Mastering Distal Tibial Deformity Correction: Paley Principles & Ankle Biomechanics
Key Takeaway
Distal tibial deformities are corrected using Paley Principles, focusing on precise ankle biomechanics. Key steps involve identifying the Center of Rotation of Angulation (CORA), restoring Mechanical Axis Deviation (MAD), and understanding joint orientation angles to ensure optimal load sharing and prevent osteoarthritis.
Introduction to Distal Tibial Deformities and Paley Principles
The evaluation and management of distal tibial deformities require a profound understanding of lower extremity biomechanics, joint orientation angles, and the intricate relationship between the tibia, talus, and calcaneus. Based on the foundational principles established by Dr. Dror Paley, mastering the Center of Rotation of Angulation (CORA), the Mechanical Axis Deviation (MAD), and the compensatory mechanisms of the foot and ankle is essential for any orthopedic surgeon, resident, or fellow undertaking deformity correction.
Unlike the knee, where slight joint line convergence is tolerated, the ankle joint demands precise parallelism. A failure to recognize the spatial orientation of the ankle joint axis, the conical shape of the talus, or the cascading effects of subtalar compensation will inevitably lead to poor surgical outcomes, residual malalignment, and early-onset osteoarthritis.
This comprehensive guide deconstructs the complexities of ankle and foot considerations in distal tibial deformities, transforming fundamental concepts into a high-yield, clinically applicable masterclass for surgical planning and execution.
Core Concepts of Deformity Correction
Before addressing the specific nuances of the distal tibia, the surgeon must be fluent in the universal language of deformity correction. Dr. Paley revolutionized orthopedic surgery by introducing a systematic, reproducible geometric method for analyzing and correcting bone deformities.
Mechanical Axis Deviation and Lower Extremity Alignment
The mechanical axis of the lower extremity is a straight line drawn from the center of the femoral head to the center of the ankle joint. In a normally aligned limb, this line passes slightly medial to the center of the knee joint. Mechanical Axis Deviation (MAD) is the perpendicular distance from the center of the knee joint to this mechanical axis line.
In the presence of a distal tibial deformity, the MAD may shift medially (varus deformity) or laterally (valgus deformity). Correcting the distal tibia is not merely about making the bone look straight on a radiograph; it is about restoring the mechanical axis to a neutral position to ensure physiologic load sharing across the hip, knee, and ankle joints.

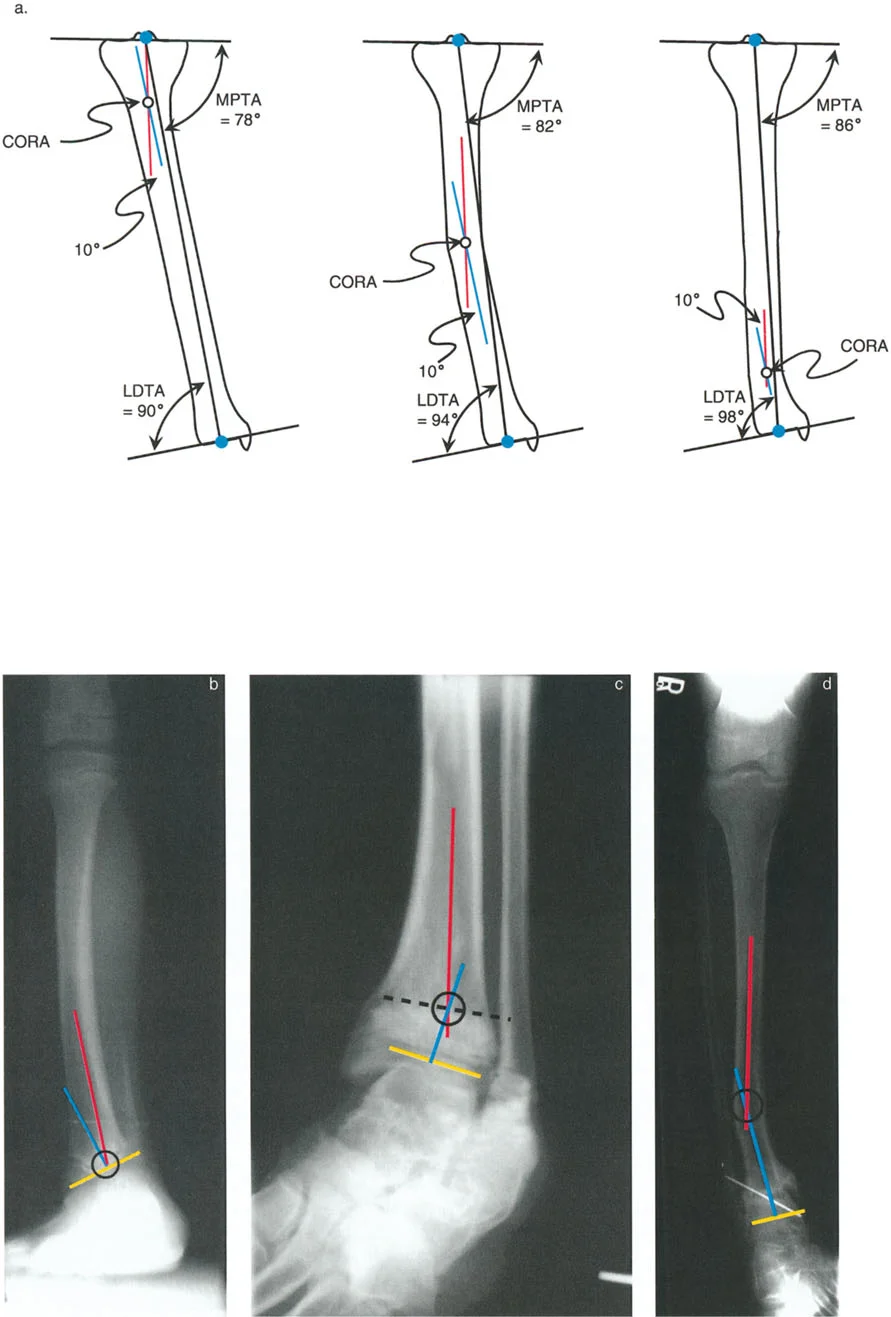
Center of Rotation of Angulation
The Center of Rotation of Angulation (CORA) is the cornerstone of Paley's principles. It represents the point of intersection between the proximal mid-diaphyseal axis and the distal mid-diaphyseal axis of a deformed bone.
Identifying the CORA is the most critical step in preoperative planning. The location of the CORA dictates where the osteotomy should ideally be performed and where the hinge of the fixation construct must be placed to achieve a perfect correction without inducing iatrogenic translation. In the distal tibia, the CORA is frequently located very close to the joint line (juxta-articular), which presents significant challenges for fixation and often necessitates applying specific osteotomy rules to perform the cut at a more proximal, biologically favorable level.

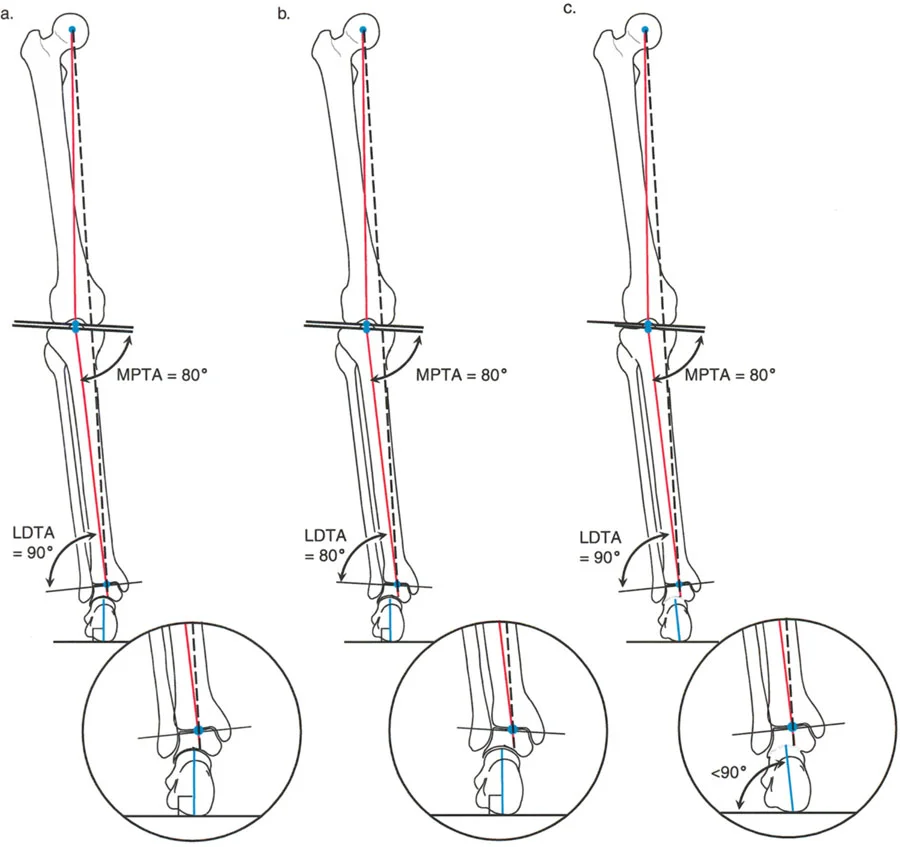
Joint Orientation Angles of the Lower Extremity
To accurately define a deformity, the surgeon relies on joint orientation angles. These are the angles formed by the intersection of the anatomic or mechanical axis of a bone with its respective joint line.
For the tibia, the critical angles include:
* MPTA (Medial Proximal Tibial Angle)
* LDTA (Lateral Distal Tibial Angle)
* ADTA (Anterior Distal Tibial Angle)
Understanding the normative values for these angles allows the surgeon to determine whether a deformity is intra-articular or extra-articular, and precisely how many degrees of correction are required in both the frontal and sagittal planes.
Normal Radiographic Anatomy of the Distal Tibia and Ankle
To correct a deformity, one must first master the parameters of normal alignment. The distal tibia and its relationship to the hindfoot present unique geometric challenges in both the frontal and sagittal planes.
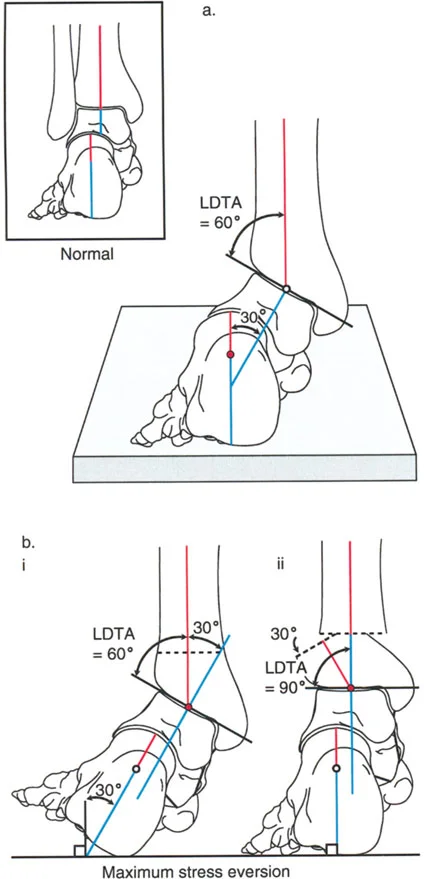
Frontal Plane Alignment and the Tibiotalar Relationship
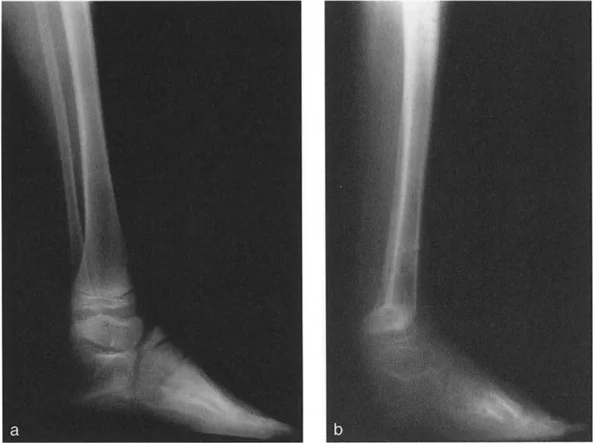
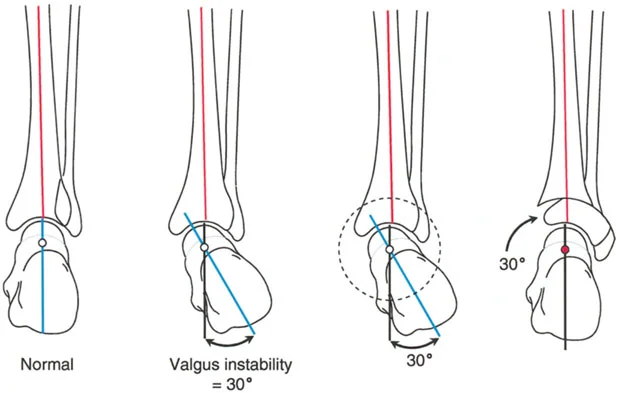
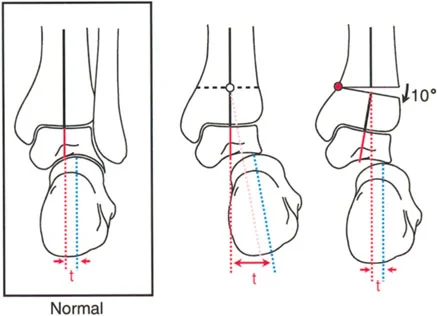
In the frontal plane, the talus presents with a distinct, squared cross-sectional appearance. The paramount rule of normal ankle alignment is that the superior dome of the talus must be strictly parallel to the tibial plafond.
Normally, there is absolutely no joint line convergence between the tibial plafond and the dome of the talus. This is a critical distinction from the knee joint, where up to a 3 degree lack of parallelism between the femoral condyle line and the tibial plateau line (Joint Line Convergence Angle, or JLCA) is considered physiologic.
When evaluating the mechanical and anatomic axes:
* The medial and lateral diaphyseal cortical lines of the tibia, when extended distally, should perfectly intersect the talus laterally and medially, respectively, aligning with the adjacent borders of the talus.
