Mastering Proximal Femoral Osteotomies: Paley's Principles & Hip Biomechanics
Key Takeaway
Proximal femoral osteotomies correct hip deformities by altering femoral geometry. Applying Paley's principles, surgeons address the complex interplay between anatomical and mechanical axes, crucial for conditions like coxa vara, to restore optimal hip biomechanics and prevent complications.
Comprehensive Guide to Proximal Femoral Osteotomies
The hip joint is a highly constrained multi axial ball and socket joint that relies on a precise balance of osseous geometry ligamentous stability and dynamic muscular forces. Deformities of the proximal femur whether congenital developmental or post traumatic profoundly alter the biomechanics of the hip. These alterations not only affect the hip joint itself but also have cascading effects on the mechanical axis of the entire lower extremity altering loads transmitted across the knee and ankle.
When addressing proximal femoral deformities particularly coxa vara or non unions of the femoral neck the orthopaedic surgeon must navigate the complex interplay between the anatomical axis of the femur and the mechanical axis of the lower limb. Correcting one without regard for the other often leads to iatrogenic complications such as joint impingement abductor weakness or accelerated osteoarthritis in adjacent joints.
This comprehensive guide delves deeply into the principles of proximal femoral deformity correction emphasizing the critical distinctions between mechanical and anatomical alignment the application of Paleys principles and the specific execution of the valgus lateral translation osteotomy.
Mastering Paleys Principles for the Proximal Femur
To understand the rationale behind complex proximal femoral osteotomies one must first master the standard radiographic parameters defined by Dr Dror Paley. The proximal femur is unique because its anatomical axis does not align with the mechanical axis of the lower extremity. This offset creates specific biomechanical challenges that require meticulous preoperative planning.
The mechanical axis of the lower extremity is defined by a line drawn from the center of the femoral head to the center of the ankle joint. In a normally aligned limb this line passes precisely through the center of the knee joint. Any deviation from this center point is referred to as Mechanical Axis Deviation.
Essential Radiographic Parameters and Joint Angles
When evaluating the hip and planning an osteotomy several specific joint orientation angles must be measured. These angles dictate the magnitude and location of the surgical correction.
| Radiographic Parameter | Definition | Normal Range | Clinical Significance |
|---|---|---|---|
| NSA (Neck Shaft Angle) | The anatomical angle formed by the intersection of the anatomical axis of the femoral shaft and the axis of the femoral neck. | 130° to 135° | Determines the anatomical relationship of the proximal femur. Abnormalities lead to coxa vara or coxa valga. |
| MPFA (Mechanical Proximal Femoral Angle) | Formed by the mechanical axis of the femur and a line drawn from the tip of the greater trochanter to the center of the femoral head. | 84° to 90° | Dictates the mechanical alignment of the proximal femur relative to the weight bearing axis. |
| mLDFA (Mechanical Lateral Distal Femoral Angle) | Formed by the mechanical axis of the femur and the joint line of the distal femur. | 85° to 90° | Crucial for ensuring distal femoral alignment is normal before attributing mechanical axis deviation solely to the hip. |
| MPTA (Medial Proximal Tibial Angle) | Formed by the mechanical axis of the tibia and the proximal tibial joint line. | 85° to 90° | Evaluates concurrent tibial deformities that may contribute to overall limb malalignment. |
| JLCA (Joint Line Convergence Angle) | The angle between the distal femoral joint line and the proximal tibial joint line. | 0° to 2° | Assesses ligamentous laxity or intra articular deformity at the knee. |
Defining MAD and CORA
Two foundational concepts in Paleys approach to deformity correction are the Mechanical Axis Deviation and the Center of Rotation of Angulation.
The Mechanical Axis Deviation is the perpendicular distance from the center of the knee joint to the mechanical axis line. A medial deviation indicates varus alignment of the limb increasing compressive forces on the medial compartment of the knee. A lateral deviation indicates valgus alignment overloading the lateral compartment.
The Center of Rotation of Angulation is the specific point where the proximal and distal axes of a deformed bone intersect. In proximal femoral deformities the CORA is often located intra articularly or within the femoral neck making a direct osteotomy at the CORA surgically impossible or biologically detrimental. This anatomical limitation forms the basis for Paleys Osteotomy Rules which will be discussed in detail.
