Chapter 64: · AnkleandFootConsiderations
Comprehensive Introduction to Foot and Ankle Deformities
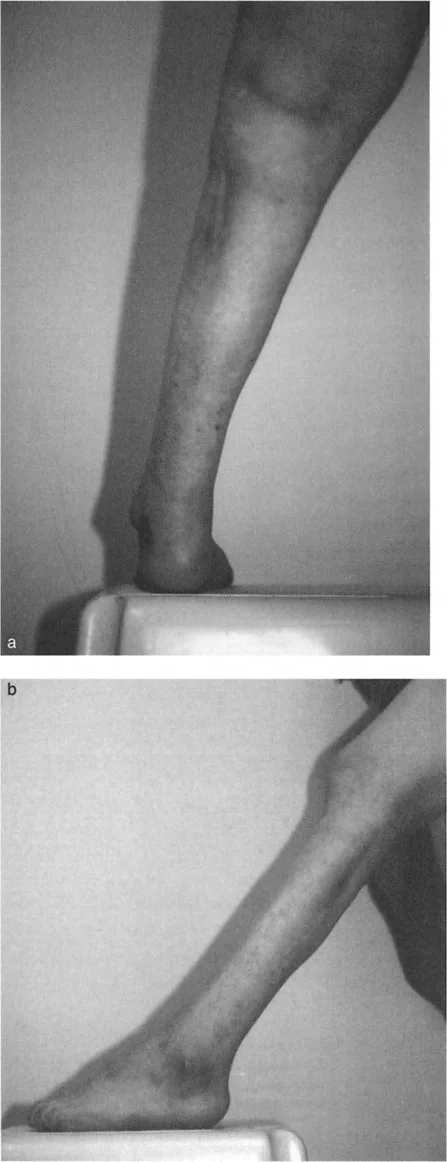
The management of complex foot and ankle deformities requires a profound understanding of lower extremity kinematics, soft tissue constraints, and osseous architecture. Equinus contracture, one of the most ubiquitous and challenging deformities encountered by the orthopedic surgeon, rarely exists in isolation. It frequently presents as a composite deformity involving the hindfoot, midfoot, and forefoot, necessitating a systematic and highly analytical approach to both diagnosis and surgical intervention.
The pathoepidemiology of these deformities spans a wide spectrum of etiologies. These include congenital anomalies such as clubfoot and arthrogryposis multiplex congenita, post-traumatic malunions, neuromuscular disorders including cerebral palsy, Charcot-Marie-Tooth disease, and poliomyelitis, and iatrogenic sequelae from prior surgical interventions.
Historically, the treatment paradigm for severe equinus and combined equinovarus deformities relied heavily on extensive, radical soft tissue releases and joint-sacrificing arthrodeses. While these techniques remain in the surgical armamentarium for specific salvage scenarios, the advent of distraction histiogenesis and the application of Ilizarov principles have revolutionized the management of these complex cases. The ability to gradually distract contracted soft tissues and simultaneously correct osseous malalignment has significantly reduced the need for radical resections, thereby preserving joint mobility and minimizing the risk of catastrophic neurovascular compromise.
Pathoepidemiology and Clinical Burden
The epidemiological burden of these deformities is significant, particularly in tertiary referral centers specializing in limb reconstruction. Post-traumatic malunions of the tibia and fibula, often accompanied by shortening of the fibula relative to the tibia, frequently result in secondary equinovalgus or equinovarus deformities. The incidence of post-traumatic equinus has risen concurrently with the increasing survival rates of high-energy trauma patients.
Furthermore, the chronicity of these deformities leads to secondary adaptive changes in the articular cartilage and surrounding soft tissues, including the neurovascular bundles. Chronic equinus contractures subject the midfoot to abnormal loading forces, often precipitating midfoot arthritis, plantar fasciitis, and intractable plantar keratoses.
The Four Pillars of Equinus Deformity
Understanding the precise anatomical locus of the deformity is paramount, as a clinical presentation of equinus may stem from four distinct pathological entities. Differentiating between these four distinct causes is the cornerstone of successful reconstructive surgery.
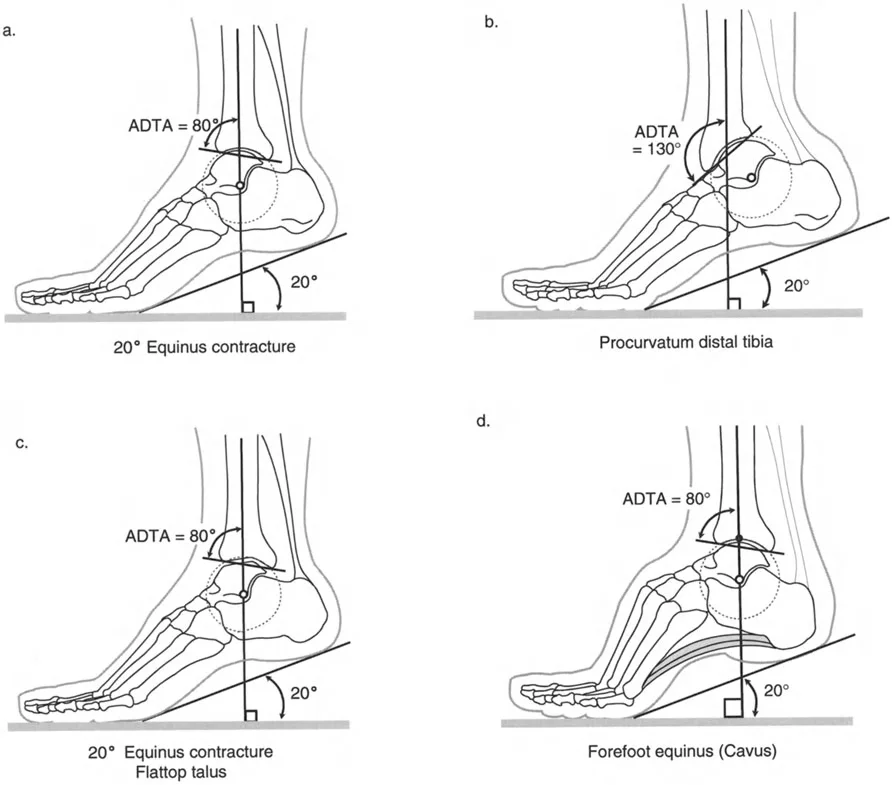
True Ankle Contracture
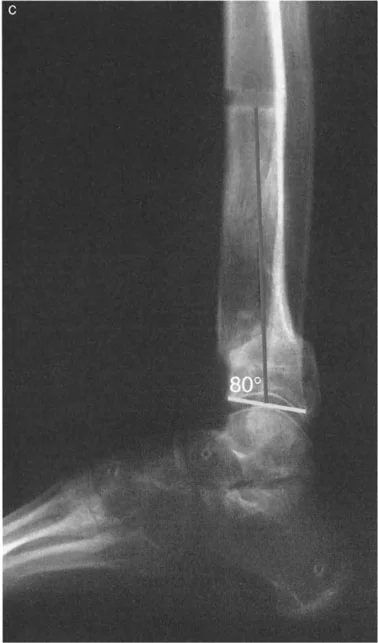
A true ankle contracture involves a tight Achilles tendon-gastrocnemius-soleus complex and posterior capsular restriction. Radiographically, this presents with a normal Anterior Distal Tibial Angle (ADTA) of approximately 80 degrees, a spherical talar dome, and no forefoot cavus. The mechanical block is entirely soft tissue in origin, restricting the talus from rotating dorsally within the mortise.