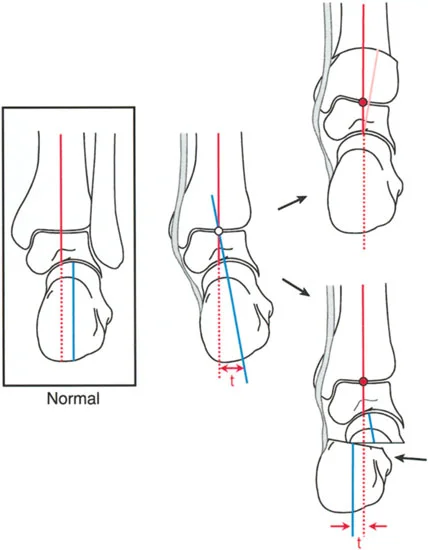
* The mid-diaphyseal line of the tibia falls slightly medial to the absolute midline of the talus.
Understanding this spatial relationship is vital when considering a fusion of the ankle following a distal tibial resection. If the medial border of the talus is made completely collinear with the medial cortex of the tibia during reconstruction, the heel will be inadvertently translated laterally, shifting the mechanical axis and creating a massive iatrogenic deformity.
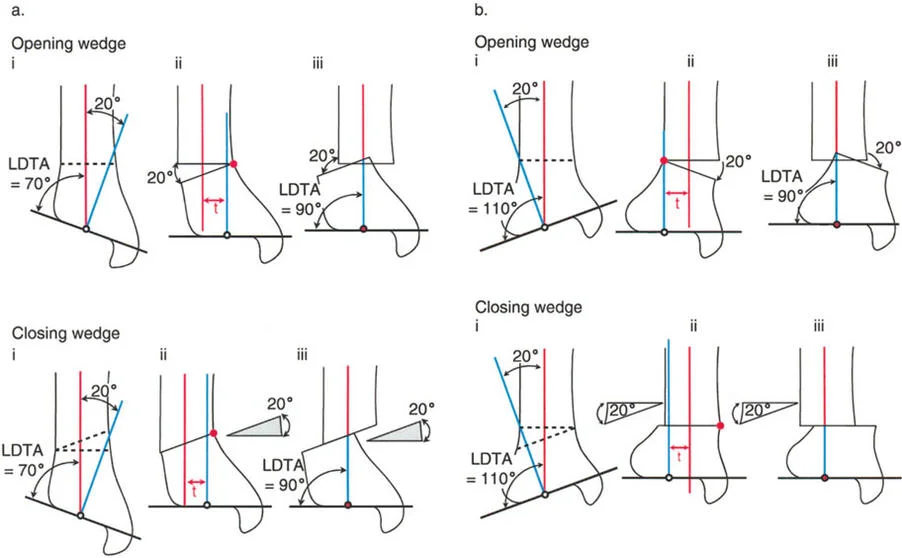
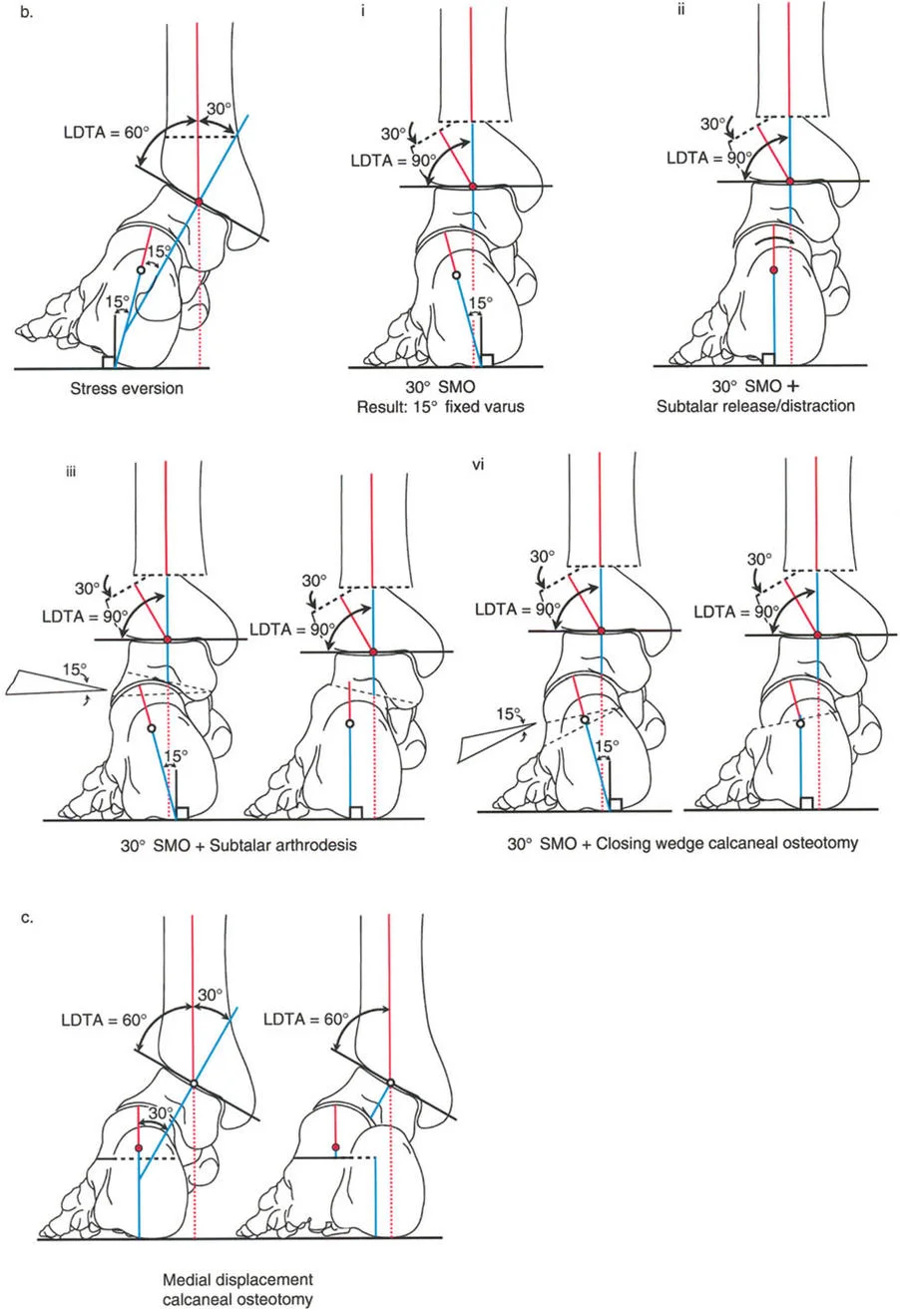
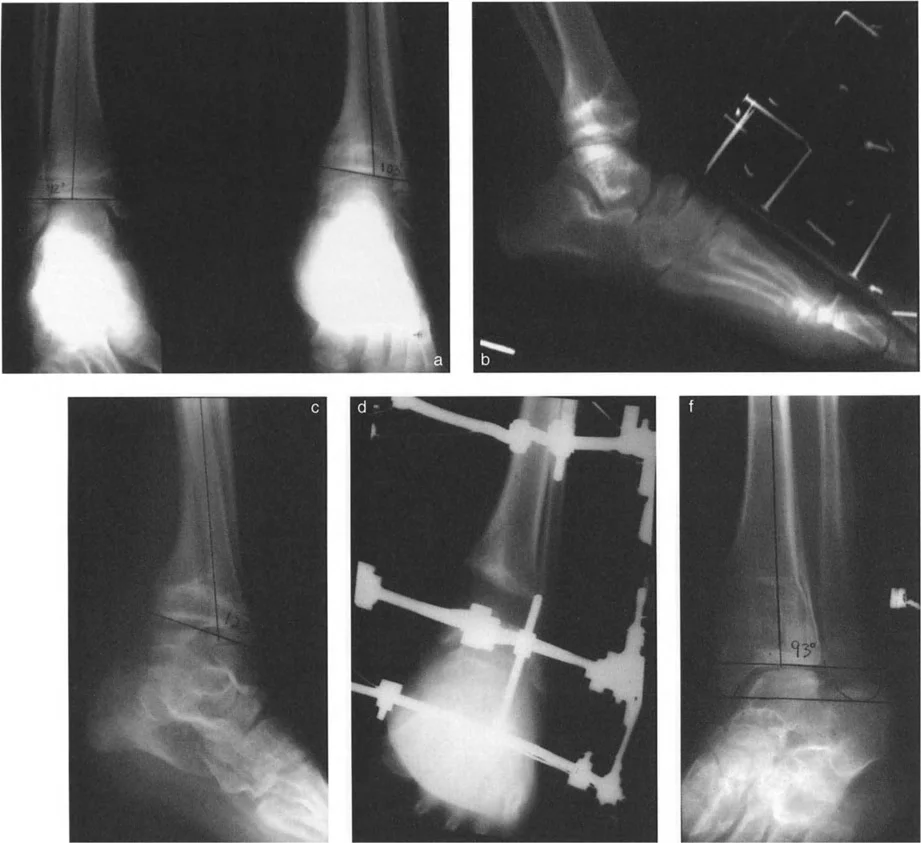
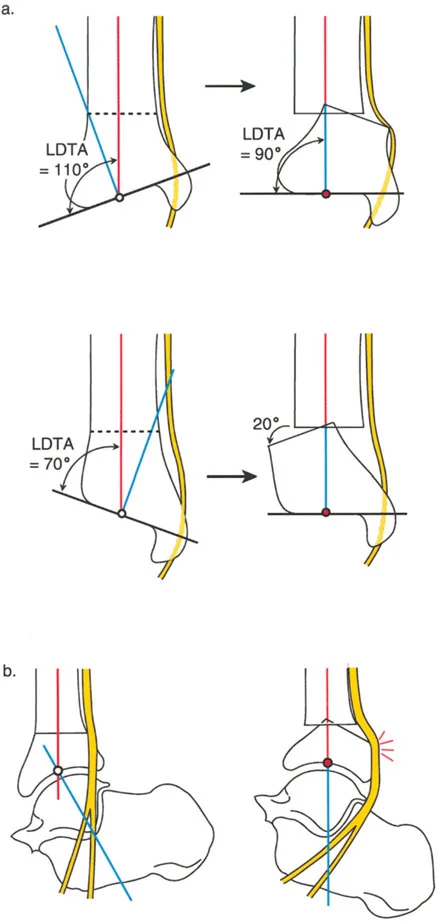
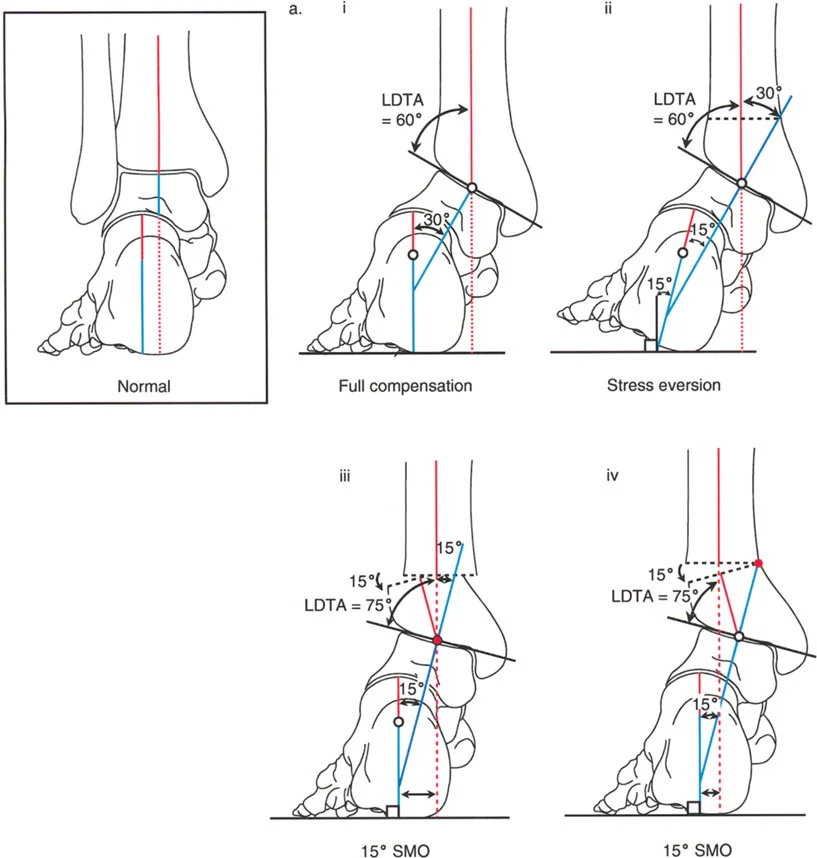
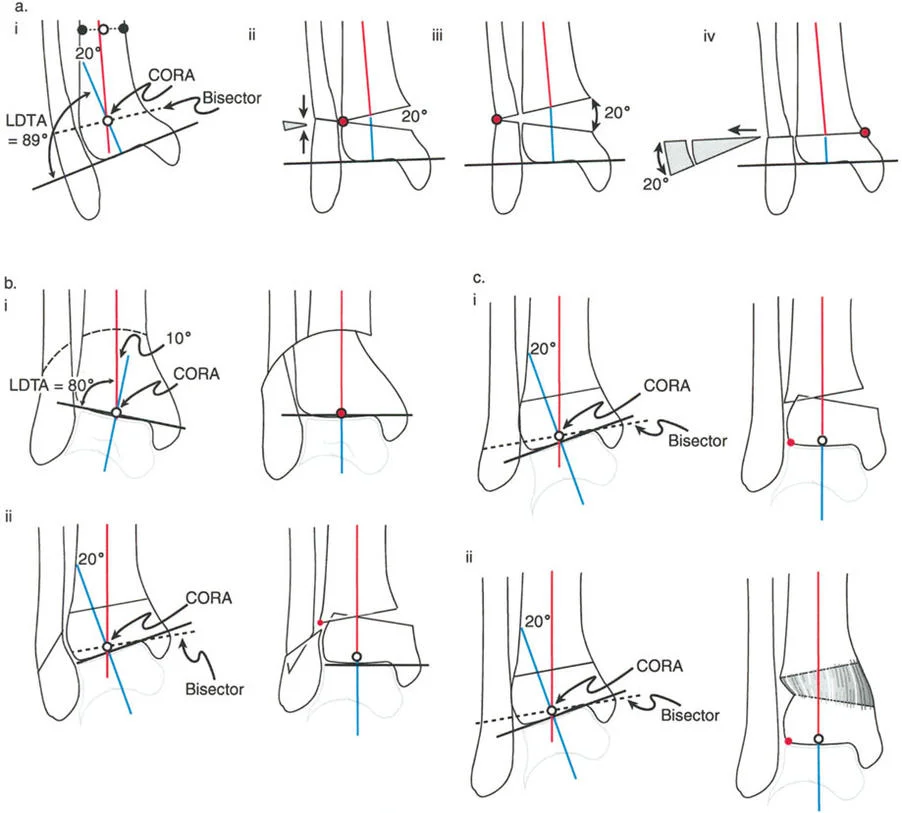
The normal Lateral Distal Tibial Angle (LDTA) is 89 degrees (range 86 to 92 degrees). Any deviation outside this narrow window indicates a frontal plane deformity (varus or valgus) that alters the load-bearing mechanics of the ankle mortise.


