Precision Knee Osteotomy: Applying Paley Principles for Unicompartmental OA
Key Takeaway
Paley Principles guide precise knee realignment osteotomy for unicompartmental osteoarthritis. They use CORA, Mechanical Axis Deviation, and joint orientation angles to correct complex multi-planar deformities. This approach redistributes loads, preserves the knee joint, and restores optimal kinematics.
Realignment for Mono Compartment Osteoarthritis of the Knee
The management of mono-compartment osteoarthritis of the knee represents a complex biomechanical challenge that requires precise surgical planning and execution. Joint preservation surgery through realignment osteotomy is a powerful tool for orthopedic surgeons, particularly in young, active patients where arthroplasty is less desirable. The ultimate goal is to redistribute mechanical loads from the diseased compartment to the healthy compartment, thereby alleviating pain, halting disease progression, and restoring optimal lower extremity kinematics.

This comprehensive guide applies the foundational principles of Dr. Dror Paley to the specific clinical scenarios associated with unicompartmental knee disease. By mastering the concepts of the Center of Rotation of Angulation, Mechanical Axis Deviation, and precise joint orientation angles, surgeons can address not only simple coronal plane deformities but complex multi-planar deformities involving torsion, recurvatum, and fixed flexion contractures.
Core Paley Principles in Knee Realignment
To successfully correct deformities associated with mono-compartment osteoarthritis, the surgeon must completely internalize the Paley framework for deformity analysis. Deformity correction is not merely about making a bone look straight on a radiograph; it is about restoring the mechanical axis and joint orientation to normal or planned overcorrected values.
Mechanical Axis Deviation
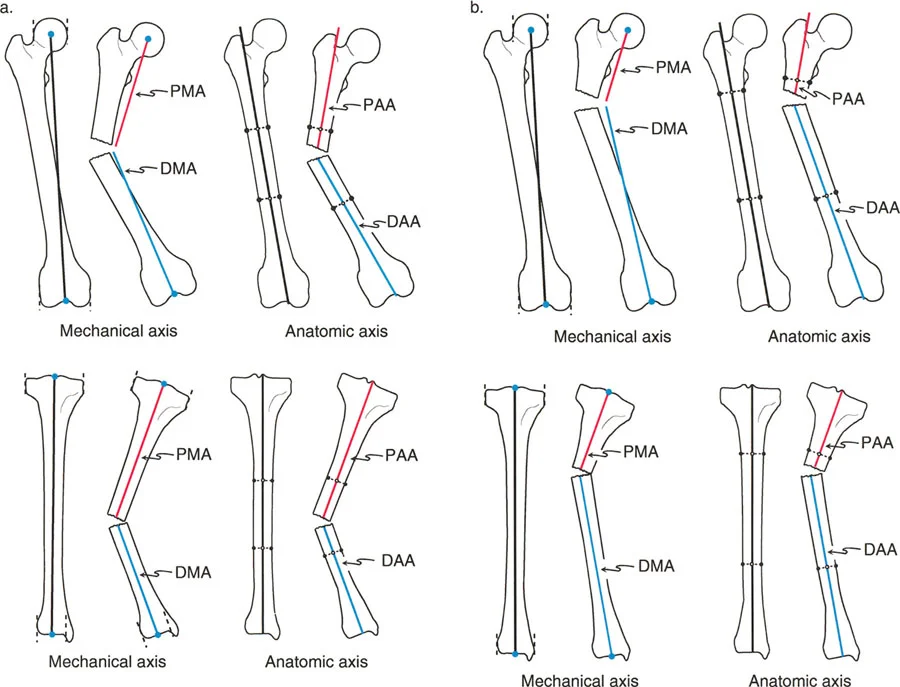
The Mechanical Axis Deviation is the foundational metric in lower extremity realignment. The mechanical axis of the lower limb is a line drawn from the center of the femoral head to the center of the ankle joint. In a normal limb, this line passes slightly medial to the center of the knee joint.
In medial mono-compartment osteoarthritis, the mechanical axis shifts medially, creating a varus deformity and overloading the medial compartment. The goal of realignment osteotomy is to shift the Mechanical Axis Deviation laterally, typically to the center of the lateral compartment (or slightly lateral to the lateral tibial spine), to offload the medial articular cartilage.