Distal Tibial Procurvatum
Conversely, a procurvatum deformity of the distal tibia presents with an abnormally high ADTA, which can frequently exceed 100 to 130 degrees. This osseous malalignment causes the talar neck to impinge prematurely on the anterior tibial plafond during attempted dorsiflexion. Clinically, this mimics a soft tissue equinus, but aggressive soft tissue release will fail to improve range of motion because the block is osseous.

Flattop Talus
A flattop talus is often a sequela of avascular necrosis, repetitive microtrauma, or prior talar neck fractures. It presents with a normal ADTA but a flattened talar dome that mechanically restricts dorsiflexion due to altered joint congruency. The normal radius of curvature of the talus is lost, preventing smooth articulation beneath the tibial plafond.
Forefoot Equinus and Cavus Deformity
Forefoot equinus, or cavus deformity, presents with a plantarflexed midfoot and forefoot relative to the hindfoot. While the ankle joint itself may possess normal dorsiflexion, the clinical posture of the foot mimics a rigid equinus. This is frequently driven by neuromuscular imbalances, such as an overactive peroneus longus overpowering the tibialis anterior, leading to plantarflexion of the first ray and subsequent compensatory hindfoot varus.

Surgical Pearls for Differentiating Equinus
* Always perform the Silfverskiöld test to differentiate isolated gastrocnemius tightness from combined gastrocnemius-soleus contracture.
* Assess ankle dorsiflexion with the knee extended and flexed, but also with the forefoot inverted to lock the transverse tarsal joint, isolating true tibiotalar motion.
* Weight-bearing lateral radiographs are mandatory to assess the ADTA and talar morphology.
Paley Principles in Foot and Ankle Reconstruction
The foundational principles developed by Dr. Dror Paley are essential for the systematic analysis and correction of lower extremity deformities. Applying these principles to the foot and ankle requires an understanding of the Mechanical Axis Deviation (MAD), Joint Orientation Angles, and the Center of Rotation of Angulation (CORA).
Joint Orientation Angles of the Ankle
Accurate deformity correction begins with defining the normal joint orientation angles. The mechanical axis of the tibia must be perfectly aligned to distribute forces evenly across the talar dome.
Key radiographic parameters include:
* Mechanical Lateral Distal Tibial Angle (mLDFA): The normal mLDFA is 89 degrees (range 86 to 92 degrees). This angle dictates the coronal plane alignment of the ankle mortise. An abnormal mLDFA indicates a supramalleolar varus or valgus deformity.
* Anterior Distal Tibial Angle (ADTA): The normal ADTA is 80 degrees (range 78 to 82 degrees). Measured on the lateral radiograph, it dictates sagittal plane alignment.
* Joint Line Convergence Angle (JLCA): In the ankle, this represents the talocrural angle. Widening of the medial or lateral clear space indicates syndesmotic injury or ligamentous incompetence, altering the JLCA.