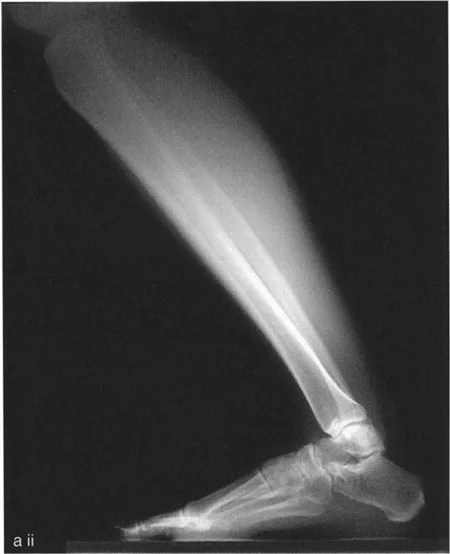
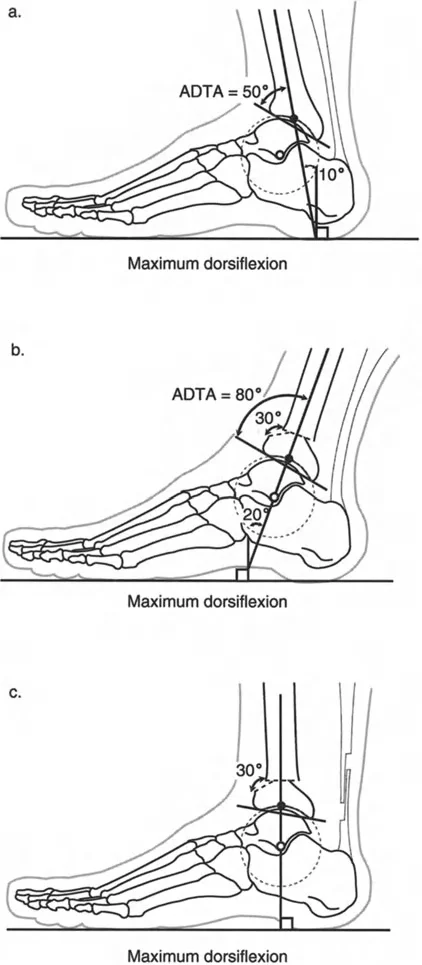
Sagittal Plane Alignment and the Talar Frustum Concept
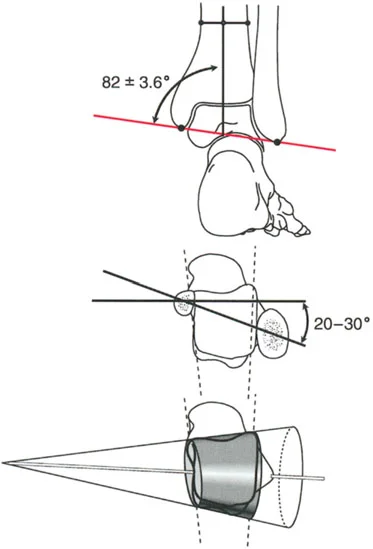
In the sagittal plane, the articular surface of the talus appears circular, but its three-dimensional anatomy is far more complex. As described by Inman and Stiehl, the three dimensional shape of the talar dome is a frustum, which is a section of a cone.
Because of this conical geometry, the axis of ankle rotation is not a simple hinge parallel to the joint line. Instead, the true axis of rotation:
* Runs obliquely from the tip of the medial malleolus (anterosuperior) to the tip of the lateral malleolus (posteroinferior).
* Passes directly through the lateral process of the talus.
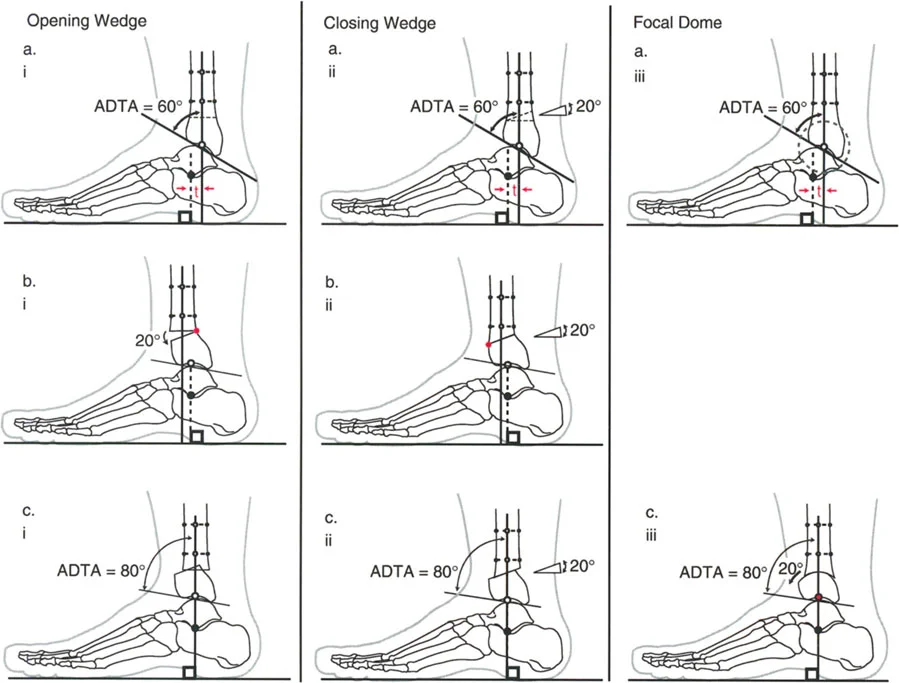
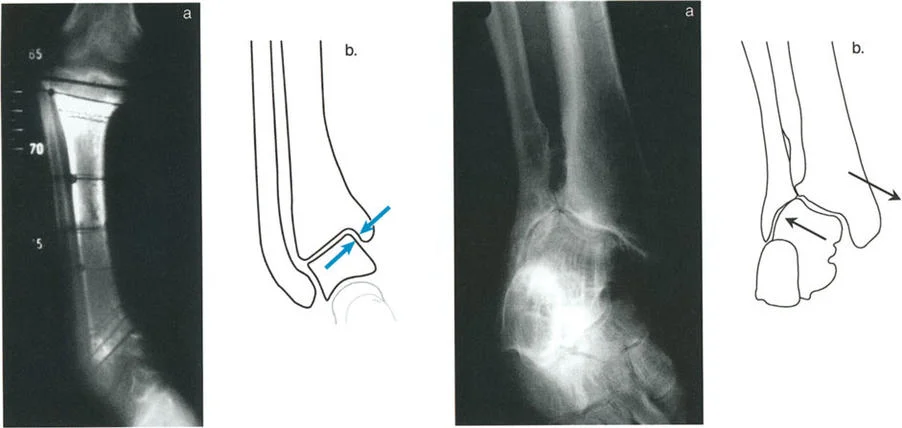
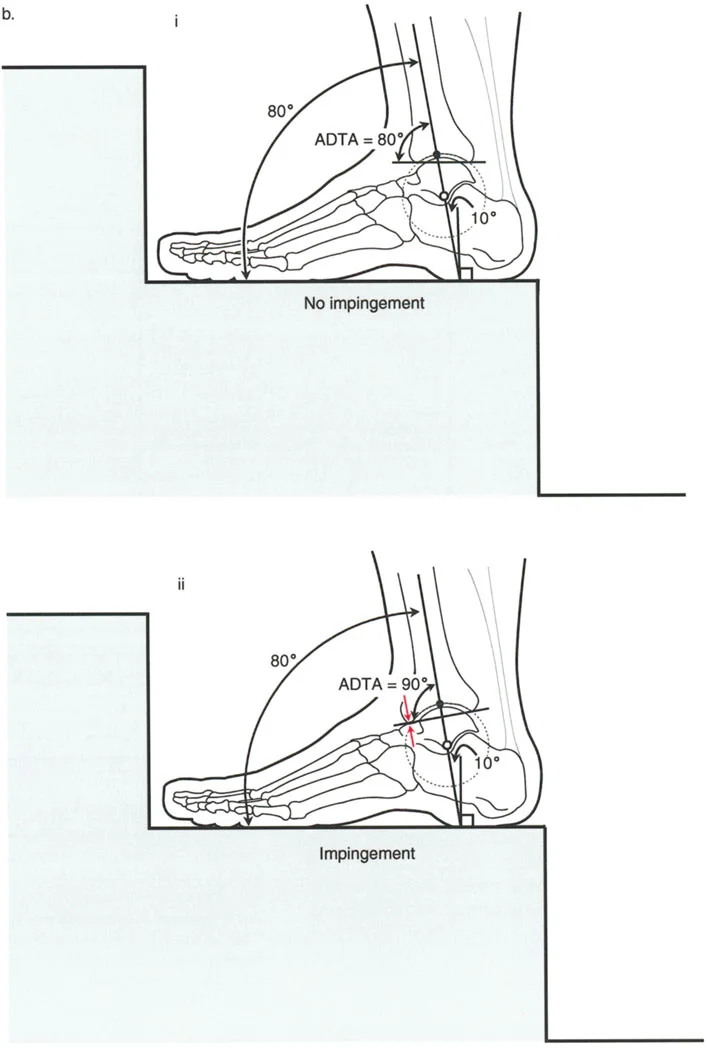
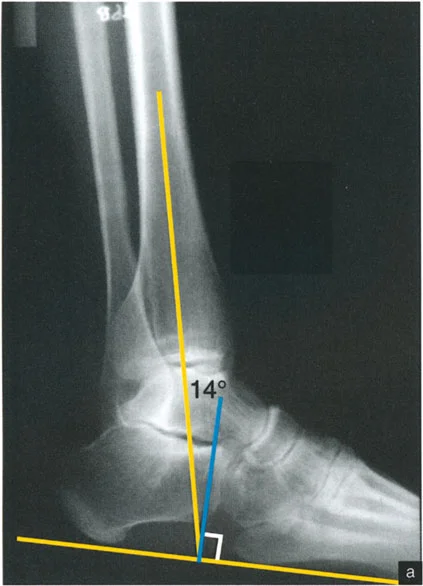
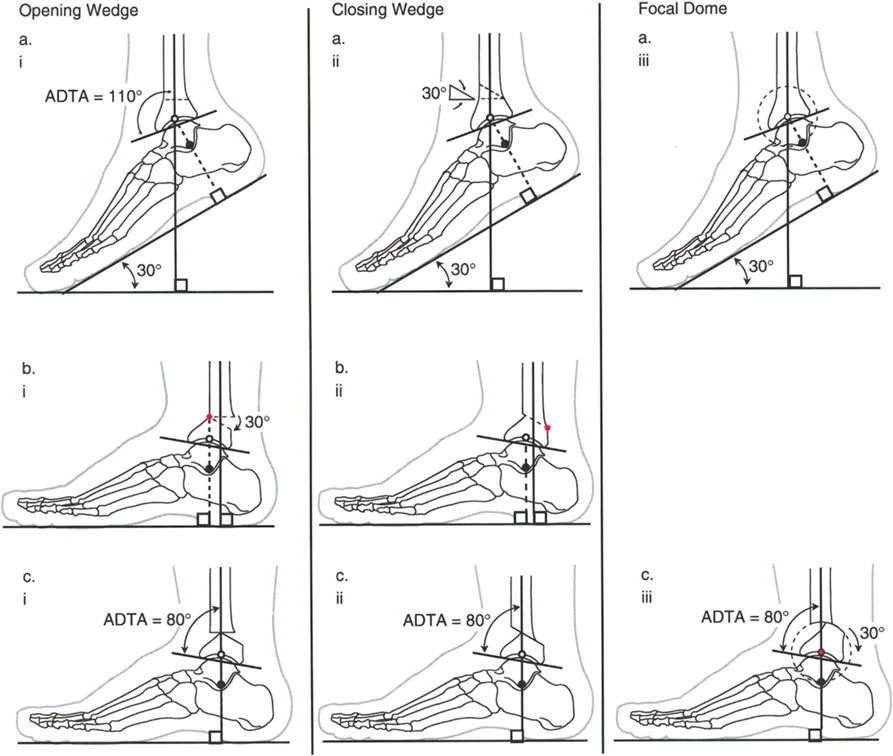
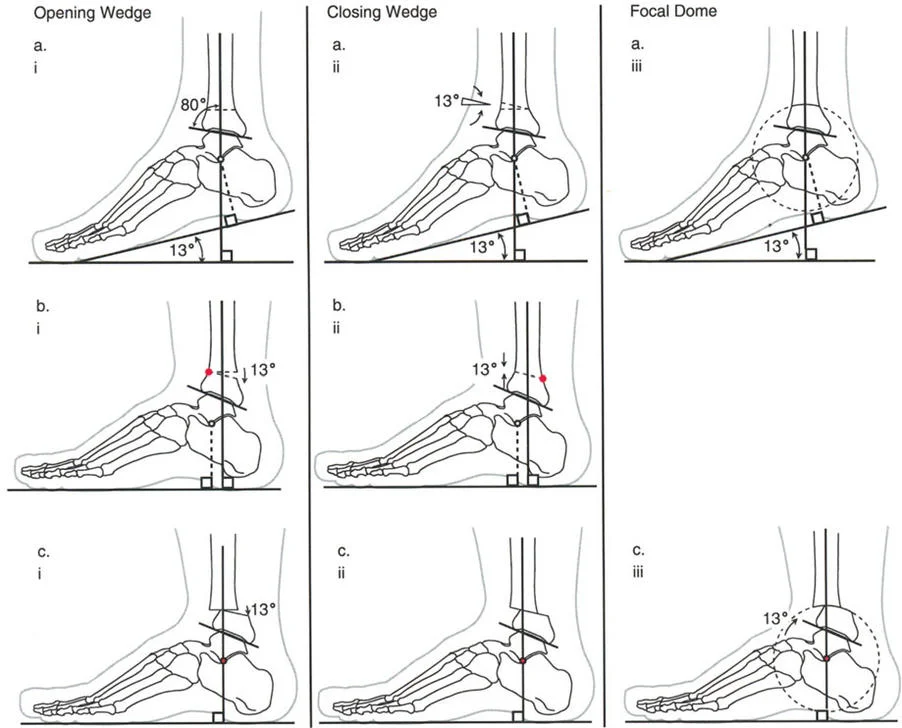
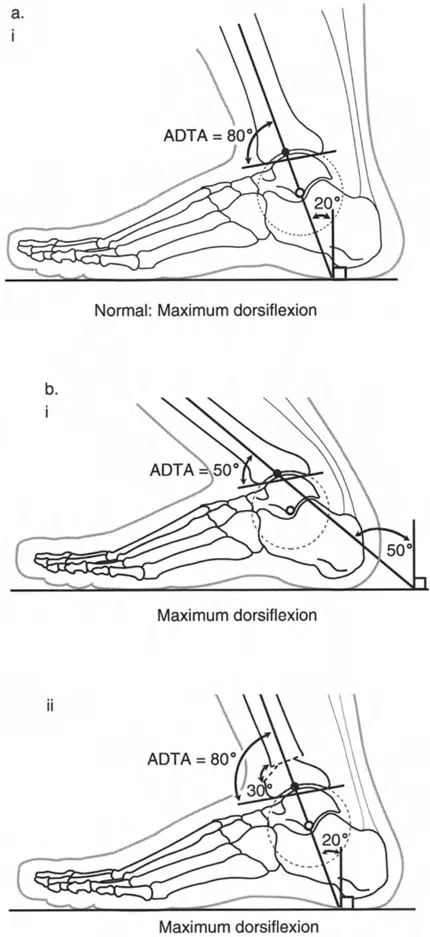
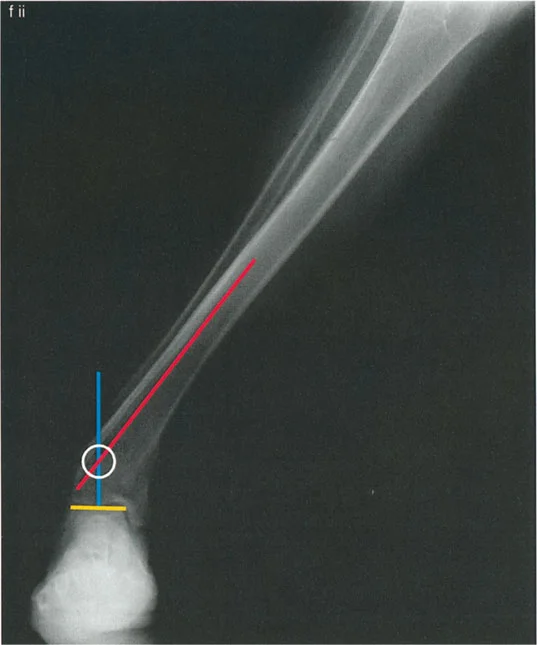
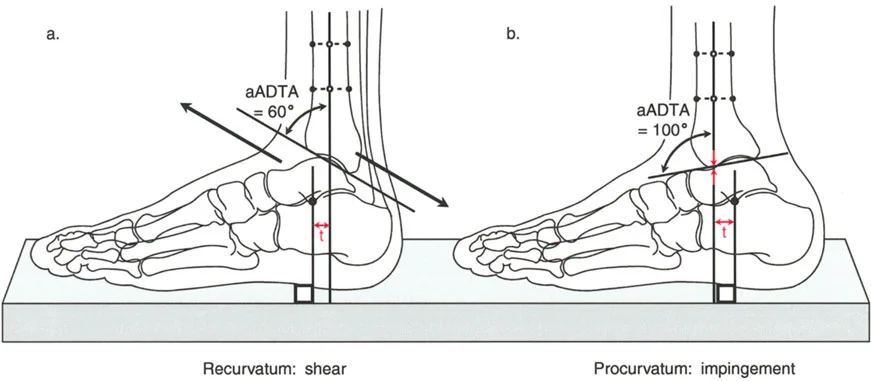
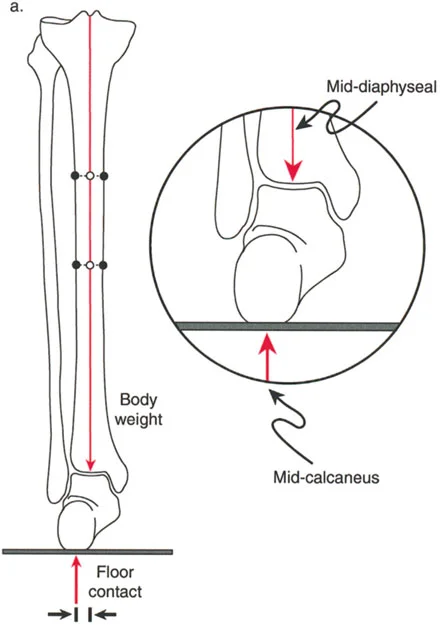
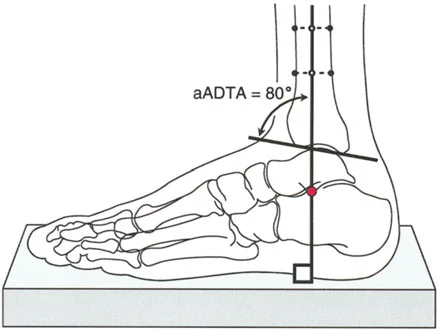
On a lateral radiograph, when the plantar aspect of the foot is at exactly 90 degrees to the tibia, the mid-diaphyseal line of the tibia should pass precisely through the lateral process of the talus, which approximates the center of rotation of the ankle joint. Furthermore, the normal tibial plafond is tilted anteriorly, yielding an Anterior Distal Tibial Angle (ADTA) of exactly 80 degrees (range 78 to 82 degrees).