Joint Orientation Angles
Understanding normal joint orientation angles is critical for identifying whether the deformity originates in the femur, the tibia, or the joint space itself.
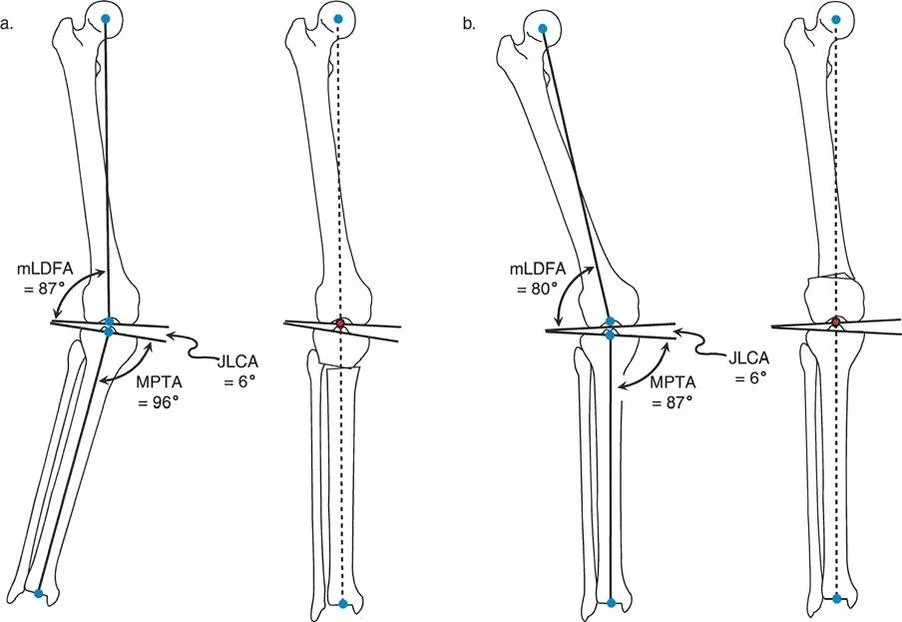
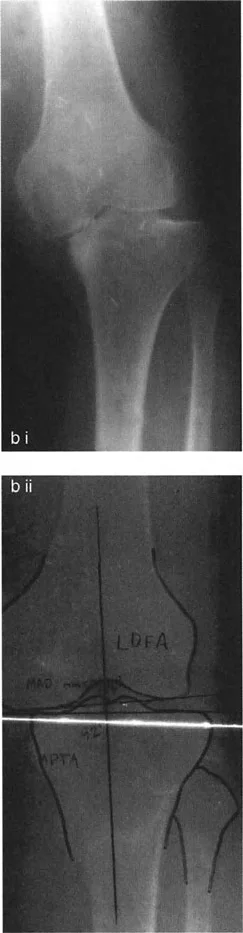
- mLDFA (Mechanical Lateral Distal Femoral Angle): The lateral angle formed between the mechanical axis of the femur and the knee joint line. Normal is approximately 87 degrees.
- MPTA (Medial Proximal Tibial Angle): The medial angle formed between the mechanical axis of the tibia and the knee joint line. Normal is approximately 87 degrees.
- JLCA (Joint Line Convergence Angle): The angle between the distal femoral articular line and the proximal tibial articular line. Normal is 0 to 2 degrees. An increased JLCA often indicates ligamentous laxity or cartilage wear.