| Radiographic Parameter | Normal Value | Clinical Significance |
|---|---|---|
| mLDFA | 89 degrees | Coronal plane tibial alignment (Varus/Valgus) |
| ADTA | 80 degrees | Sagittal plane tibial alignment (Procurvatum/Recurvatum) |
| Calcaneal Pitch | 20 to 30 degrees | Sagittal hindfoot alignment (Pes Cavus/Planus) |
| Meary Angle | 0 degrees | Sagittal midfoot alignment (Talo-first metatarsal axis) |
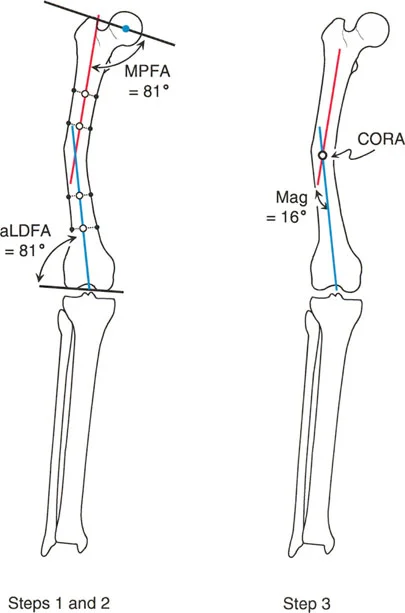
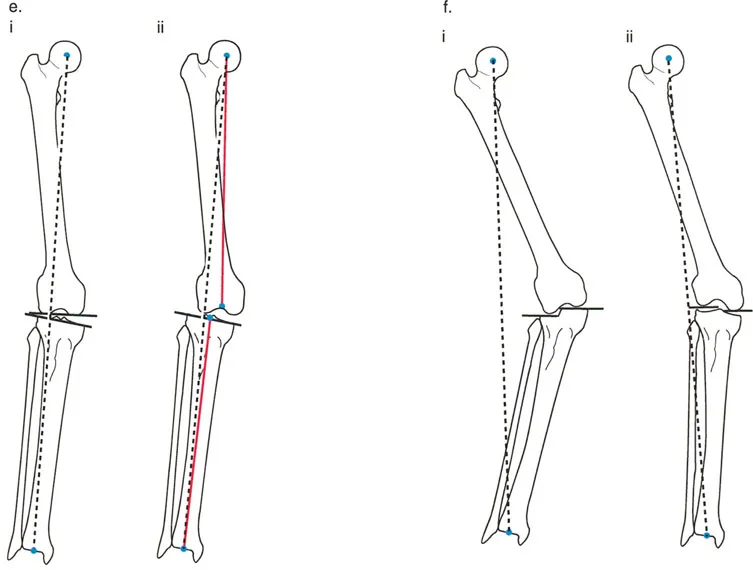
Calculating the Center of Rotation of Angulation
The CORA is the point at which the proximal and distal mechanical or anatomical axes intersect. In the context of ankle and foot considerations, identifying the CORA is critical for determining whether a deformity is intra-articular, peri-articular, or diaphyseal.
To calculate the CORA for a supramalleolar deformity:
1. Draw the mid-diaphyseal line of the proximal tibial segment.
2. Draw the joint orientation line of the distal tibial plafond.
3. Project a line proximally from the joint line at the normal mLDFA (89 degrees) or ADTA (80 degrees).
4. The intersection of these two lines is the CORA.
If the CORA is located at the level of the joint line, the deformity is intra-articular or involves a joint contracture. If the CORA is proximal to the joint line, the deformity is osseous and located within the tibia.
Applying the Osteotomy Rules
Dr. Paley established three fundamental osteotomy rules that dictate how bone cuts should be made relative to the CORA to achieve optimal alignment without inducing secondary translation.
- Osteotomy Rule 1: When the osteotomy and the hinge (axis of correction) are both placed at the CORA, angulation is corrected without translation. The mechanical axis is fully restored.
- Osteotomy Rule 2: When the hinge is placed at the CORA, but the osteotomy is performed at a different level, the angulation is corrected, but translation occurs at the osteotomy site. This is highly useful in the distal tibia when poor skin quality prevents an incision directly over the CORA.
- Osteotomy Rule 3: When the osteotomy and the hinge are placed away from the CORA, a secondary translation deformity is induced. This is generally avoided unless purposefully utilized to correct a pre-existing translational deformity.
Surgical Anatomy and Biomechanical Considerations
The surgical anatomy of the ankle and foot is a marvel of biomechanical engineering, characterized by a highly congruent osseous mortise stabilized by a robust network of ligaments and dynamic musculotendinous units.
The Osseous Mortise and Distal Tibia
The ankle joint, a modified hinge joint, derives its stability from the precise articulation of the talar dome within the mortise formed by the distal tibia and the medial and lateral malleoli. The ADTA is a critical radiographic parameter dictating the spatial orientation of the tibial plafond in the sagittal plane.
Any deviation from this anatomical norm fundamentally alters the biomechanics of the joint. For instance, in a procurvatum deformity where the ADTA increases significantly, the anterior impingement of the talar neck against the tibia leads to a consequent loss of dorsiflexion. Furthermore, the presence of anterior osteophytes on the tibia or within the dorsal sulcus of the talus can create a mechanical block, necessitating meticulous osseous resection to restore normal kinematics.
When performing supramalleolar osteotomies, the surgeon must respect the distal tibiofibular syndesmosis. If a tibial osteotomy requires significant angular correction, a concomitant fibular osteotomy is almost always required to prevent syndesmotic disruption or restricted correction.
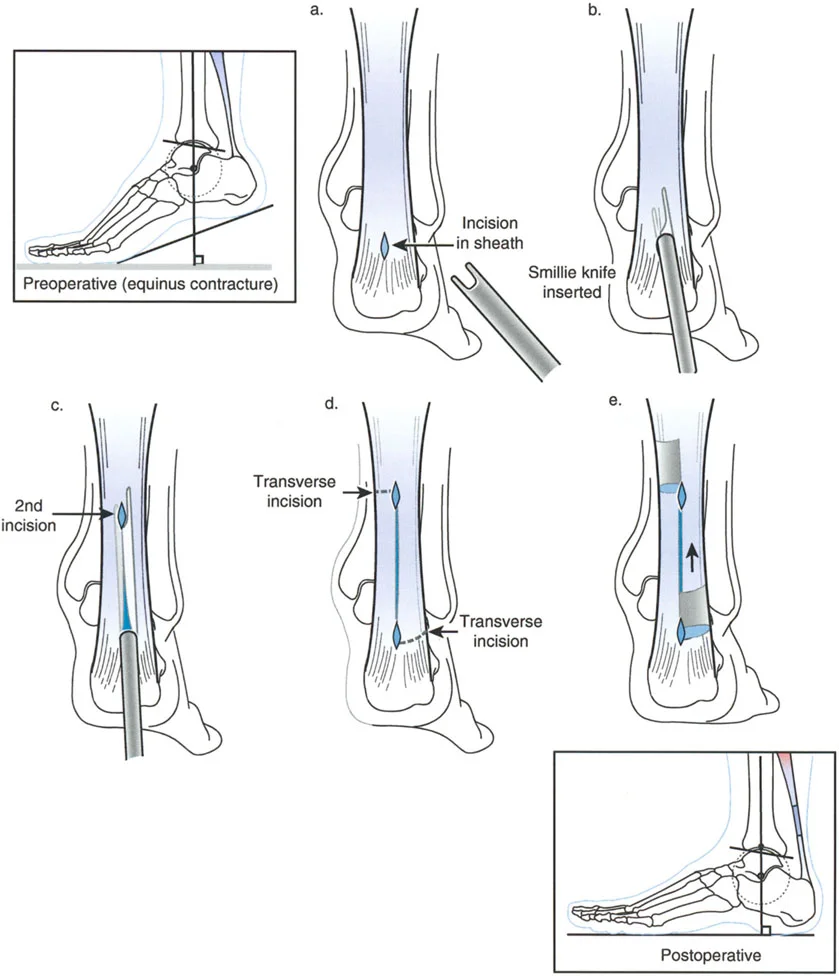
Soft Tissue Envelope and the Achilles Complex
The soft tissue envelope of the posterior ankle is dominated by the Achilles tendon, the largest and strongest tendon in the human body. Formed by the confluence of the gastrocnemius and soleus aponeuroses, the Achilles tendon inserts into the posterior calcaneal tuberosity.