Ankle Biomechanics and the Ground Reaction Force Vector
The orientation of the calcaneus relative to the talus and tibia dictates how forces are transmitted from the ground through the lower extremity. Deformity correction must account for these dynamic forces to ensure longevity of the adjacent joints.
Calcaneal Alignment and the Saltzman View
In the sagittal plane, the long axis of the calcaneal body is inclined, creating the calcaneal pitch. In the frontal plane, however, the calcaneus is notoriously difficult to visualize on standard radiographs. Clinically, hindfoot alignment is best evaluated from behind the standing patient.
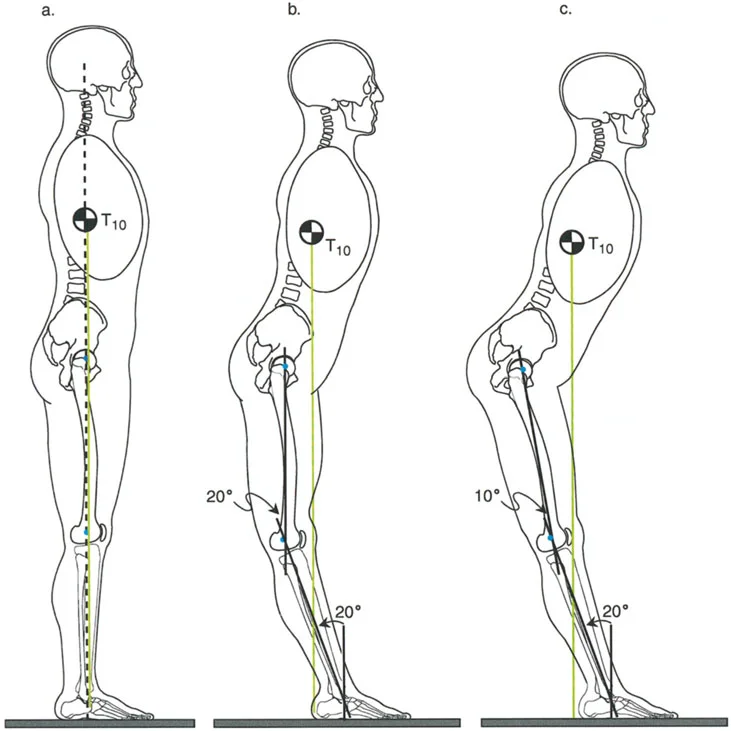
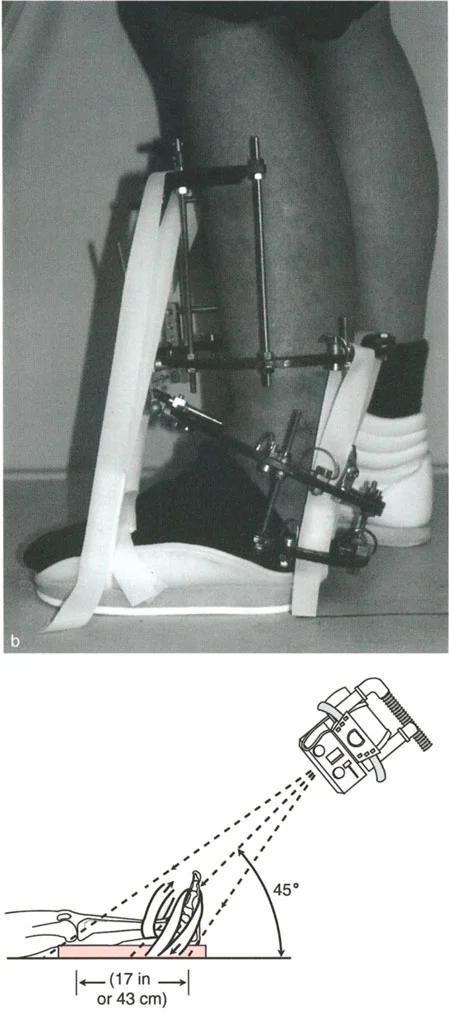
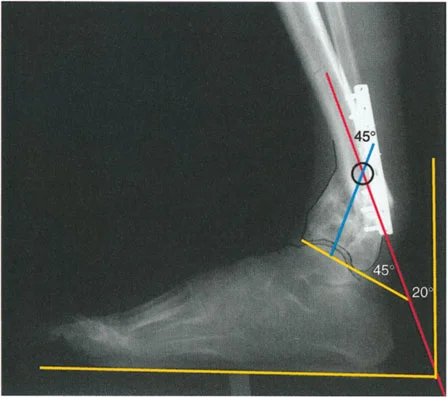
Radiographically, the axis of the body of the calcaneus is parallel to the anatomic axis of the tibia, but it is laterally displaced. This lateral displacement is due to the stepped articulation of the subtalar joint via the sustentaculum tali. To accurately measure this, a long axial view radiograph (Saltzman view) is obtained at a 20 degree inclination to the horizontal. This view allows the surgeon to measure the alignment of the calcaneus relative to the mid-diaphyseal line of the tibia and compare it to the contralateral normal side.
