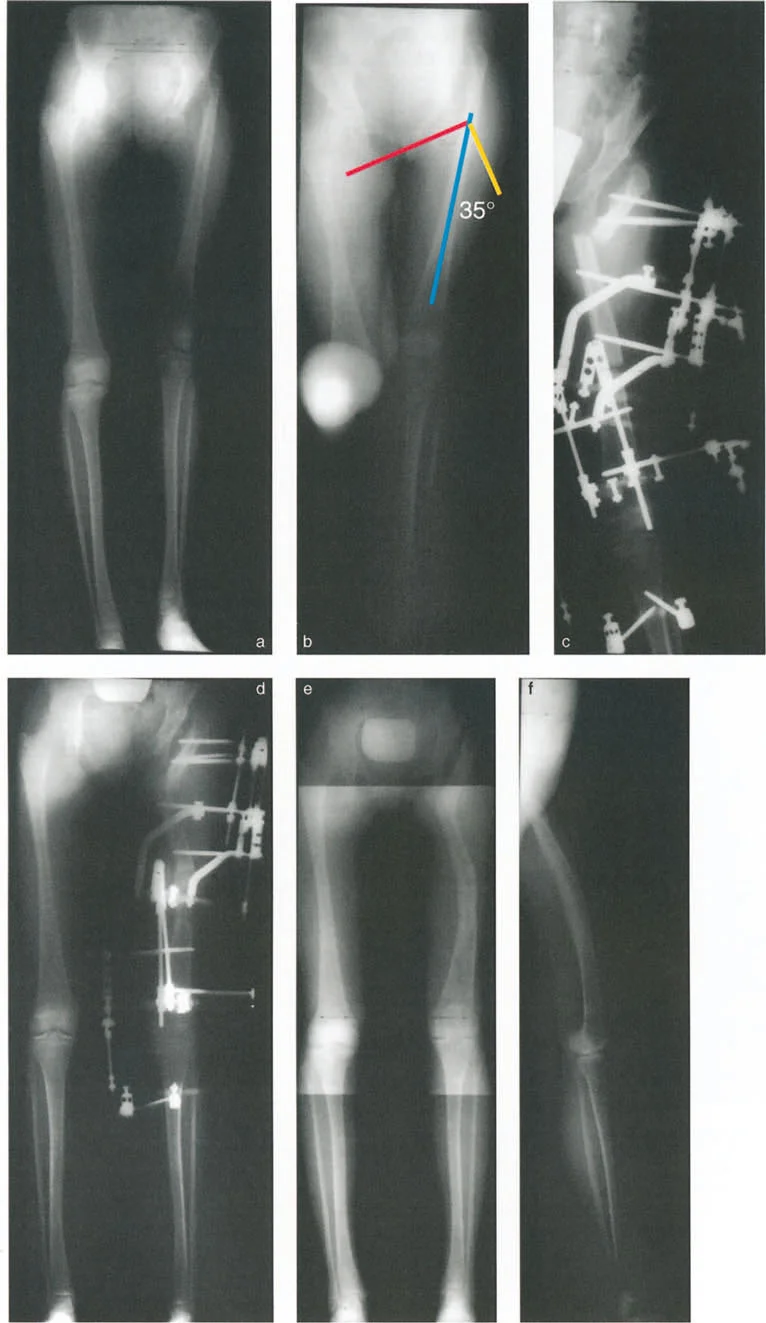
- Assess the Resulting Mechanical Axis After simulating the proximal valgus draw a new line from the center of the knee joint up through the newly angled proximal femur. You will observe that the mechanical axis is now severely deviated laterally creating a massive valgus deformity at the knee.
- Locate the Distal CORA Draw the ideal Proximal Mechanical Axis dropping perpendicularly from the horizontal pelvic line. Extend the Distal Mechanical Axis up from the center of the ankle through the center of the knee. The intersection of these two lines dictates the exact location and magnitude of the distal varus osteotomy required to neutralize the mechanical axis.
- Plan the Distal Osteotomy The distal osteotomy is typically located in the distal third of the femur. The magnitude of the varus correction here must perfectly offset the lateral deviation caused by the proximal valgus. Furthermore this distal site will serve as the primary zone for distraction osteogenesis to correct the limb length discrepancy.
Key Takeaways for Radiographic Planning
* The proximal osteotomy is an acute valgus and extension correction.
* The distal osteotomy is a gradual varus correction combined with lengthening.
* Failure to accurately calculate the distal varus will result in persistent knee malalignment and early joint degeneration.
Surgical Execution of the Pelvic Support Osteotomy
The surgical execution of the double level pelvic support osteotomy is highly demanding and requires mastery of external fixation techniques specifically the Ilizarov apparatus or hexapod systems like the Taylor Spatial Frame.