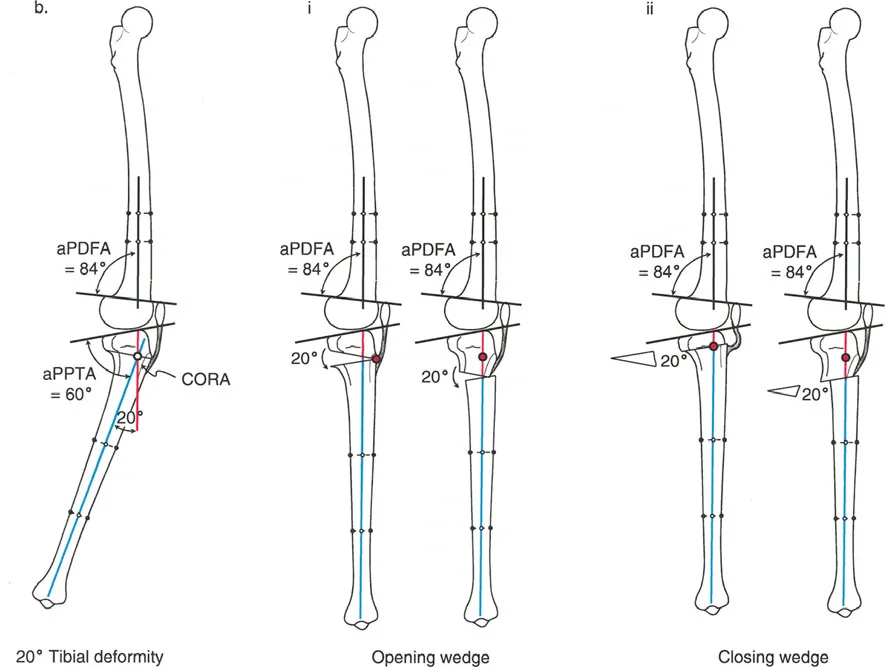
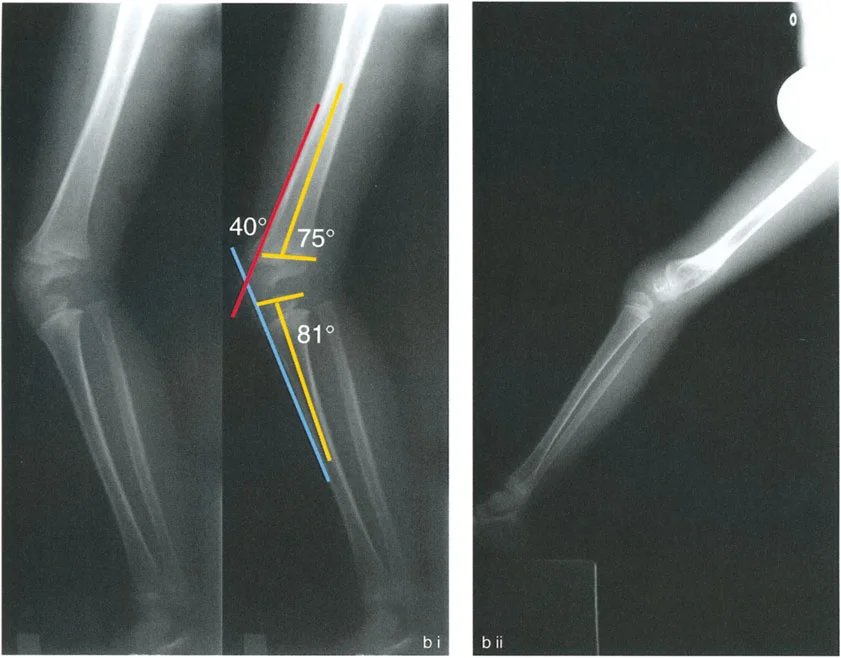
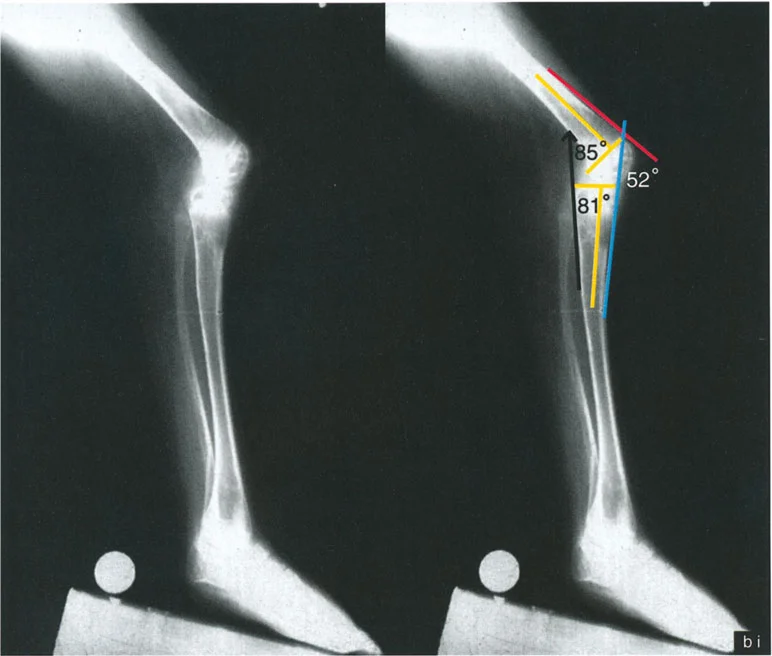
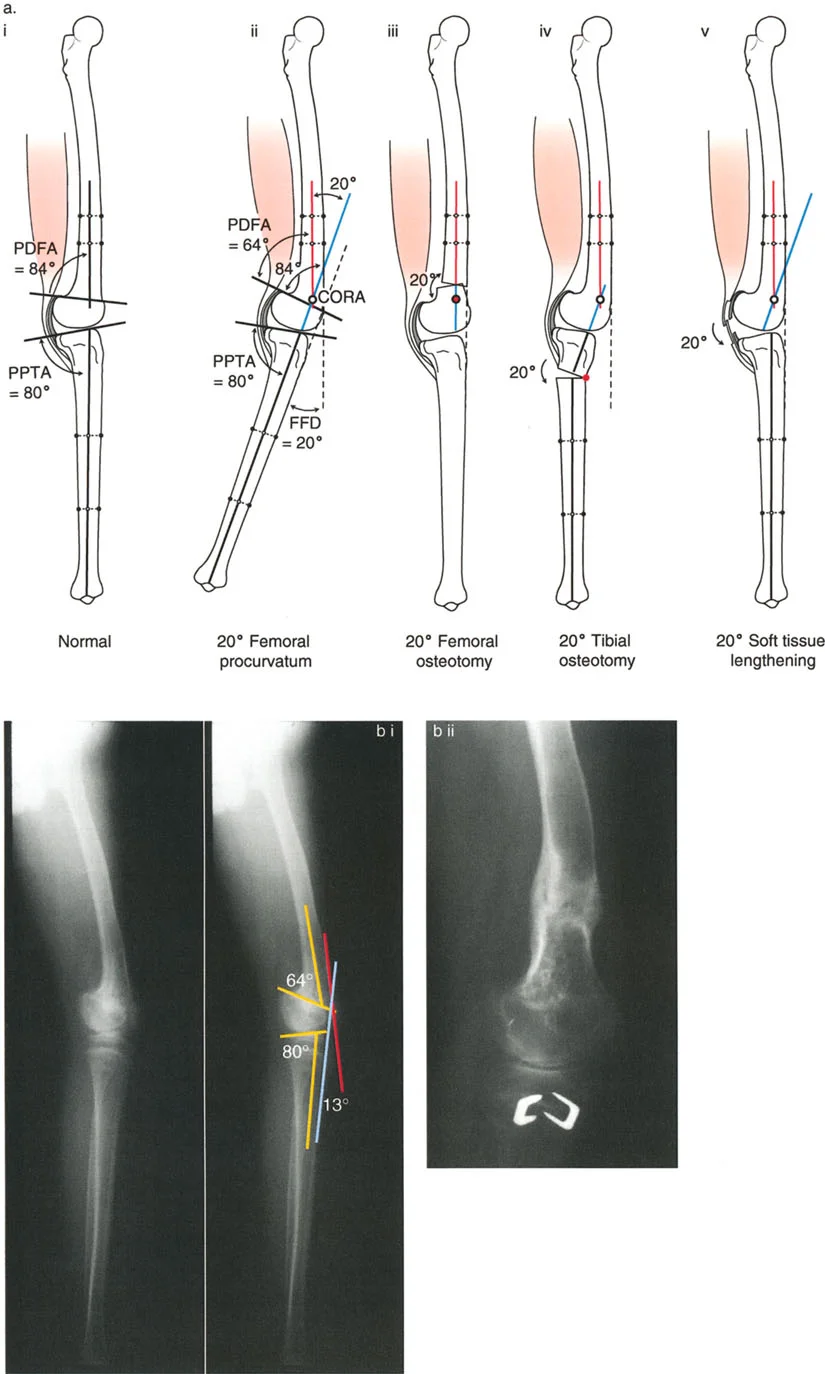
- aPPTA (Anterior Proximal Tibial Angle): Evaluated on the lateral radiograph, this is the angle between the anatomic axis of the tibia and the joint line. Normal is approximately 81 degrees.