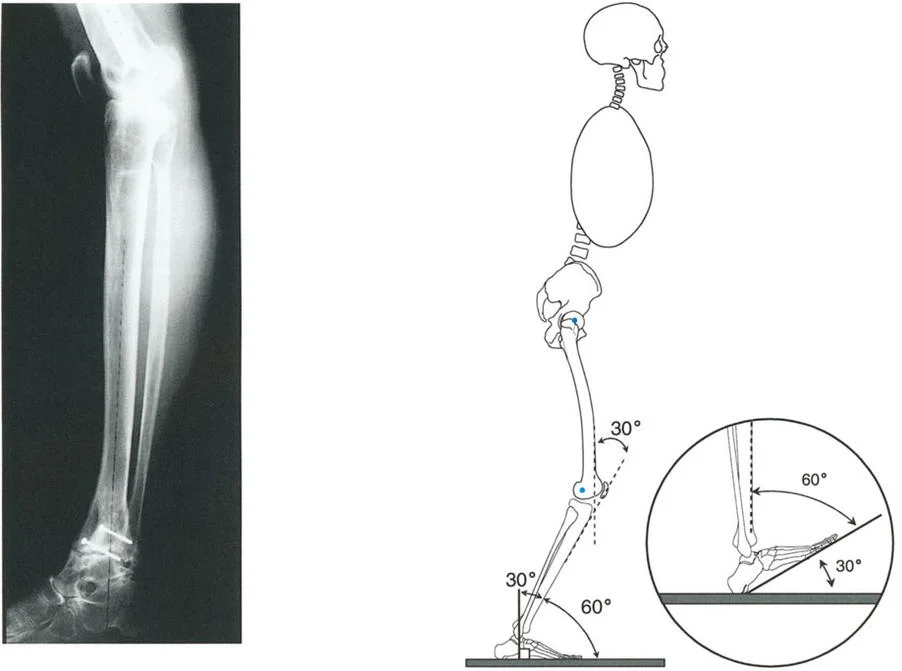
Valgus Moment and Dorsiflexion Moment Dynamics
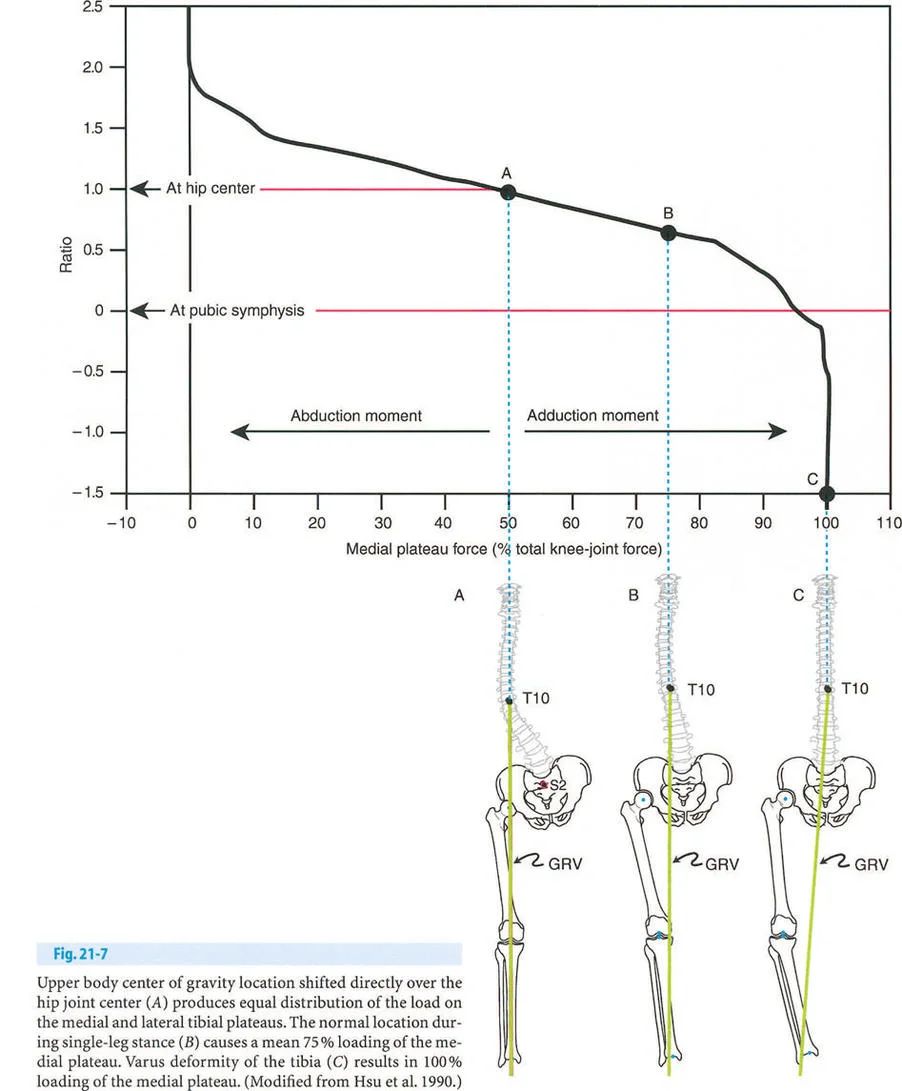
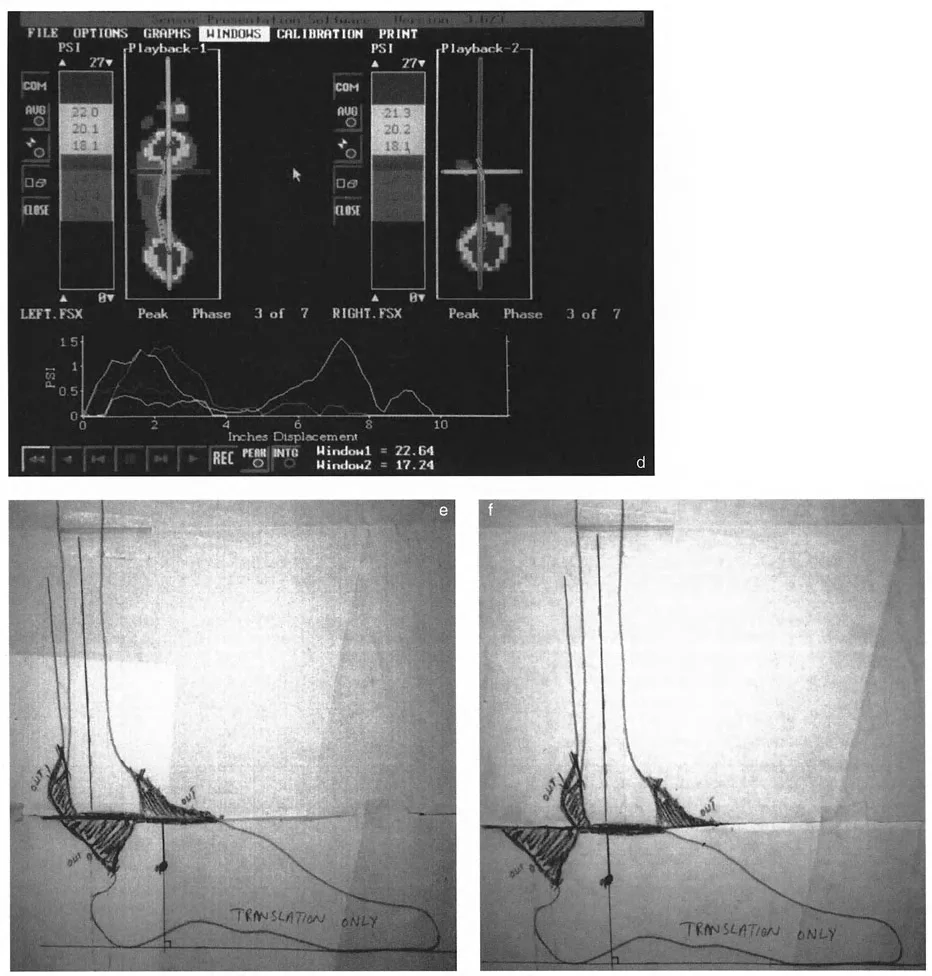
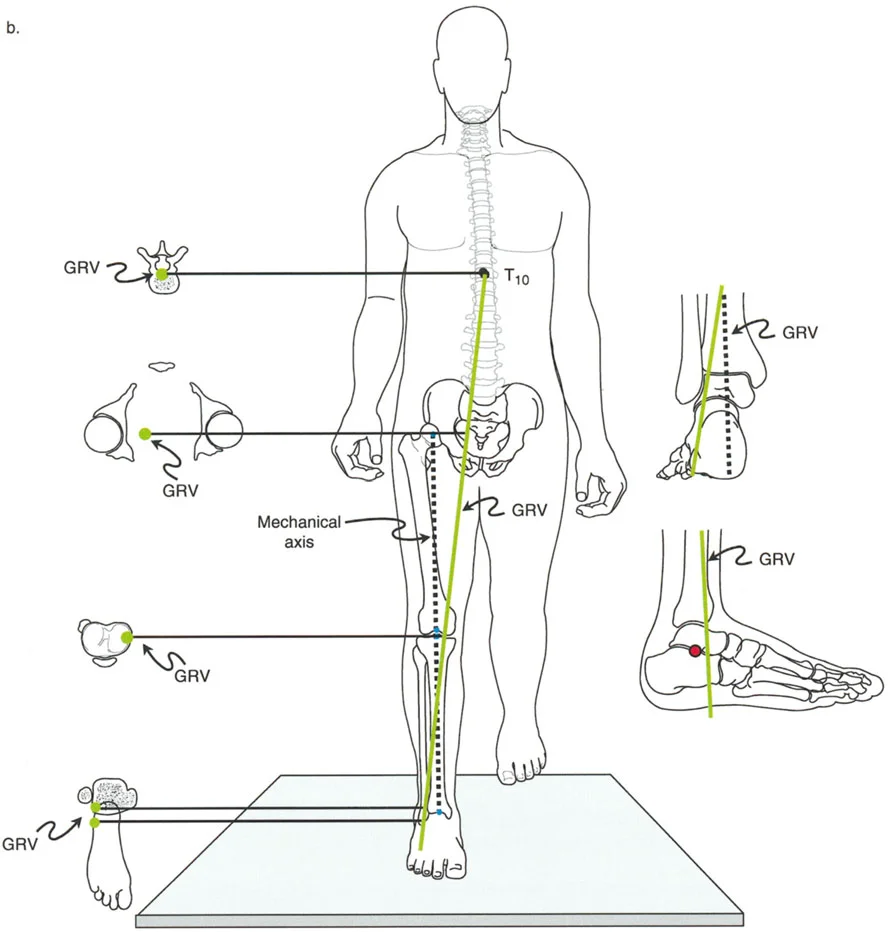
During normal single-leg stance, the Ground Reaction Force Vector (GRV) originates from the lateral border of the foot.
- Frontal Plane: The GRV passes lateral to the center of the subtalar and ankle joints. This imparts a continuous valgus moment on the hindfoot.
- Sagittal Plane: The GRV passes anterior to the center of rotation of the ankle joint, corresponding to the calcaneocuboid joint at the sole of the foot. This imparts a continuous dorsiflexion moment.
Because the GRV is located anterior and lateral to the ankle joint, the anterolateral aspect of the tibiotalar joint is subjected to the greatest moment arm of stress.
Muscular Compensation Mechanisms
This biomechanical reality explains two critical clinical phenomena regarding muscle activation. The tibialis posterior (inverter) and the gastro-soleus complex (plantar flexors) must remain highly active during the majority of the single-leg stance phase to dynamically counter the passive valgus and dorsiflexion moments.
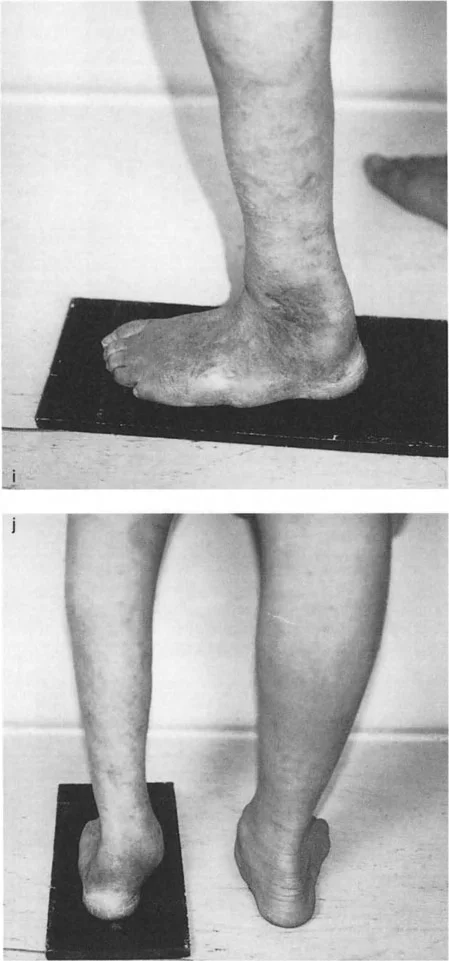
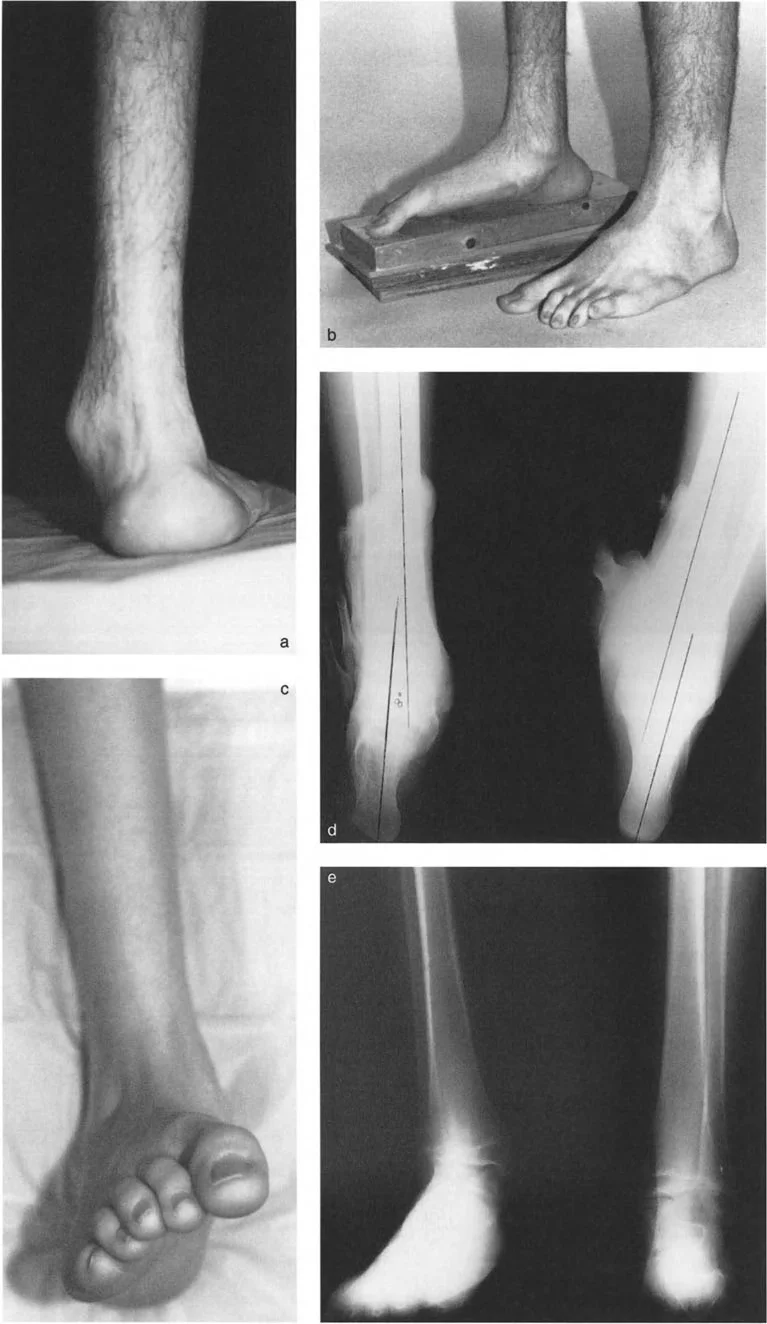
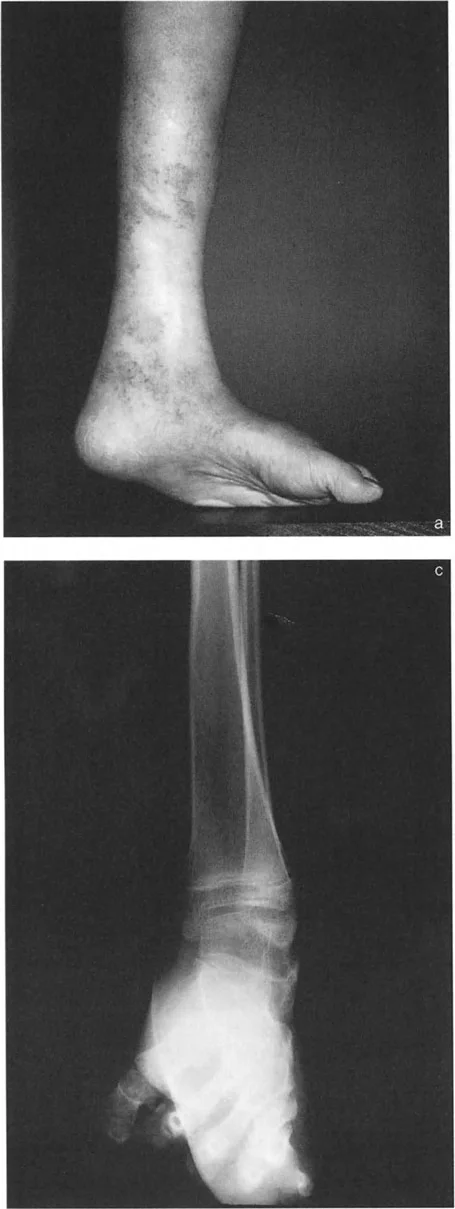
When a distal tibial deformity alters the GRV, these muscle groups are forced into overdrive, leading to tendinopathy, fatigue, and eventual failure. For example, a severe valgus deformity of the distal tibia shifts the GRV even further laterally, exponentially increasing the valgus moment and rapidly exhausting the tibialis posterior tendon, often resulting in acquired flatfoot deformity secondary to the tibial malalignment.