Proximal Valgus Extension Osteotomy
The patient is positioned supine on a radiolucent Jackson table or fracture table. Fluoroscopy is utilized throughout the procedure.
- Frame Application A specialized femoral frame is constructed. The proximal segment typically consists of a 90 degree or 120 degree arch positioned laterally to accommodate the torso. This arch is secured to the proximal femur using multiple hydroxyapatite coated half pins.
- Pin Placement Care must be taken to place the proximal pins superior to the planned osteotomy site avoiding the neurovascular bundle anteriorly and the sciatic nerve posteriorly.
- The Proximal Osteotomy A percutaneous or minimally invasive corticotomy is performed at the pre planned level usually just distal to the lesser trochanter or at the level of the ischial tuberosity.
- Acute Correction The proximal femur is acutely angulated into the pre calculated valgus and extension. The extension component is critical to correct the flexion contracture that invariably accompanies a chronically dislocated hip. The frame hinges are locked to secure this acute correction.
Distal Varus Lengthening Osteotomy
Once the proximal support is established attention turns to the distal femur.
- Distal Frame Application Full rings are applied to the distal femur and secured with tensioned wires and half pins. The distal rings are connected to the proximal arch using threaded rods or hexapod struts.
- The Distal Osteotomy A second corticotomy is performed in the distal metadiaphyseal region of the femur. This must be a low energy osteotomy utilizing multiple drill holes and an osteotome to preserve the endosteal blood supply and periosteal sleeve which is vital for successful distraction osteogenesis.
- Frame Linkage The frame is finalized ensuring that the hinges or struts are perfectly aligned with the distal CORA to allow for gradual varus correction and longitudinal distraction.
Postoperative Protocol and Distraction Osteogenesis
The postoperative phase is just as critical as the surgical execution. The success of the distal osteotomy relies on the biological principles of tension stress discovered by Ilizarov.
Latency Phase
Following surgery a latency period of 7 to 10 days is observed. This allows the acute inflammatory phase of fracture healing to subside and the initial soft callus to form at the distal corticotomy site.
Distraction Phase
Distraction is initiated at a rate of approximately 1 millimeter per day divided into four increments of 0.25 millimeters. During this phase the hexapod struts or Ilizarov rods are adjusted daily by the patient to gradually induce varus and lengthen the femur.
Close radiographic monitoring is required every 10 to 14 days to assess the quality of the regenerate bone. If the regenerate appears too lucent the distraction rate is slowed. If premature consolidation is threatened the rate is increased.
Physical Therapy
Aggressive physical therapy is mandatory throughout the distraction phase. Lengthening the femur places immense tension on the quadriceps specifically the rectus femoris and the iliotibial band. Without daily stretching severe knee flexion contractures and joint subluxation can occur.
Consolidation Phase
Once the target length and mechanical axis alignment are achieved the frame is locked. The consolidation phase begins during which the regenerate bone mineralizes and hardens. This phase typically takes twice as long as the distraction phase. The external fixator is only removed when circumferential corticalization of the regenerate is visible on orthogonal radiographs.
Complications and Advanced Management Strategies
The double level pelvic support osteotomy is a massive undertaking with a high complication profile. Surgeons must be prepared to manage these issues proactively.
Pin Site Infections
Superficial pin site infections are almost universal during prolonged external fixation. They are managed with oral antibiotics and aggressive local pin care. Deep infections requiring pin removal and exchange are rare but must be addressed immediately to prevent osteomyelitis or loss of frame stability.
Joint Contractures
Knee stiffness is the most common functional complication. The tension generated by lengthening the femur pulls tightly across the knee joint. If physical therapy fails to maintain range of motion the distraction must be temporarily halted. In severe cases surgical release of the iliotibial band or quadriceps lengthening may be required.
Premature Consolidation and Delayed Union
If the distraction rate is too slow the bone may heal prematurely requiring a return to the operating room for a repeat corticotomy. Conversely if the regenerate is poor delayed union occurs. This is managed by the accordion maneuver where the distraction is reversed compressing the regenerate for a few days to stimulate osteogenesis before resuming lengthening.
Neurologic Injury
Stretching the limb can lead to neuropraxia most commonly affecting the peroneal or sciatic nerves. Patients must be monitored daily for changes in sensation or motor function such as foot drop. If nerve palsy develops distraction is immediately stopped and the limb is slightly shortened to relieve tension on the nerve until function returns.
By adhering strictly to Paley principles of deformity correction and executing the Ilizarov double level technique meticulously surgeons can successfully navigate these complications. The Pelvic Support Osteotomy remains a masterclass in orthopedic biomechanics offering a life changing functional restoration for patients with otherwise unsalvageable hip pathology.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like