Its blood supply is tenuous, particularly in the watershed area 2 to 6 centimeters proximal to its insertion. This has profound implications for surgical approaches and the risk of postoperative wound complications or tendon rupture. Deep to the Achilles tendon lies the posterior deep fascia and the posterior capsule of the ankle and subtalar joints, structures that frequently become rigidly contracted in chronic equinus deformities.
When applying circular external fixators for gradual correction, the posterior tibial neurovascular bundle (posterior tibial artery and tibial nerve) is at significant risk during distraction. The nerve is tethered at the tarsal tunnel; aggressive correction of equinovarus can induce acute tarsal tunnel syndrome. Prophylactic tarsal tunnel release is often indicated prior to initiating gradual distraction.
Step by Step Preoperative Planning
Meticulous preoperative planning is the absolute foundation of deformity correction. A complete clinical and radiographic assessment ensures that all components of a complex foot and ankle deformity are addressed.
Clinical Evaluation and Gait Analysis
The clinical evaluation must begin with an assessment of the patient's gait, noting the progression angle, heel strike, and push-off phases.
Step-by-Step Clinical Assessment:
1. Rotational Profile: Assess the thigh-foot axis to rule out proximal rotational deformities (e.g., tibial torsion) that may be compensating for or exacerbating foot pathology.
2. Hindfoot Alignment: Observe the heel from behind while the patient is standing to assess for varus or valgus.
3. Coleman Block Test: Differentiate between a flexible and rigid hindfoot varus driven by a plantarflexed first ray.
4. Silfverskiöld Test: Isolate gastrocnemius contracture from Achilles contracture.
5. Neurovascular Status: Document baseline sensation, motor function, and pulses. This is critical before initiating distraction histiogenesis.
Radiographic Assessment
Standardized, weight-bearing radiographs are non-negotiable. Non-weight-bearing films obscure the true mechanical relationships of the foot and ankle under load.
Required views include:
* Weight-bearing AP and Lateral of the foot and ankle.
* Saltzman (Hindfoot alignment) view.
* Full-length standing AP and Lateral of the bilateral lower extremities to assess Mechanical Axis Deviation (MAD), mLDFA, and MPTA.
During radiographic planning, the surgeon must map the CORA for all identified deformities. If multiple CORAs exist (e.g., a supramalleolar varus combined with a midfoot cavus), a multi-level correction strategy must be developed.
Surgical Techniques and Distraction Histiogenesis
The surgical execution of foot and ankle deformity correction relies on choosing the appropriate modality: acute correction with internal fixation versus gradual correction with external fixation.
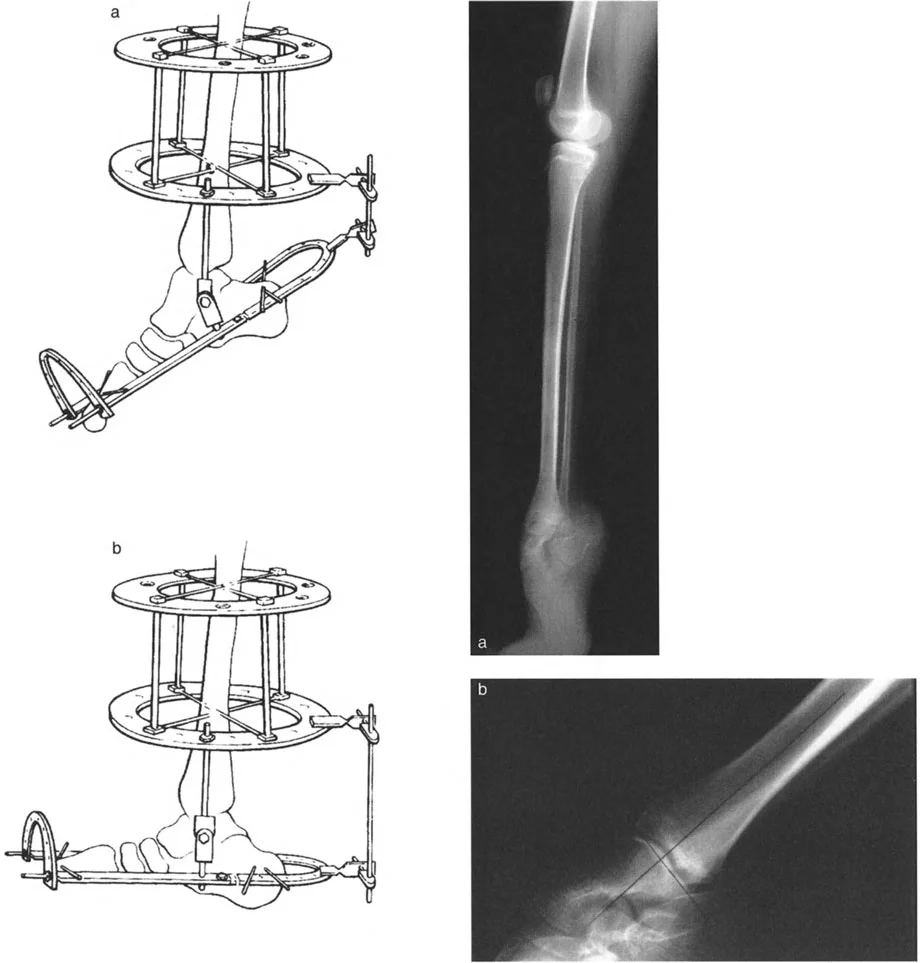
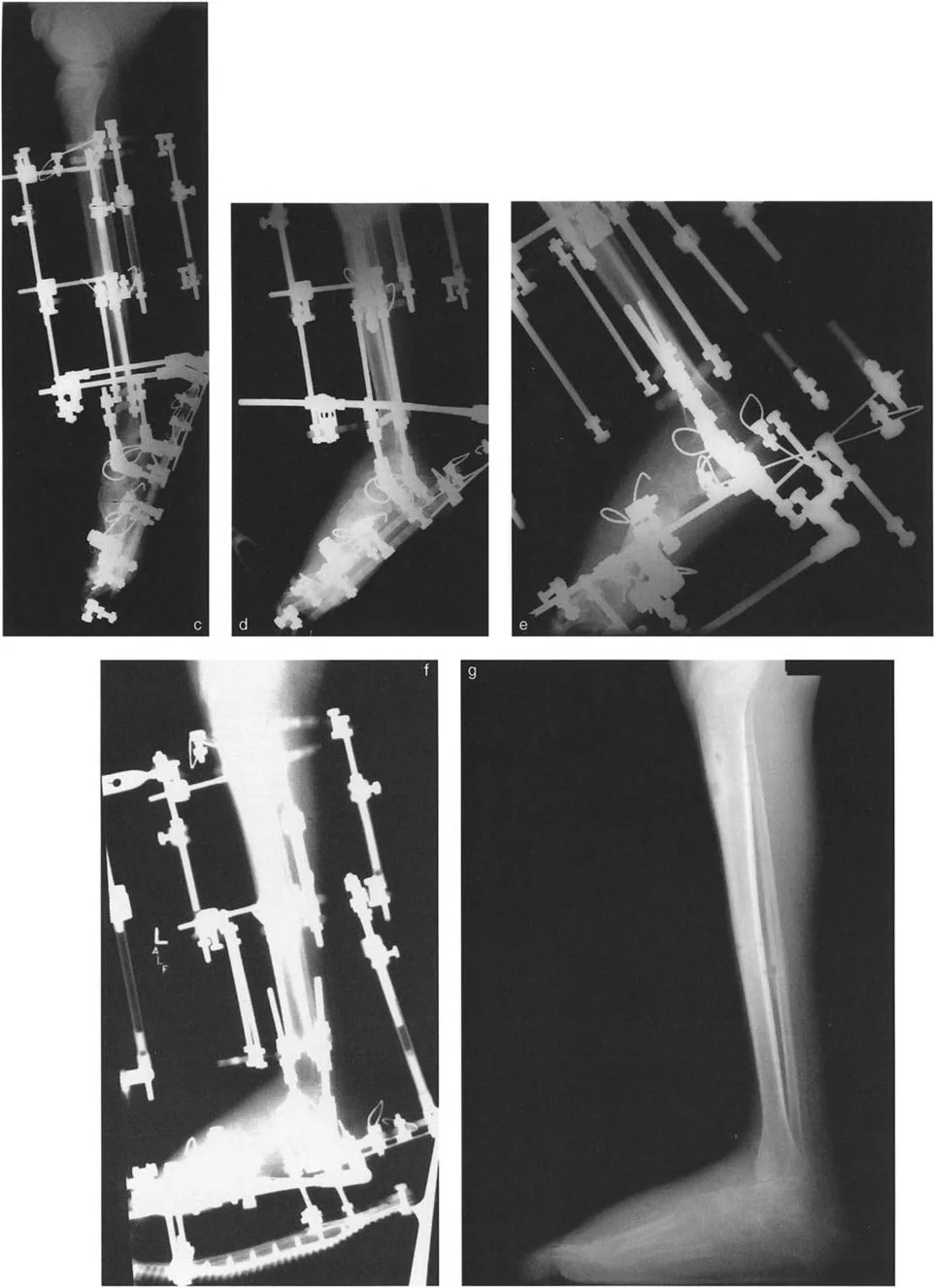
Gradual Deformity Correction with Circular External Fixation
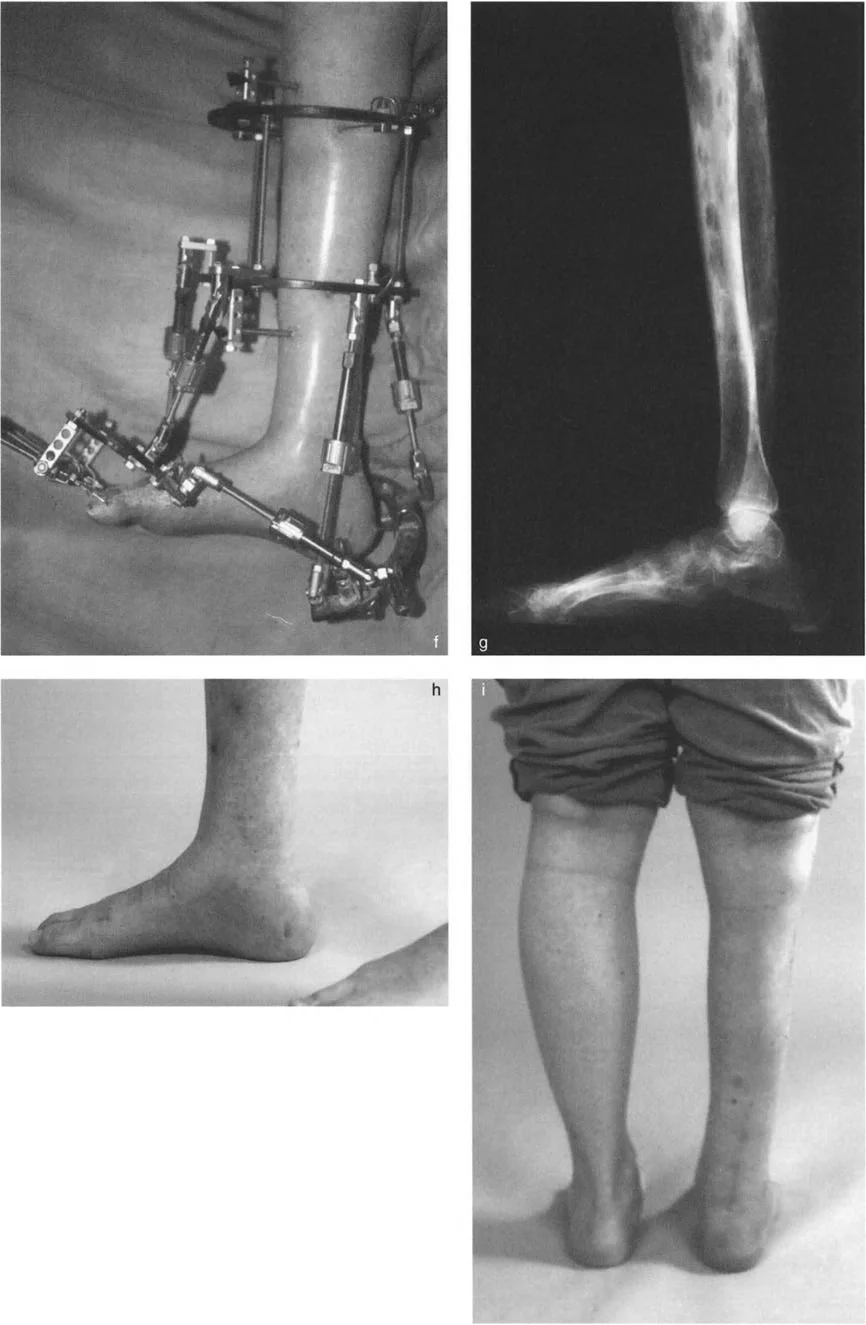
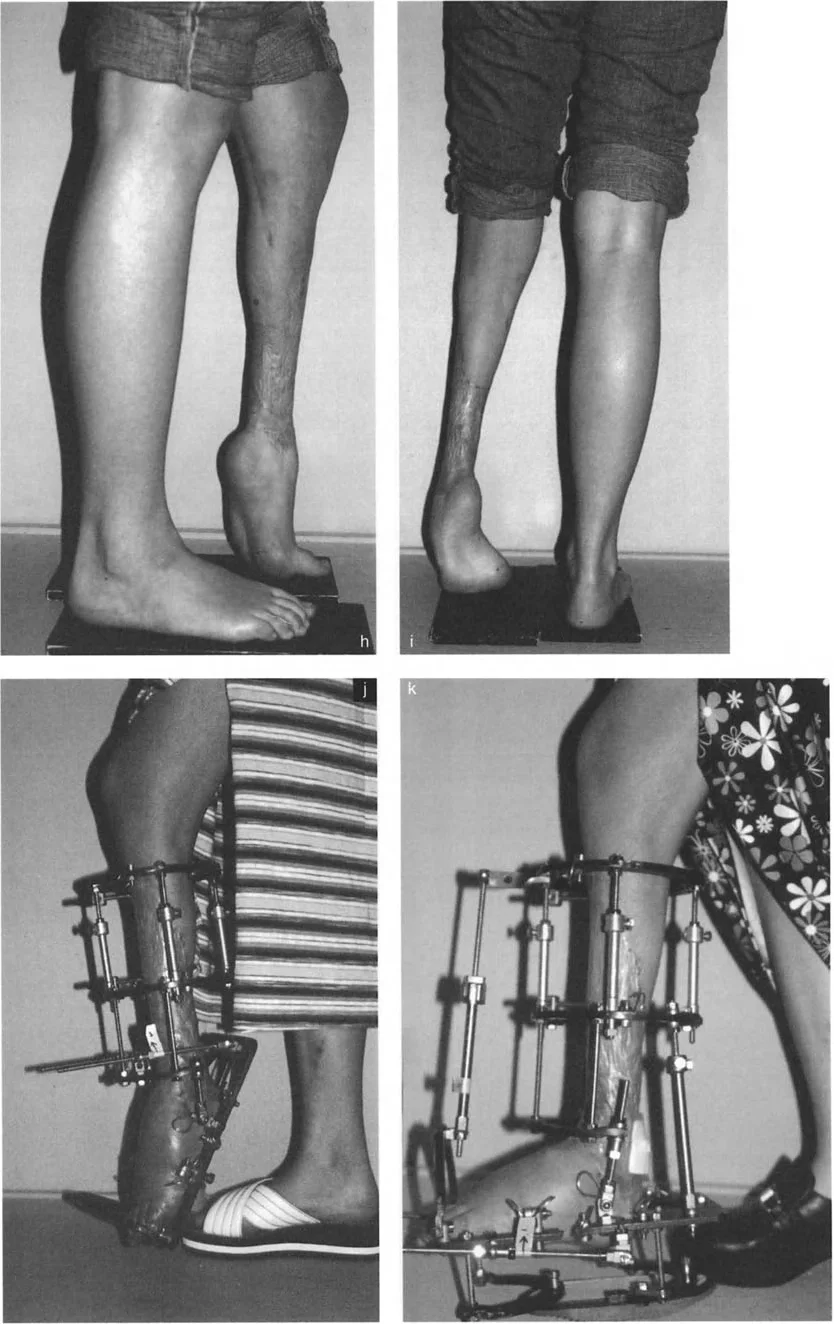
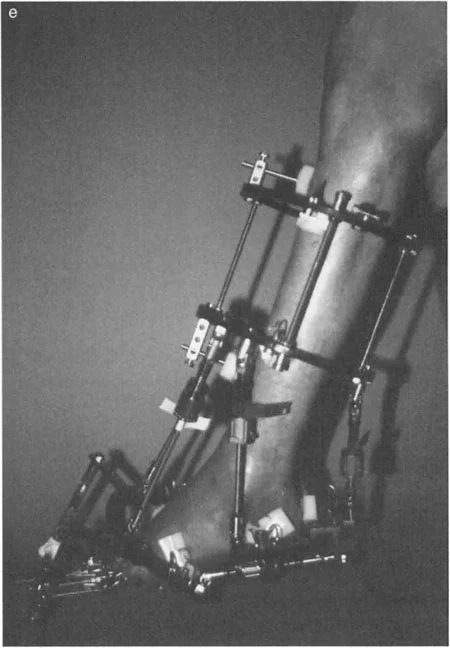
For severe, chronic, or multiplanar deformities, particularly those with compromised soft tissue envelopes or significant shortening, gradual correction using Ilizarov principles or a Taylor Spatial Frame (TSF) is the gold standard.