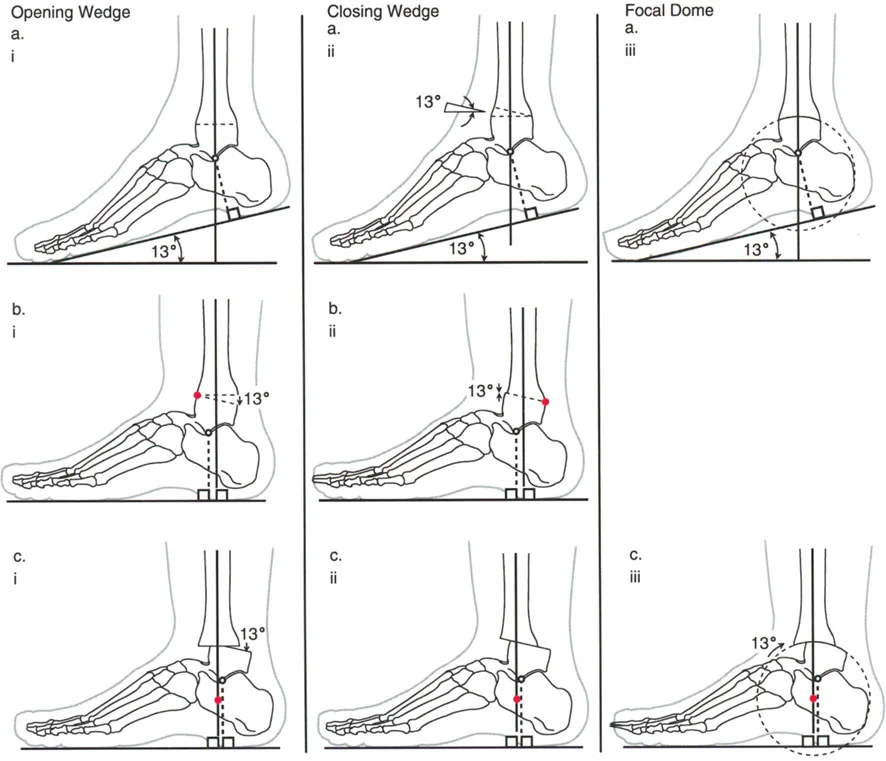
Paley Osteotomy Rules for Distal Tibial Deformities
Translating the geometric analysis into surgical execution relies on the three Paley Osteotomy Rules. Understanding these rules is non-negotiable for preventing iatrogenic translation (the "Z-deformity") during correction.
Osteotomy Rule One
When the osteotomy and the axis of correction (the hinge) are both located at the CORA, pure angulation occurs, and the mechanical axis is perfectly realigned without any translation.
In the distal tibia, Rule One is often difficult to execute because the CORA frequently lies within the metaphyseal flare or directly on the joint line. Performing an osteotomy too close to the joint capsule compromises fixation and healing.

Osteotomy Rule Two
When the osteotomy is performed at a level different from the CORA (usually more proximal in the tibial diaphysis for better bone stock and soft tissue coverage), but the axis of correction (hinge) remains at the CORA, the bone ends will angulate and translate relative to each other.
This translation is not a complication; it is a mathematical necessity to restore the collinearity of the proximal and distal axes. This is the most frequently utilized rule in distal tibial deformity correction. The surgeon intentionally creates translation at the osteotomy site to ensure the mechanical axis of the entire leg is restored.
Osteotomy Rule Three
When the osteotomy and the axis of correction are both located outside the CORA, a new deformity (iatrogenic translation) is created. The mechanical axis will remain deviated. Rule Three is generally considered a surgical error in primary deformity correction, though it is sometimes used intentionally in complex, multi-apical deformities or bone transport scenarios.

Step by Step Preoperative Planning for Distal Tibial Correction
Meticulous preoperative planning is the difference between an excellent outcome and a catastrophic failure. The process must be standardized and rigorous.
Clinical and Radiographic Evaluation
- Obtain Quality Imaging: Procure full-length, weight-bearing standing radiographs of both lower extremities. Include dedicated AP, Lateral, and Mortise views of the ankle, as well as a Saltzman view for hindfoot alignment.
- Assess Soft Tissues: Evaluate the skin envelope. The anteromedial face of the distal tibia has minimal soft tissue coverage. Previous scars, skin grafts, or compromised vascularity will dictate the surgical approach and fixation method.
- Evaluate Joint Range of Motion: Document ankle and subtalar motion. A rigid subtalar joint will not compensate for a corrected tibia, potentially leaving the foot unplantable.
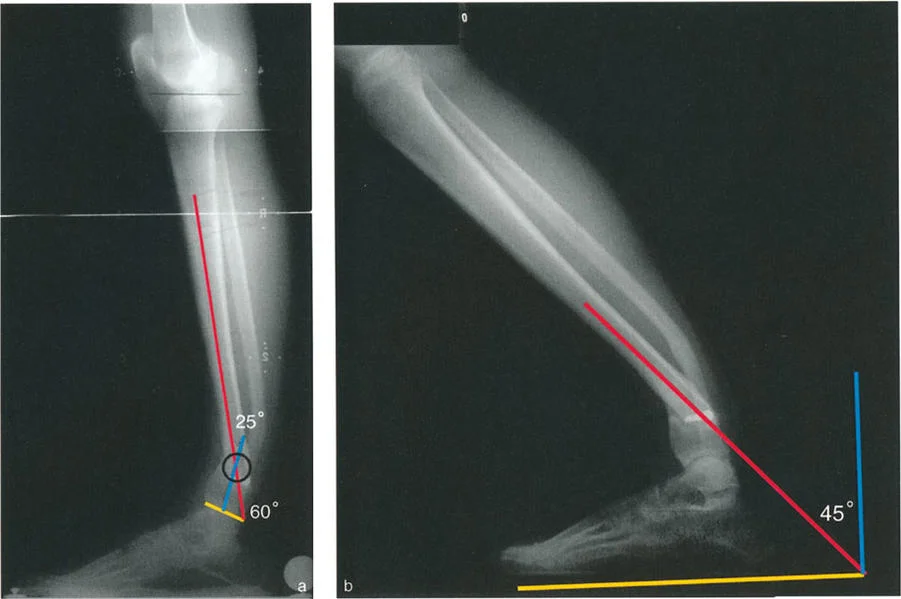
Determining the Deformity Apex
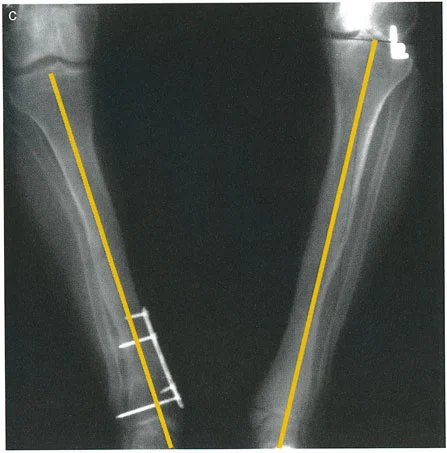
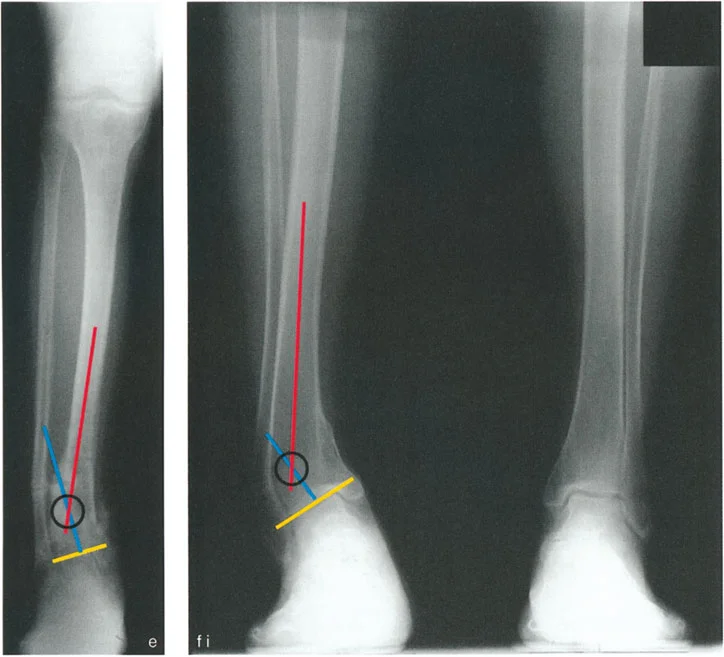
- Draw the Proximal Axis: Draw the mid-diaphyseal line of the proximal tibia.
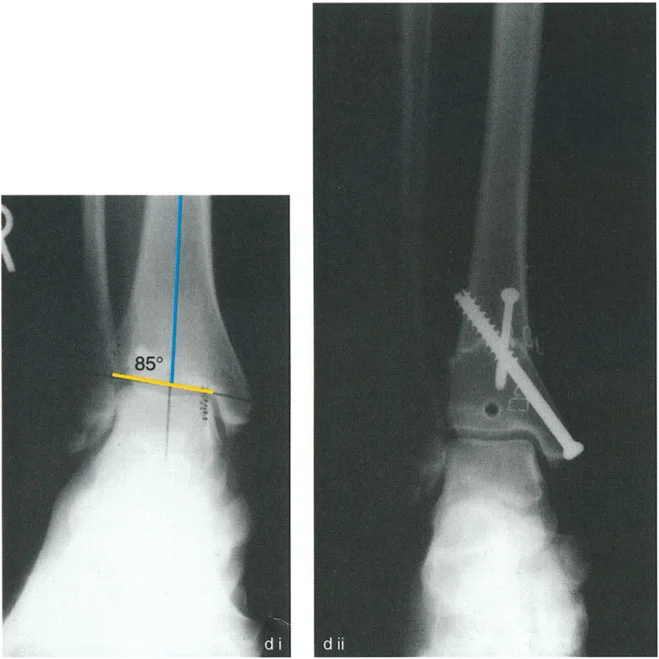
- Draw the Distal Axis: Draw the joint orientation line of the tibial plafond. Drop a line at 89 degrees (the normal LDTA) to this joint line. This represents the normal distal anatomic axis.
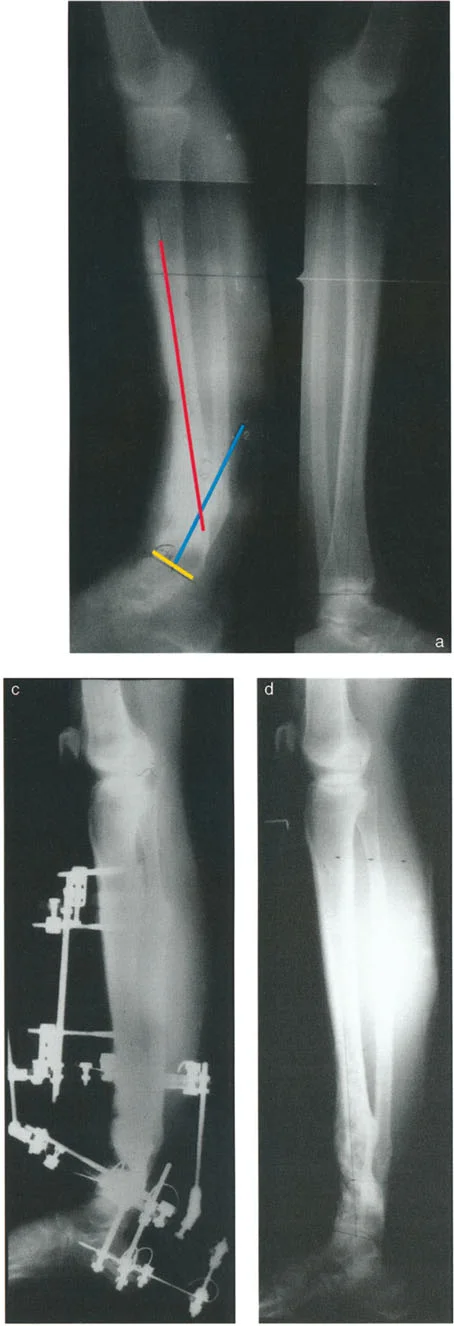
- Locate the CORA: The intersection of the proximal diaphyseal line and the distal anatomic line is the CORA.
- Measure the Magnitude: The angle formed at the CORA is the true magnitude of the deformity in that plane. Repeat this process on the lateral radiograph using the ADTA (80 degrees) to find the sagittal plane CORA.

Selecting the Fixation Method
The choice of fixation depends on the magnitude of the deformity, the presence of poor soft tissues, limb length discrepancy, and patient compliance.
| Fixation Type | Primary Indications | Advantages | Disadvantages |
|---|---|---|---|
| Circular External Fixation (Hexapod) | Multiplanar deformities, poor soft tissue, LLD, active infection | Allows postoperative adjustment, minimally invasive, perfect Rule 2 execution | Pin tract infections, bulky, requires high patient compliance |
| Intramedullary Nailing | Diaphyseal to metaphyseal deformities, good soft tissue | Load sharing, highly stable, no pin care | Requires Poller screws for distal control, technically demanding to prevent wedge effect |
| Plating (MIPO) | Simple uniplanar deformities, juxta-articular CORA | Rigid internal fixation, familiar technique | Extensive soft tissue stripping if not done percutaneously, fixed angle cannot be adjusted post-op |
Surgical Execution and Advanced Fixation Strategies
Once the plan is solidified, execution requires precision. The distal tibia is unforgiving due to its watershed blood supply and proximity to the ankle joint.