- aPDFA (Anterior Proximal Distal Femoral Angle): Evaluated on the lateral radiograph, representing the sagittal distal femoral joint orientation. Normal is approximately 83 degrees.
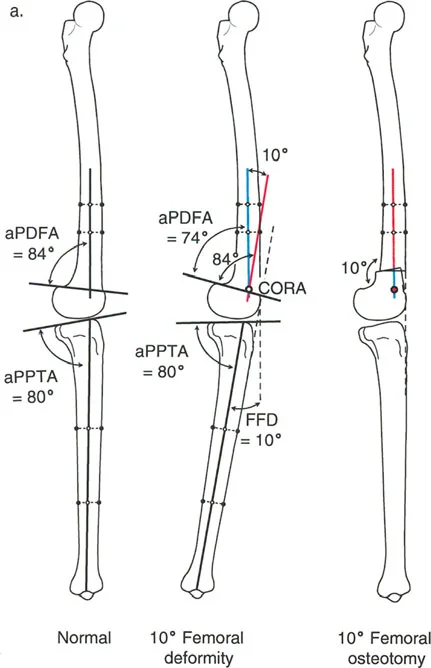
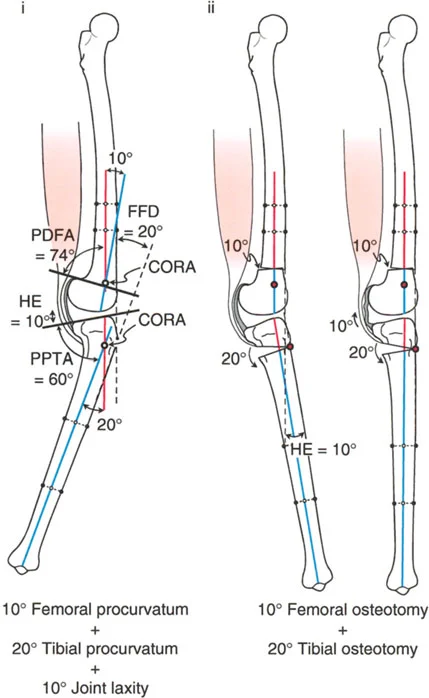
The Center of Rotation of Angulation
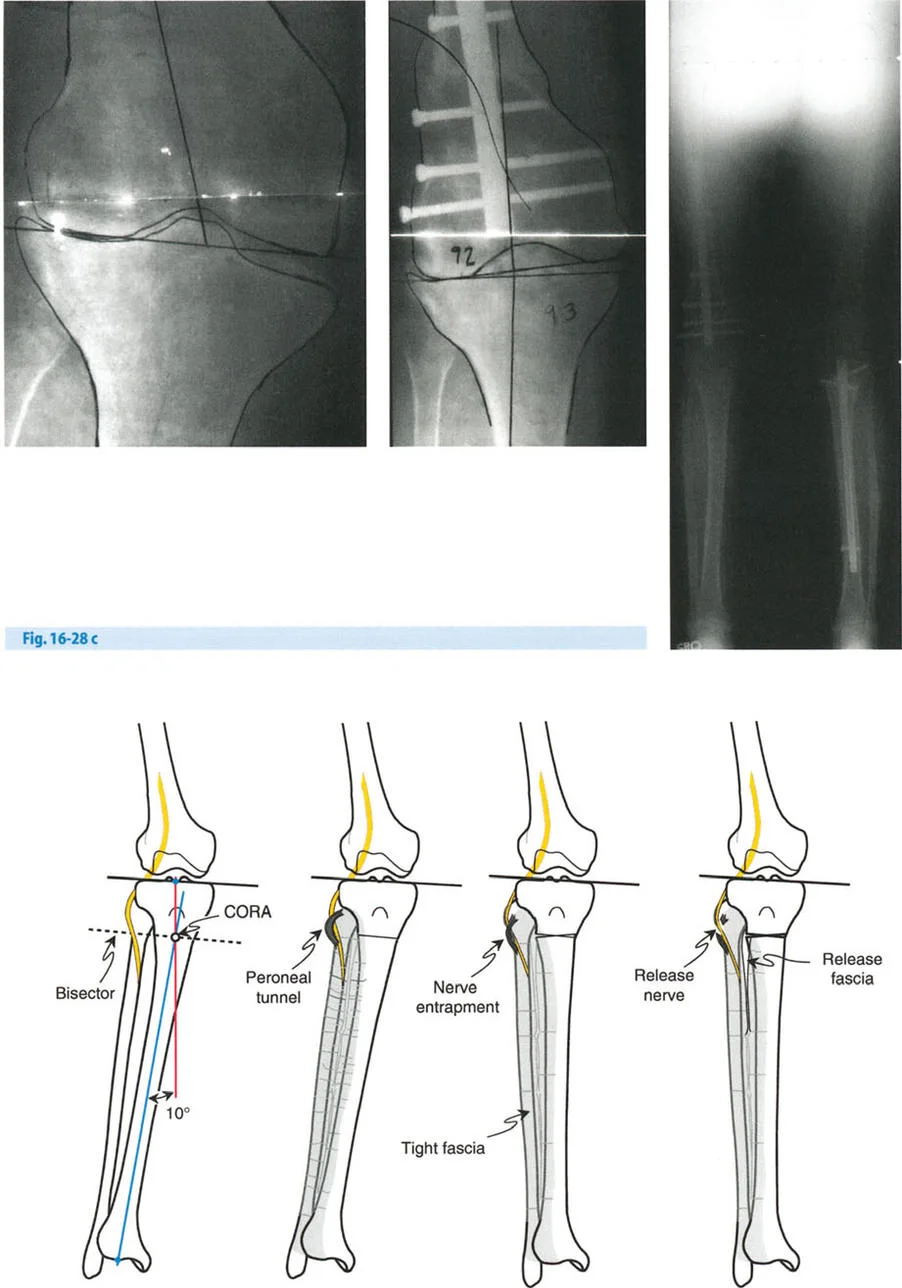
The Center of Rotation of Angulation represents the intersection of the proximal and distal mechanical (or anatomic) axis lines of a deformed bone. Identifying the Center of Rotation of Angulation is the most critical step in preoperative planning.
Paley established three fundamental osteotomy rules based on the Center of Rotation of Angulation:
1. Rule 1: If the osteotomy and the hinge are both located at the Center of Rotation of Angulation, the bone will realign perfectly without translation.
2. Rule 2: If the osteotomy is located outside the Center of Rotation of Angulation, but the hinge remains at the Center of Rotation of Angulation, the bone will realign, but translation at the osteotomy site will occur.
3. Rule 3: If both the osteotomy and the hinge are located outside the Center of Rotation of Angulation, a secondary translation deformity will be created upon correction.
Preoperative Planning for Knee Osteotomies
Meticulous preoperative planning is the hallmark of successful deformity correction. The surgeon must evaluate the entire lower extremity in weight-bearing conditions to accurately assess the Mechanical Axis Deviation and joint orientation angles.
Radiographic Evaluation Steps
- Standing Full-Length Anteroposterior Radiograph: The patella must be facing directly forward to accurately assess coronal plane alignment and avoid rotational artifact.
- Standing Lateral Radiograph of the Knee: Essential for evaluating sagittal plane deformities such as fixed flexion deformity or genu recurvatum, and for measuring the aPPTA and aPDFA.
- Merchant or Skyline View: Critical for evaluating patellofemoral tracking and joint space narrowing.
- Stress Radiographs: Useful in cases with an abnormal Joint Line Convergence Angle to differentiate between structural bone deformity and ligamentous laxity.

Managing Medial Compartment Osteoarthritis with Axial Plane Deformities
Patients presenting with medial compartment osteoarthritis frequently exhibit complex multi-planar deformities. One of the most challenging combinations is varus deformity coupled with external tibial torsion and patellofemoral maltracking.