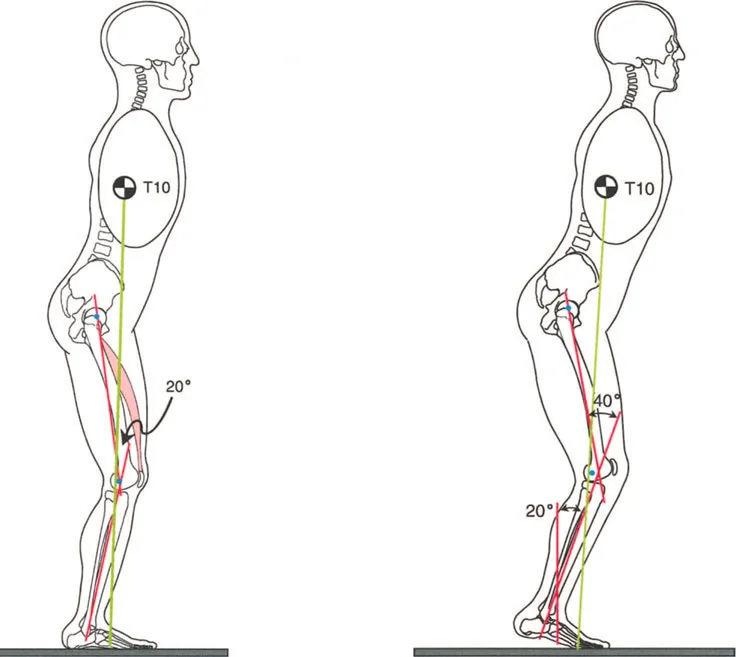
Biomechanical Conflict in Coxa Vara
Coxa vara is defined as a reduction in the Neck Shaft Angle to less than 120 degrees. Biomechanically this deformity drastically alters the force vectors acting across the hip joint and the proximal femur.
The primary structural consequence of coxa vara is an exponential increase in the bending moment across the femoral neck. As the femoral neck becomes more horizontal the compressive forces of weight bearing are converted into shear forces. This altered biomechanical environment heavily predisposes the patient to fatigue fractures hardware failure and recalcitrant non unions of the femoral neck.
Paradoxically coxa vara increases the abductor lever arm. The greater trochanter is displaced laterally and superiorly which can theoretically reduce the overall joint reactive force by giving the gluteus medius a mechanical advantage. However this advantage is almost always negated by the resulting limb shortening and altered gait mechanics. The superior migration of the greater trochanter often leads to relative lengthening of the abductor musculature causing tension loss and a subsequent positive Trendelenburg sign.
The primary surgical challenge in correcting coxa vara is the discrepancy between the anatomical correction and the mechanical correction. Because the center of rotation of the hip joint is offset from the femoral shaft a purely angular correction of the proximal femur will invariably translate the mechanical axis of the entire limb.
Detailed Image Analysis Anatomical Versus Mechanical Dilemma
To perfectly illustrate the complexity of proximal femoral correction we must examine the relationship between the Neck Shaft Angle and the Mechanical Proximal Femoral Angle during surgical planning.
The provided diagram outlines distinct scenarios that highlight the critical decision making process in hip joint deformity correction. Understanding these scenarios is paramount for any orthopedic surgeon attempting to reconstruct the proximal femur.
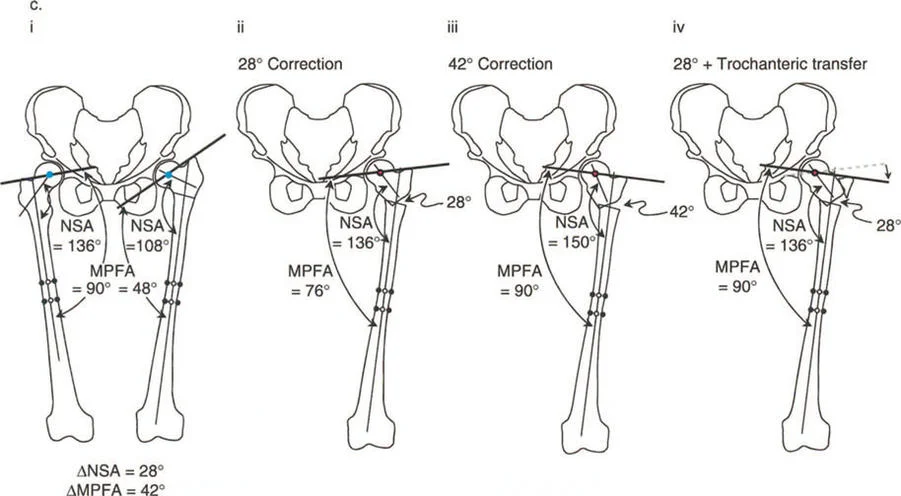
Scenario One The Preoperative Deformity
In figure i we observe a bilateral comparison. The normal right hip demonstrates a normal Neck Shaft Angle of 136 degrees and a normal Mechanical Proximal Femoral Angle of 90 degrees. The pathological left hip exhibits severe coxa vara. The Neck Shaft Angle is reduced to 108 degrees and the Mechanical Proximal Femoral Angle is drastically reduced to 48 degrees.