The application of a circular frame allows for simultaneous correction of angulation, translation, rotation, and length.
Key Frame Construction Principles:
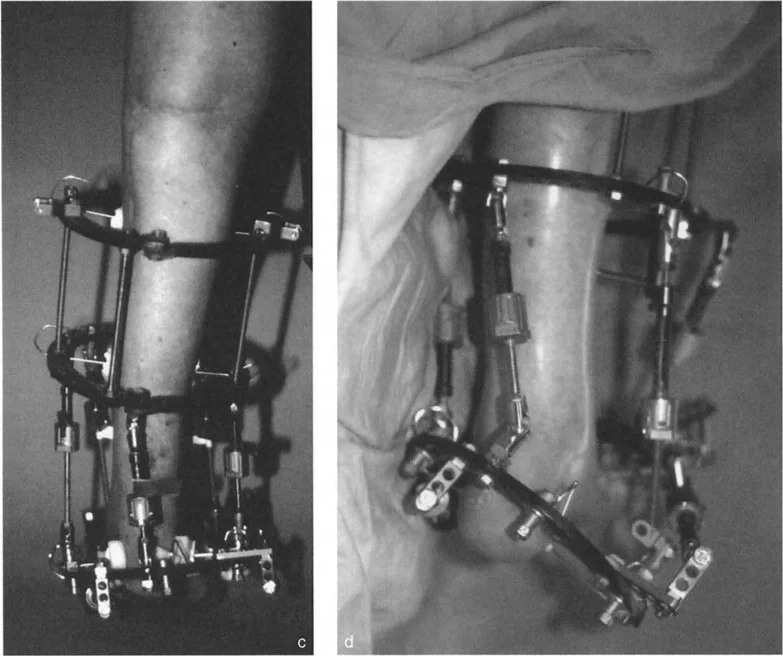
* Tibial Block: Establish a stable base in the proximal or mid-tibia using at least two rings, secured with tensioned wires and half-pins.
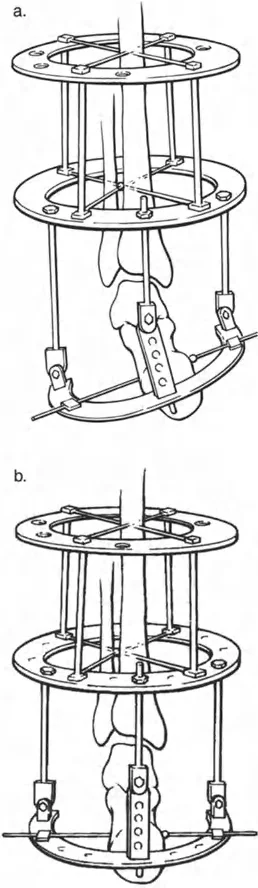
* Foot Construct: The foot is typically secured using a calcaneal half-ring (U-plate) and a forefoot half-ring. Opposing olive wires are used in the calcaneus to prevent medial or lateral translation during distraction.
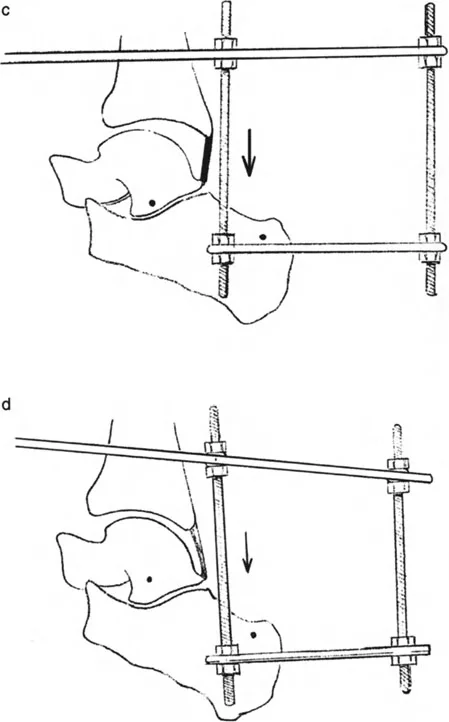
* Hinge Placement: If using traditional Ilizarov constructs, the hinges must be placed exactly on the axis of the CORA. For a true ankle equinus, the hinge is placed at the center of rotation of the talus. If using a hexapod system (TSF), the virtual hinge is programmed into the software based on precise radiographic mounting parameters.