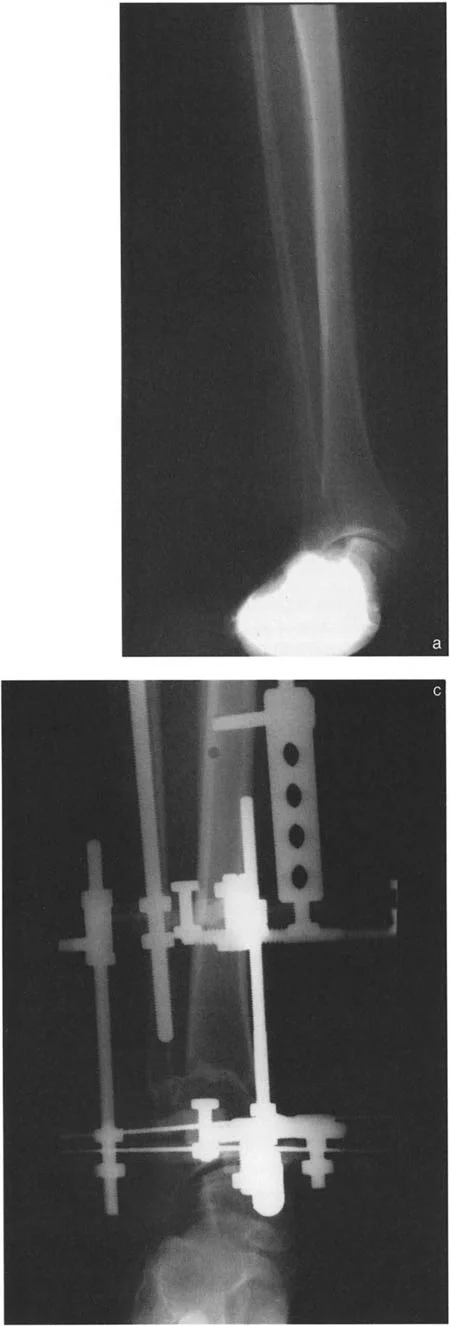
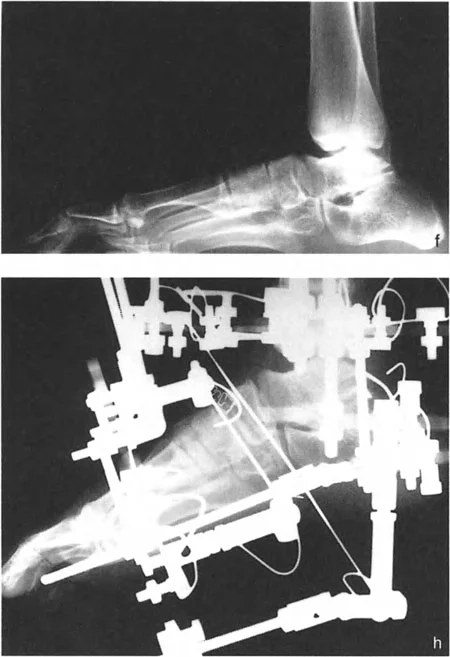
External Fixation and Hexapod Systems
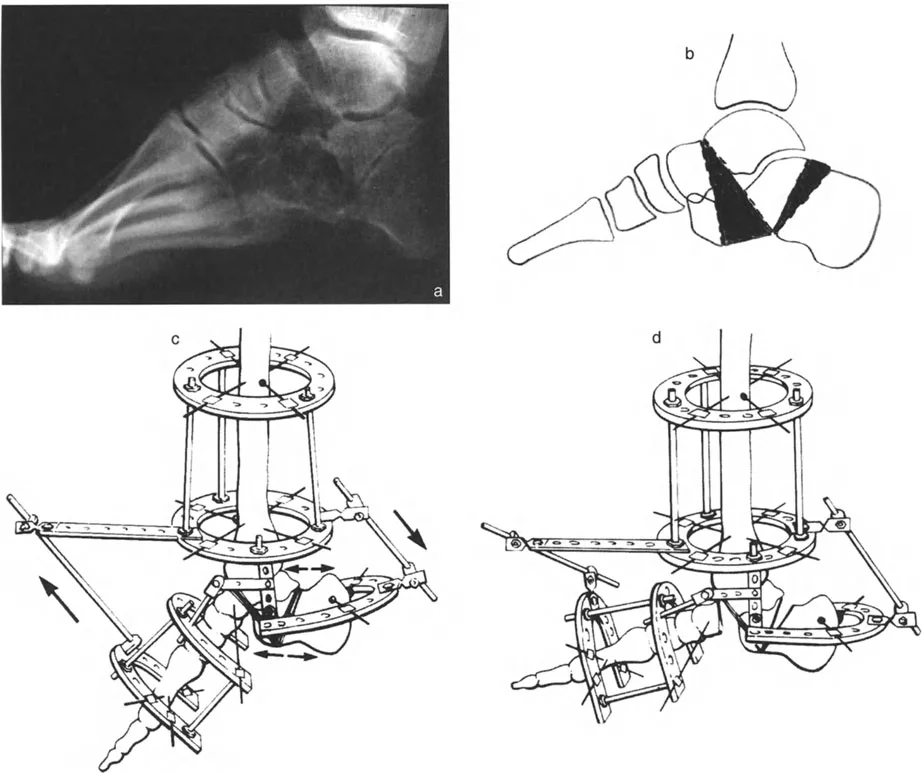
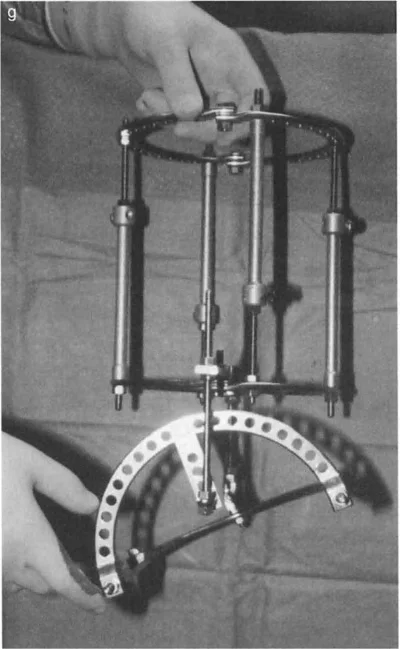
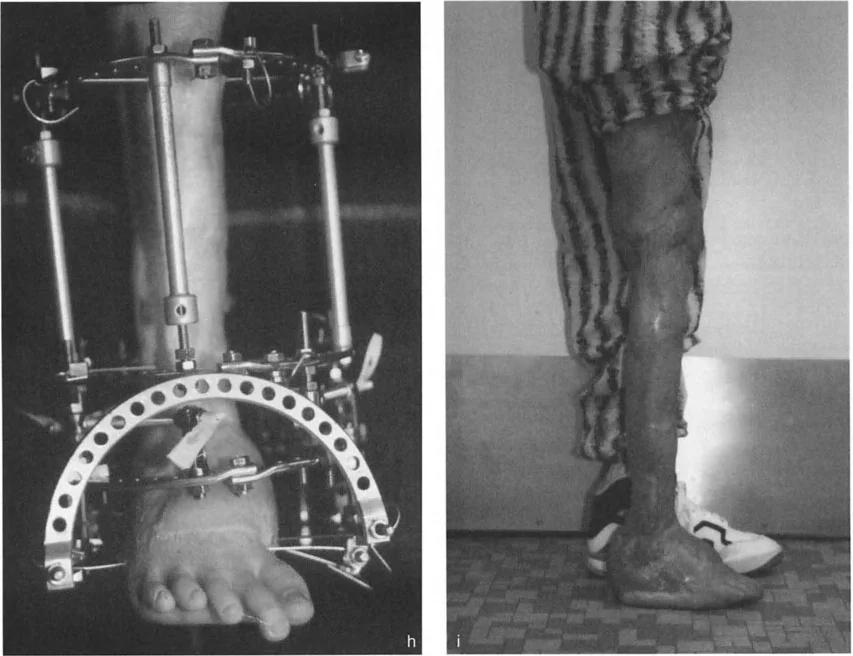
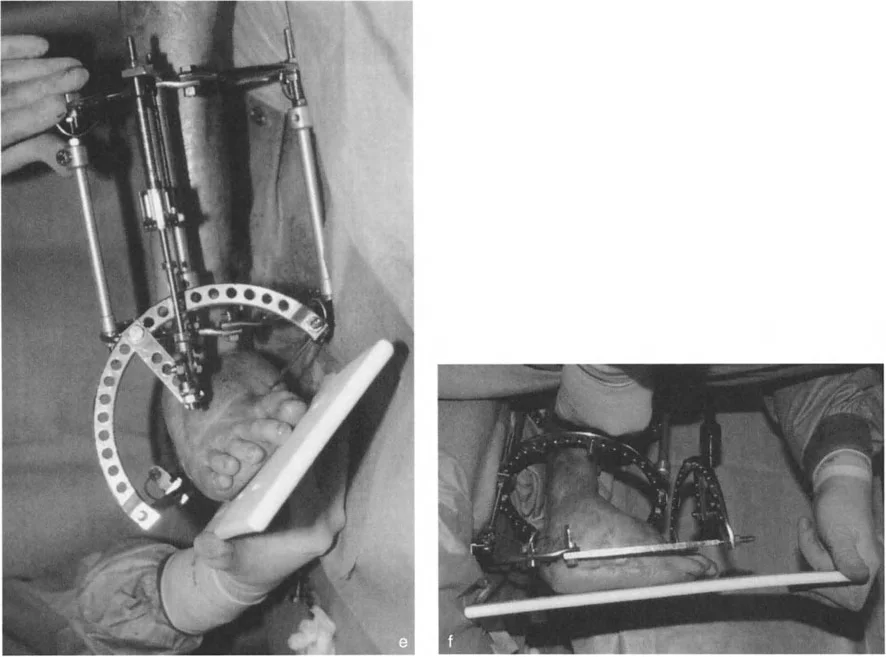
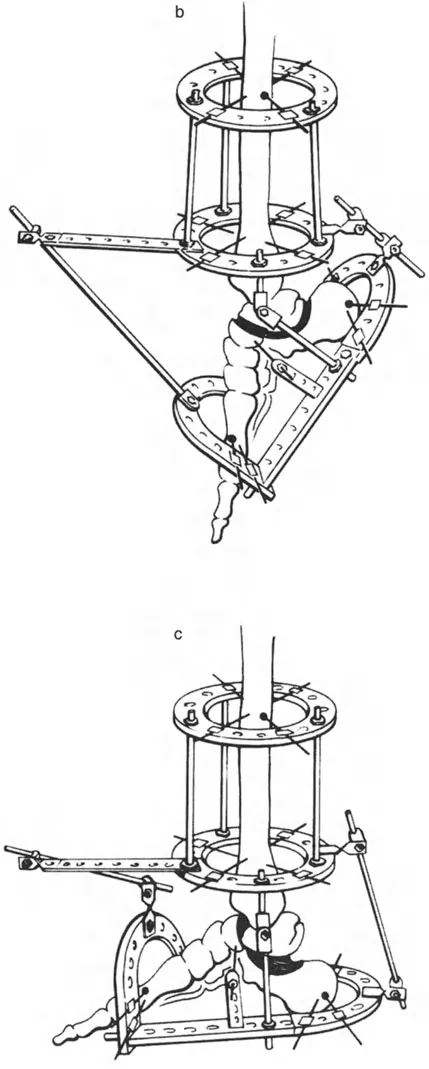
Circular fixators, such as the Taylor Spatial Frame or Ilizarov apparatus, are the gold standard for complex distal tibial deformities. They utilize the concept of a "virtual hinge."
By programming the exact location of the CORA into the software, the hexapod struts adjust over time, executing a flawless Paley Rule Two correction. The bone ends translate and angulate simultaneously, perfectly restoring the mechanical axis without requiring the surgeon to manually calculate the translation during the operation.
Surgical Pearls for Circular Fixation:
* Always mount the reference ring strictly orthogonal to the reference bone segment.
* Use olive wires to prevent translation of the bone on the ring during correction.
* Ensure the fibula is osteotomized at a different level than the tibia to prevent cross-union.
Internal Fixation with Plates and Intramedullary Nails
When utilizing internal fixation, the correction is acute. This requires the surgeon to manually achieve the translation and angulation on the operating table before securing the hardware.
When using an intramedullary nail for a distal deformity, the "wedge effect" of the wide metaphysis will naturally force the nail to the center of the canal, often recreating the deformity. To combat this, Poller screws (blocking screws) are essential. Placed on the concavity of the deformity, they artificially narrow the medullary canal, forcing the nail to follow the corrected mechanical axis.