The angular difference between the normal and abnormal Neck Shaft Angle is 28 degrees. However the difference between the normal and abnormal Mechanical Proximal Femoral Angle is 42 degrees. This mathematical discrepancy is the crux of proximal femoral osteotomy planning. The angular deformity of the neck does not match the angular deviation of the mechanical axis.
Scenario Two Pure Anatomical Correction
If the surgeon chooses to perform a 28 degree valgus osteotomy they successfully restore the anatomical Neck Shaft Angle to a normal 136 degrees. This is depicted in figure ii. The proximal femur looks anatomically correct on a localized radiograph.
However looking at the mechanical axis the Mechanical Proximal Femoral Angle only improves to 76 degrees. The patient is left with a residual mechanical varus of the proximal femur. This under correction of the mechanical axis will result in a medial Mechanical Axis Deviation at the knee. Over time this medial shift of the weight bearing axis will lead to asymmetric cartilage wear and medial compartment osteoarthritis of the knee. The surgeon has fixed the bone but failed the limb.
Scenario Three Pure Mechanical Correction
Conversely if the surgeon decides to prioritize the mechanical axis and performs a 42 degree valgus osteotomy to restore the Mechanical Proximal Femoral Angle to a perfect 90 degrees a new biomechanical disaster arises.
As seen in figure iii the anatomical Neck Shaft Angle is over corrected to 150 degrees creating severe iatrogenic coxa valga. Coxa valga drastically shortens the abductor lever arm by medializing the greater trochanter. This leads to profound abductor weakness a severe positive Trendelenburg gait and potentially lateral hip impingement. Furthermore the mechanical axis is shifted laterally and the joint reactive forces are concentrated on a smaller surface area of the superior acetabulum accelerating joint degeneration and increasing the risk of avascular necrosis.
Scenario Four The Paley Solution
The ultimate goal is to restore both the anatomical Neck Shaft Angle and the mechanical Mechanical Proximal Femoral Angle simultaneously. Because the angular differences are not equal a simple opening or closing wedge osteotomy is insufficient.
The solution requires the application of Paleys Osteotomy Rules specifically combining angular correction with lateral translation of the distal shaft. By performing a valgus producing osteotomy and translating the distal femoral shaft laterally the surgeon can restore the Neck Shaft Angle to 136 degrees while simultaneously shifting the mechanical axis laterally to restore the Mechanical Proximal Femoral Angle to 90 degrees. This is known as the Valgus Lateral Translation Osteotomy.
Applying Paleys Osteotomy Rules to the Hip
Dr Dror Paley established three fundamental rules of deformity correction that govern the relationship between the osteotomy site the Center of Rotation of Angulation and the resulting mechanical axis. Applying these rules is non negotiable for successful proximal femoral reconstructions.
Osteotomy Rule One
Rule One states that if the osteotomy and the hinge of the correction are placed exactly at the Center of Rotation of Angulation pure angulation will perfectly realign the mechanical axis without causing any translation.
In the proximal femur the Center of Rotation of Angulation for coxa vara is typically located within the femoral head or the femoral neck. Performing an osteotomy at this exact location is usually impossible due to the risk of avascular necrosis disruption of the joint capsule and lack of adequate bone stock for fixation. Therefore Rule One is rarely applicable in proximal femoral deformity correction.
Osteotomy Rule Two
Rule Two states that if the osteotomy is performed at a level different from the Center of Rotation of Angulation but the hinge of correction remains at the Center of Rotation of Angulation the correction will require both angulation and translation to realign the mechanical axis perfectly.