Soft Tissue Releases versus Osseous Correction
The decision to perform soft tissue releases versus osseous osteotomies depends entirely on the location of the CORA.
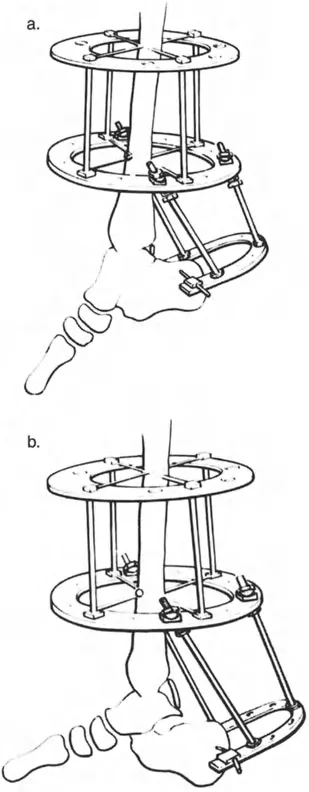
If the CORA is at the joint line (e.g., true ankle equinus), the correction requires soft tissue distraction. The frame is applied across the ankle joint, and the soft tissues are gradually stretched at a rate of 1 millimeter per day.
If the CORA is in the distal tibia (e.g., distal tibial procurvatum), a supramalleolar osteotomy is required. Performing a soft tissue release for an osseous deformity will result in joint subluxation and failure.
Surgical Pearls for Osteotomies:
* Always perform a percutaneous multiple drill-hole osteotomy (Gigli saw or osteotome) to preserve the periosteal blood supply, which is critical for distraction osteogenesis.
* If correcting a cavus deformity, a midfoot osteotomy (e.g., through the cuneiforms and cuboid) may be necessary. Ensure the osteotomy is distal to the vascular watershed of the talus.
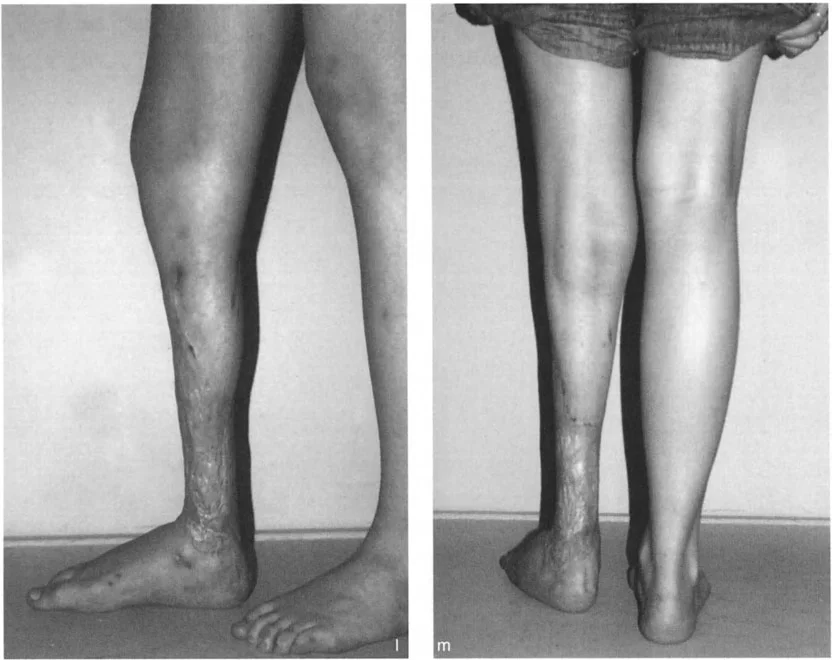
Postoperative Management and Rehabilitation
The success of deformity correction using Paley principles extends far beyond the operating room. Meticulous postoperative care is essential to prevent complications and ensure adequate bone regenerate and functional recovery.
Frame Care and Weight Bearing Protocols
Weight-bearing is highly encouraged in circular external fixation, as axial micro-motion stimulates osteogenesis in the distraction gap.
- Distraction Phase: Typically begins 7 to 10 days postoperatively (the latency period). Distraction proceeds at approximately 1 millimeter per day, divided into four 0.25 millimeter increments.
- Consolidation Phase: Once the desired correction is achieved, the frame is locked. The consolidation phase is generally twice as long as the distraction phase.
- Pin Site Care: Daily cleaning with chlorhexidine or half-strength hydrogen peroxide is required to prevent superficial pin tract infections, which are the most common complication of external fixation.
Complication Avoidance and Management
Vigilance is required to detect early signs of neurovascular compromise during the distraction phase.
- Nerve Stretch Injuries: If the patient develops burning pain, numbness, or clawing of the toes, the distraction rate must be slowed or temporarily reversed.
- Joint Subluxation: When distracting across the ankle joint or midfoot, the joints must be monitored radiographically every 2 weeks to ensure the talus is not subluxating anteriorly or posteriorly out of the mortise. Prophylactic pinning of the talonavicular or subtalar joints may be required in highly unstable feet.
- Premature Consolidation: If the distraction rate is too slow, the regenerate bone may heal prematurely, requiring a return to the operating room to re-cut the bone.
By strictly adhering to the principles of comprehensive patho-anatomical analysis, precise CORA calculation, and meticulous surgical execution, orthopedic surgeons can successfully reconstruct even the most severely deformed foot and ankle, restoring both alignment and function.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like