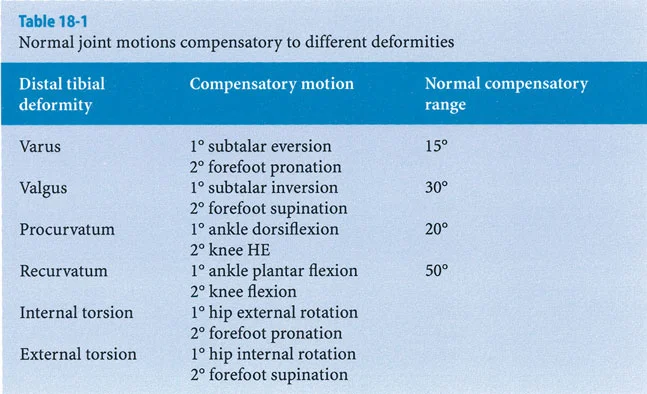

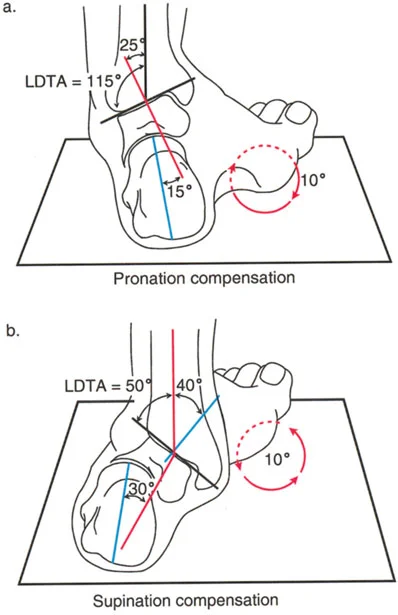
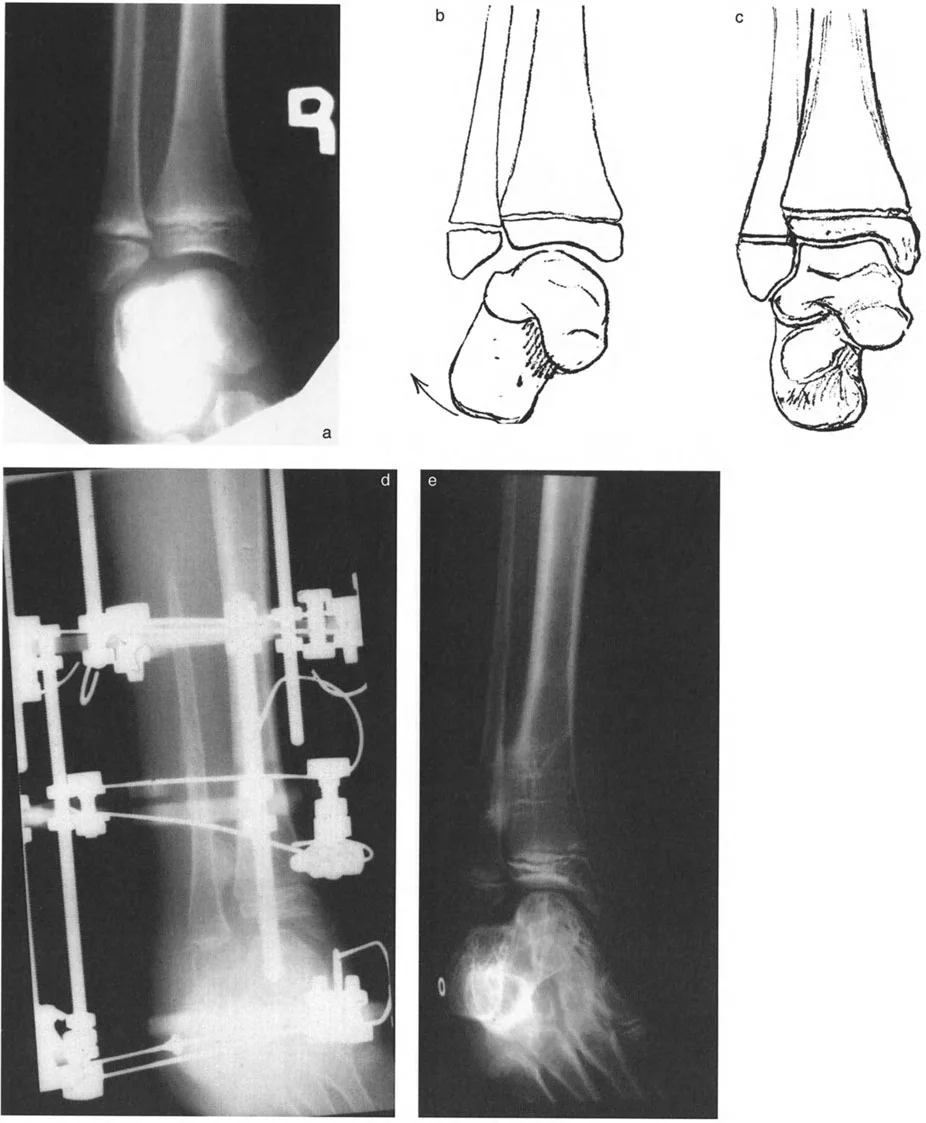
Managing Subtalar and Hindfoot Compensation
The most common pitfall in distal tibial deformity correction is failing to account for the subtalar joint. The subtalar joint is a powerful compensator for tibial malalignment.
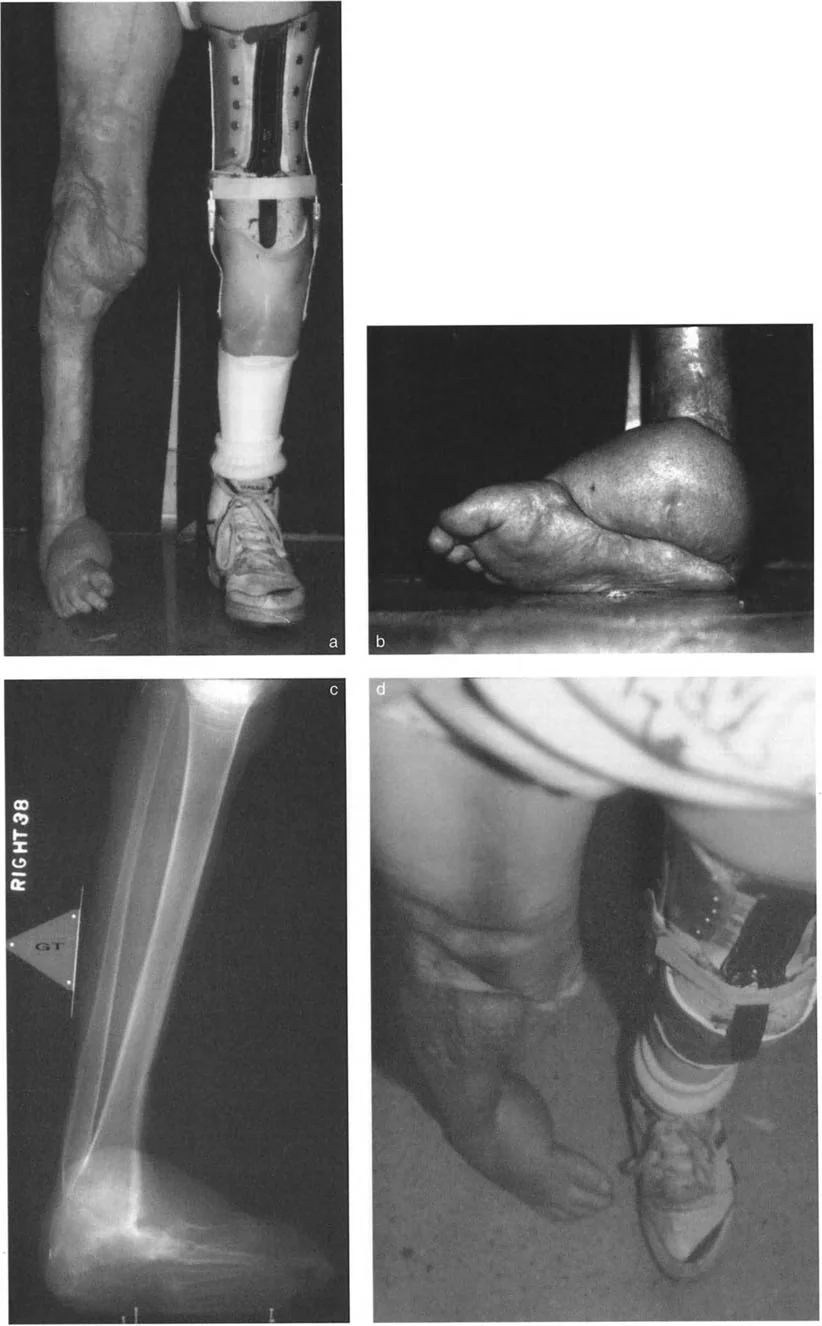
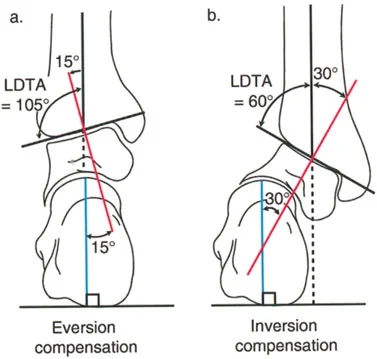
Recognizing Rigid Versus Flexible Deformities
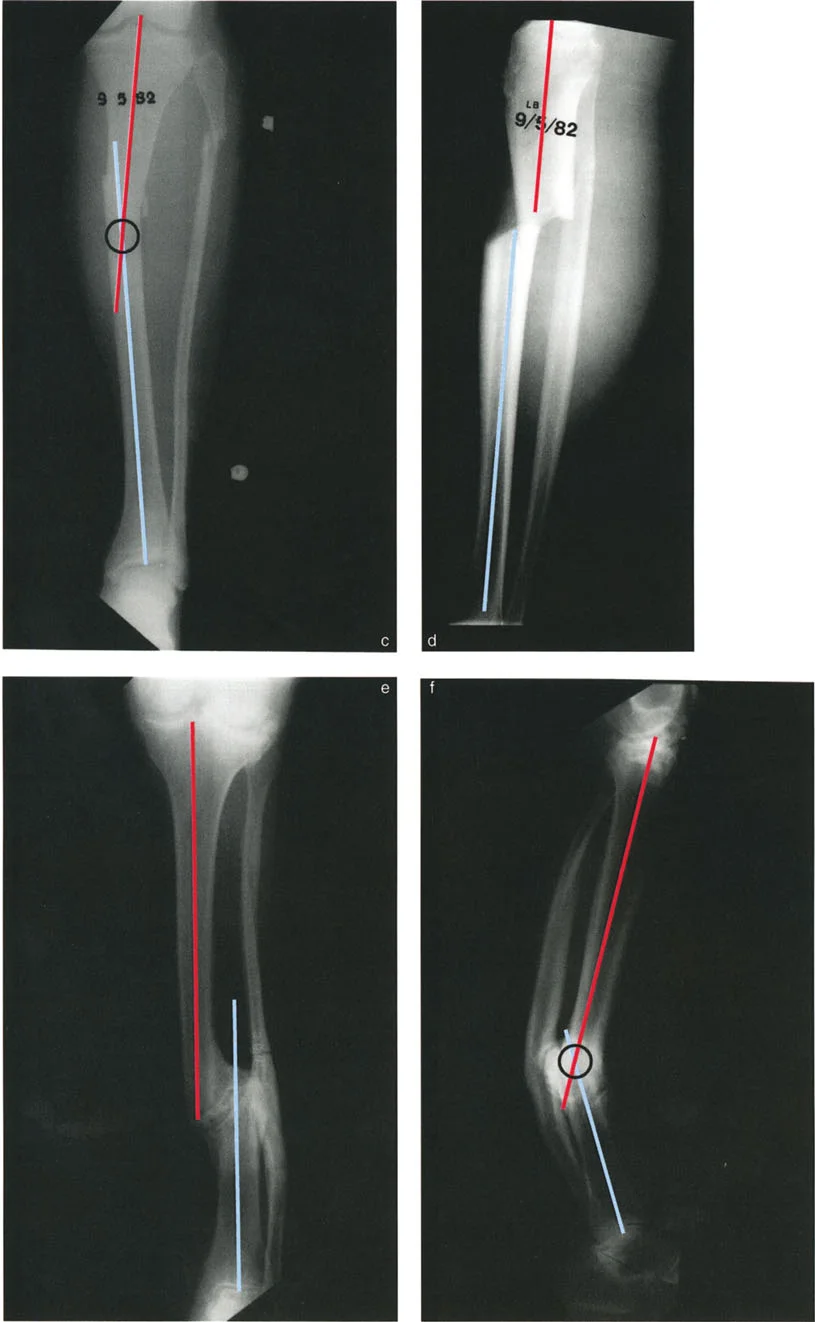
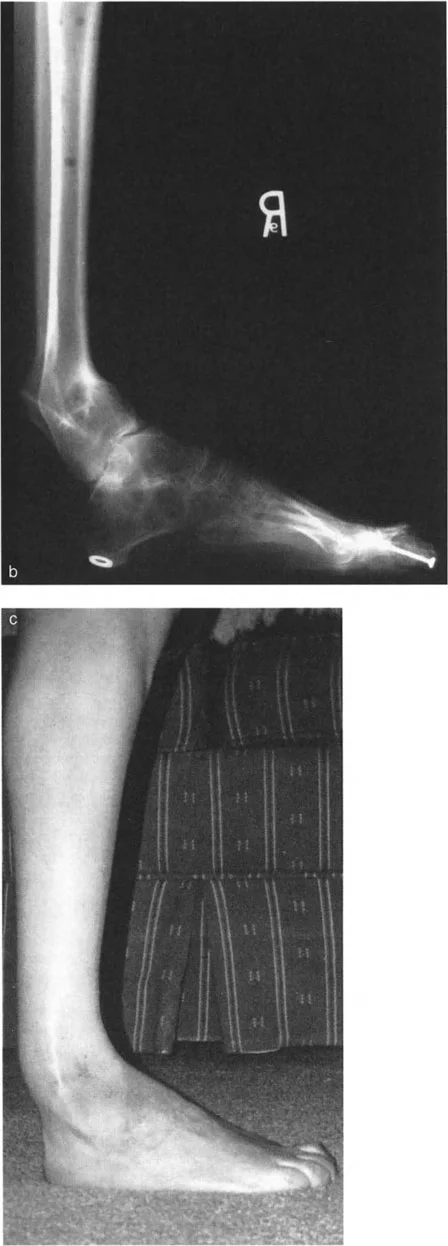
In a patient with a long-standing varus deformity of the distal tibia, the subtalar joint will evert (valgus) to allow the plantar surface of the foot to remain flat on the ground. Over years, this compensatory valgus can become rigid due to soft tissue contracture and joint remodeling.
If the surgeon acutely corrects the tibial varus to neutral, but the subtalar joint remains locked in compensatory valgus, the patient will be left with a severe, unplantable valgus foot.
Key Takeaways for Hindfoot Assessment:
* Always test subtalar flexibility preoperatively using the Coleman block test.
* If the subtalar joint is flexible, it will spontaneously realign once the tibia is corrected.
* If the subtalar joint is rigid, the surgeon must either under-correct the tibia to accommodate the foot, or plan a simultaneous hindfoot osteotomy/fusion to achieve a plantigrade foot.
Addressing Iatrogenic Translation
Iatrogenic translation occurs when Paley Rule Three is inadvertently applied, or when the fibula prevents proper mobilization of the tibial segments.
The fibula acts as a lateral strut. In almost all distal tibial corrections, a fibular osteotomy is mandatory. If the fibula is intact, it will act as a tether, forcing the tibia into valgus or preventing necessary translation. The fibular cut should be oblique to increase surface area for healing, and it must be positioned away from the tibial osteotomy site.






!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like