This is the guiding principle for the Valgus Lateral Translation Osteotomy. The surgeon makes the bone cut at the intertrochanteric or subtrochanteric level which is distal to the true Center of Rotation of Angulation. To prevent the mechanical axis from deviating medially the distal femoral segment must be translated laterally as the valgus angulation is applied. This simultaneous angulation and translation satisfies both the anatomical and mechanical requirements of the limb.
Osteotomy Rule Three
Rule Three serves as a warning. It states that if the osteotomy and the hinge of correction are both placed at a level different from the Center of Rotation of Angulation pure angulation will result in a parallel translation of the mechanical axis creating an iatrogenic deformity.
This is exactly what occurs in Scenario Two and Scenario Three of our image analysis. By performing a pure angular correction at the subtrochanteric level without compensatory translation the surgeon inevitably creates a Mechanical Axis Deviation at the knee. Rule Three highlights the danger of ignoring the spatial relationship between the osteotomy site and the Center of Rotation of Angulation.
Step by Step Preoperative Planning
Meticulous preoperative planning is the cornerstone of a successful proximal femoral osteotomy. Surgeons must transition from viewing localized hip radiographs to analyzing full length standing weight bearing films.
- Obtain Proper Imaging Acquire full length standing anteroposterior radiographs of both lower extremities with the patellae facing strictly forward. Obtain dedicated AP and lateral views of the affected hip.
- Draw the Mechanical Axis Draw a line from the center of the normal femoral head to the center of the normal ankle to establish the baseline mechanical axis. Repeat this on the deformed side.
- Measure Joint Orientation Angles Calculate the Neck Shaft Angle the Mechanical Proximal Femoral Angle and the Mechanical Lateral Distal Femoral Angle on both the normal and deformed sides. Identify the exact magnitude of the angular discrepancies.
- Locate the CORA Draw the proximal anatomical axis through the center of the femoral neck. Draw the distal anatomical axis through the center of the femoral diaphysis. The intersection of these two lines is the anatomical Center of Rotation of Angulation.
- Determine the Osteotomy Level Select an osteotomy site that allows for optimal bone healing and hardware placement typically at the intertrochanteric or high subtrochanteric level.
- Calculate Required Translation Because the osteotomy is distal to the Center of Rotation of Angulation calculate the exact amount of lateral translation required to realign the mechanical axis with the center of the knee joint. This can be done using digital templating software or manual trigonometric calculations.
- Plan Hardware Placement Template the fixation device whether it is a fixed angle blade plate a locking proximal femoral plate or a monolateral external fixator. Ensure the proximal fixation has adequate purchase in the femoral head and neck without violating the joint space.
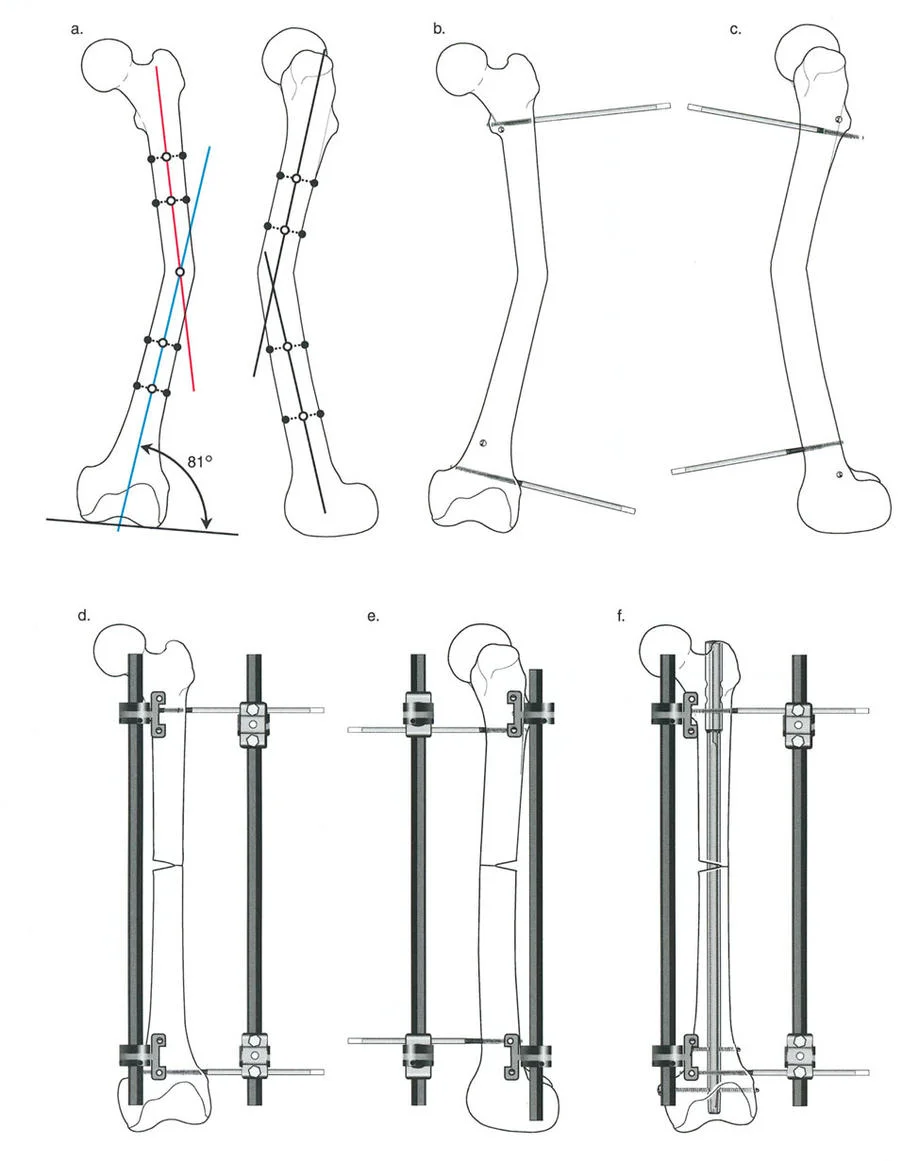
Surgical Execution of Valgus Lateral Translation Osteotomy
The execution of the valgus lateral translation osteotomy requires absolute precision. While internal fixation with blade plates or locking plates is common the use of external fixation offers unparalleled intraoperative adjustability and the ability to fine tune the correction postoperatively.
Patient Positioning and Setup
The patient is placed supine on a radiolucent operating table or a fracture table. Fluoroscopy must be positioned to provide unhindered AP and lateral views of the proximal femur down to the knee joint. The entire lower extremity is prepped and draped free to allow for intraoperative assessment of limb alignment and range of motion.
Proximal Fixation Strategy
If utilizing an external fixator or a fixed angle device the proximal trajectory is the most critical step. The proximal pins or the blade of the plate must be inserted into the femoral neck and head at an angle that anticipates the final correction.
For a valgus producing osteotomy the proximal fixation is inserted at an angle equal to the planned angular correction relative to the final desired position. For example if a 30 degree valgus correction is planned the proximal fixation is inserted 30 degrees more horizontal than its final intended resting angle. This ensures that when the distal fragment is brought into alignment with the fixation device the proximal fragment is forced into exactly 30 degrees of valgus.
Performing the Osteotomy
The osteotomy is typically performed using a multiple drill hole technique followed by an osteotome or a specialized oscillating saw equipped with saline cooling to prevent thermal necrosis. The cut is made at the pre planned intertrochanteric or subtrochanteric level.
Care must be taken to preserve the medial periosteal hinge if possible as this enhances stability and promotes rapid callus formation. However because lateral translation is required the medial cortex will often be completely displaced.
Achieving Translation and Compression
Once the bone is divided the distal femoral shaft is abducted to meet the fixation device achieving the planned valgus angulation. Simultaneously the distal fragment must be physically translated laterally.
This translation is often the most technically demanding portion of the procedure. It requires releasing tight medial fascial structures and utilizing bone holding forceps or the external fixator itself to slide the distal fragment laterally along the osteotomy plane.
Once the desired angulation and translation are achieved the osteotomy site is compressed. Compression increases the stability of the construct maximizes bone to bone contact and accelerates primary bone healing. Fluoroscopy is used to confirm the restoration of the Neck Shaft Angle and a cautery cord is stretched from the center of the femoral head to the center of the ankle to verify that the mechanical axis now passes through the center of the knee.
Managing Limb Length Discrepancy
Proximal femoral deformities are almost universally accompanied by limb length discrepancies. Coxa vara inherently shortens the limb due to the decreased vertical height of the femoral neck.
A valgus producing osteotomy naturally provides a degree of limb lengthening. By verticalizing the femoral neck the surgeon restores the lost height of the proximal femur. The exact amount of lengthening achieved is a trigonometric function of the magnitude of the angular correction and the length of the femoral neck.
However if a significant limb length discrepancy persists after the angular correction is planned the surgeon must incorporate a lengthening strategy. If using an external fixator the osteotomy can be gradually distracted postoperatively using the principles of distraction osteogenesis. If using internal fixation a concurrent distal femoral or proximal tibial lengthening may be required or the patient may be managed with a shoe lift if the discrepancy is minor.
Clinical Pearls for Proximal Femoral Reconstruction
To achieve consistent exceptional results orthopedic surgeons should internalize the following high yield clinical pearls.
- Never Ignore the Knee Always evaluate the mechanical axis down to the ankle. Correcting a hip deformity without assessing the Mechanical Lateral Distal Femoral Angle or the Medial Proximal Tibial Angle can unmask or exacerbate distal deformities.
- Translation is Mandatory When performing a valgus osteotomy for coxa vara at the subtrochanteric level lateral translation of the distal fragment is an absolute biomechanical requirement to prevent medial Mechanical Axis Deviation.
- Respect the Abductors Over correcting the Neck Shaft Angle into coxa valga will destroy abductor mechanics. Always prioritize restoring the normal abductor lever arm to prevent a permanent Trendelenburg gait.
- Template the Hardware The geometry of the proximal femur is highly variable. Preoperative templating of blade plates or locking plates is essential to ensure the hardware will physically fit within the confines of the femoral neck after translation is achieved.
- Consider Prophylactic Fixation In cases of severe osteoporosis or metabolic bone disease consider extending fixation distally or utilizing intramedullary devices to prevent stress risers and subsequent peri implant fractures.
- Assess the Sagittal Plane Proximal femoral deformities are rarely uniplanar. Always assess for concurrent flexion or extension deformities (procurvatum or recurvatum) and rotational malalignment. The osteotomy must address all three dimensions simultaneously.
Avoiding Iatrogenic Complications
The margin for error in proximal femoral osteotomies is exceptionally narrow. Complications arise primarily from a failure to adhere to Paleys principles during the planning phase.
Failure of Fixation
Failure of fixation is commonly caused by inadequate proximal purchase or failure to achieve cortical contact at the osteotomy site. The bending forces across the proximal femur are massive. If the osteotomy is left distracted or if the medial cortex is not rigidly compressed the hardware will eventually experience fatigue failure. Utilizing a lateral tension band plate combined with medial cortical compression is the most biomechanically sound construct.
Joint Impingement
Altering the geometry of the proximal femur changes the spatial relationship between the femoral neck and the acetabular rim. Excessive valgus correction can lead to lateral impingement of the greater trochanter against the ilium. Conversely failing to correct retroversion during the osteotomy can exacerbate anterior femoroacetabular impingement. Surgeons must dynamically assess hip range of motion intraoperatively after provisional fixation is applied.
Non Union and Delayed Union
The subtrochanteric region is composed primarily of cortical bone which heals slower than the cancellous bone of the intertrochanteric region. Thermal necrosis during the bone cut excessive periosteal stripping and inadequate stability are the primary culprits for non union. Utilizing low speed drills sharp osteotomes and preserving the soft tissue envelope are critical steps to ensure biological healing.
Conclusion
The correction of proximal femoral deformities requires a profound understanding of lower extremity biomechanics and a meticulous adherence to the principles of deformity correction. The interplay between the anatomical Neck Shaft Angle and the mechanical Mechanical Proximal Femoral Angle creates a unique surgical challenge that cannot be solved by simple angular osteotomies.
By applying Paleys Osteotomy Rules and mastering the execution of the valgus lateral translation osteotomy orthopaedic surgeons can successfully navigate the anatomical versus mechanical dilemma. This comprehensive approach ensures not only the restoration of localized hip anatomy but also the preservation of the mechanical axis safeguarding the knee and ankle joints from accelerated degeneration and providing the patient with a biomechanically optimized lower extremity.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like