External Tibial Torsion and Patellofemoral Maltracking
When evaluating a standing long anteroposterior radiograph of a patient with varus deformity and external tibial torsion, the surgeon will note that when the patella is facing forward, the ankle and fibula appear externally rotated relative to the tibia. This rotational malalignment exacerbates patellofemoral maltracking, leading to anterior knee pain and accelerated cartilage wear.
To correct this, a valgus realignment osteotomy combined with internal rotation of the distal segment is required. The level of the osteotomy relative to the tibial tuberosity is of paramount importance.
- Osteotomy Proximal to the Tuberosity: If the osteotomy (either a straight cut or an L-cut) is made proximal to the tibial tuberosity, internal rotation of the distal segment will cause the patellar tendon insertion to displace medially. This medialization effectively realigns the patellofemoral mechanism, correcting the maltracking.
- The L Shaped Osteotomy: Rotating the bone ends when the osteotomy is located above the tuberosity is technically demanding due to the large metaphyseal surface area and robust soft tissue attachments. To facilitate rotation above the tuberosity and to maximize the bone stock available for fixation of the proximal segment, an L-shaped osteotomy is highly recommended.
Key Surgical Pearls for Axial Plane Correction
- Assess Patellar Height: Always evaluate the Caton-Deschamps index preoperatively. Opening wedge osteotomies distal to the tuberosity lower the patella (patella baja), while closing wedge osteotomies proximal to the tuberosity raise the patella.
- Fibula Management: Rotational corrections require careful management of the fibula. A proximal tibiofibular joint release or a mid-shaft fibular osteotomy is mandatory to allow for unimpeded rotation of the distal tibial segment.
Managing Medial Compartment Osteoarthritis with Sagittal Plane Deformities
Sagittal plane deformities, namely genu recurvatum (hyperextension) and fixed flexion deformities, drastically alter knee kinematics. Failure to address these sagittal plane issues during coronal realignment will lead to suboptimal clinical outcomes and persistent pain.
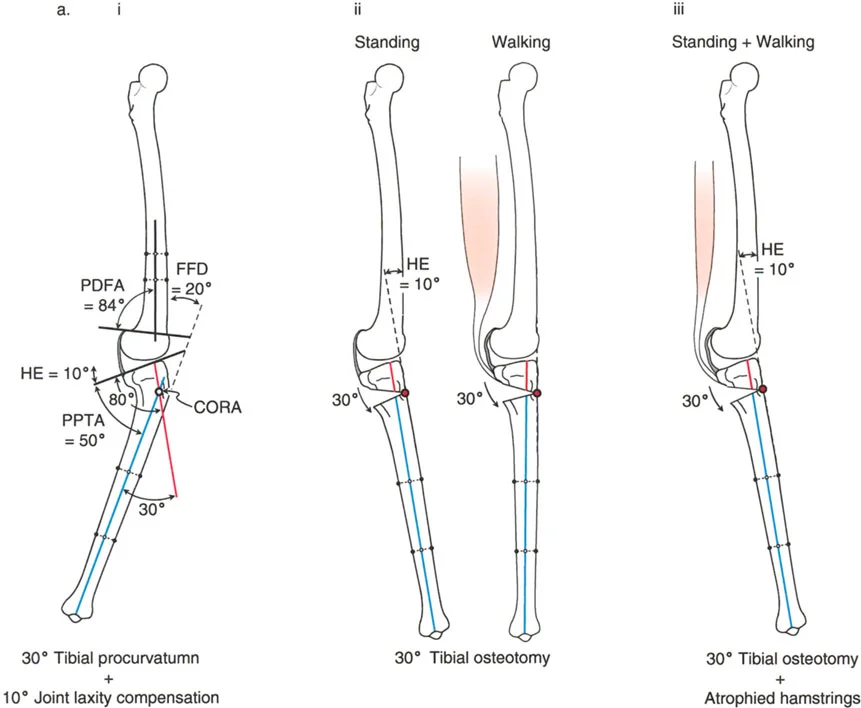
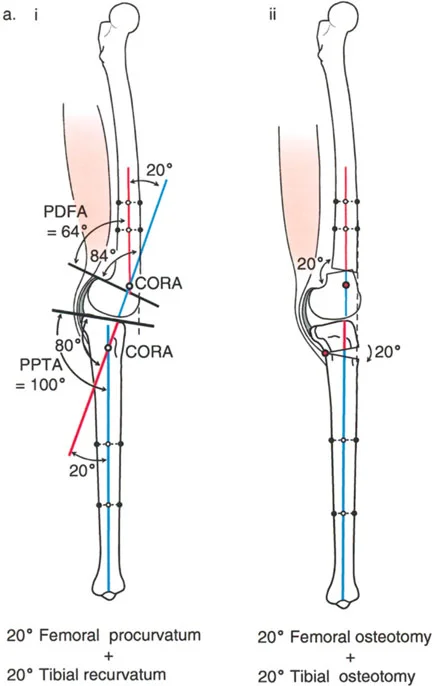
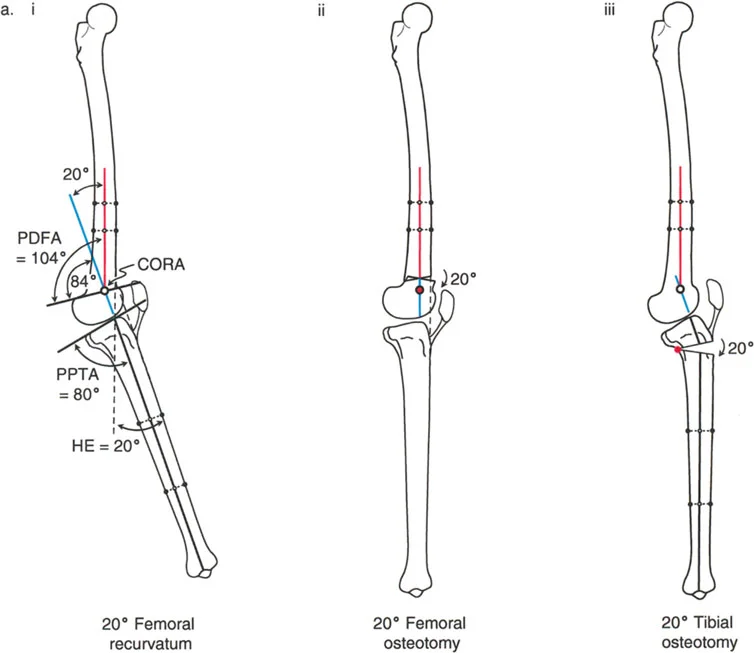
Varus Deformity with Genu Recurvatum
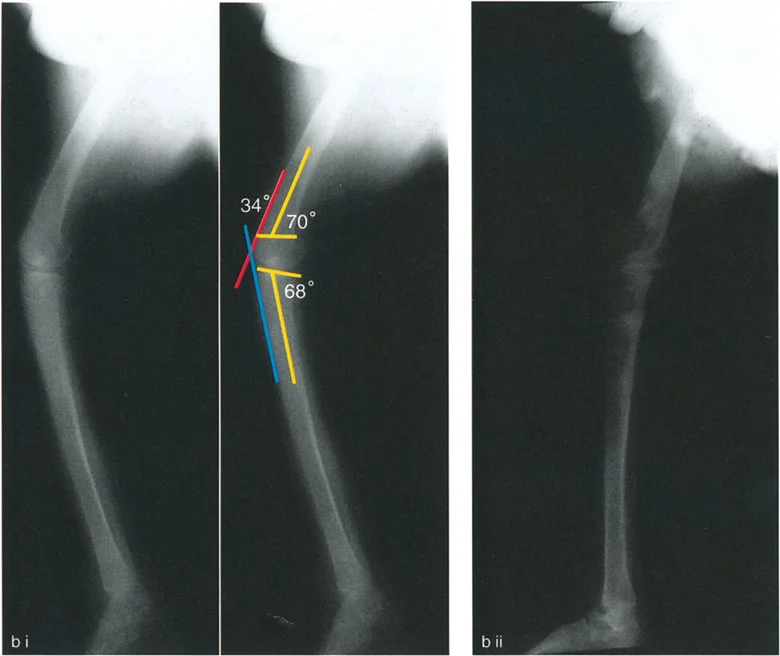
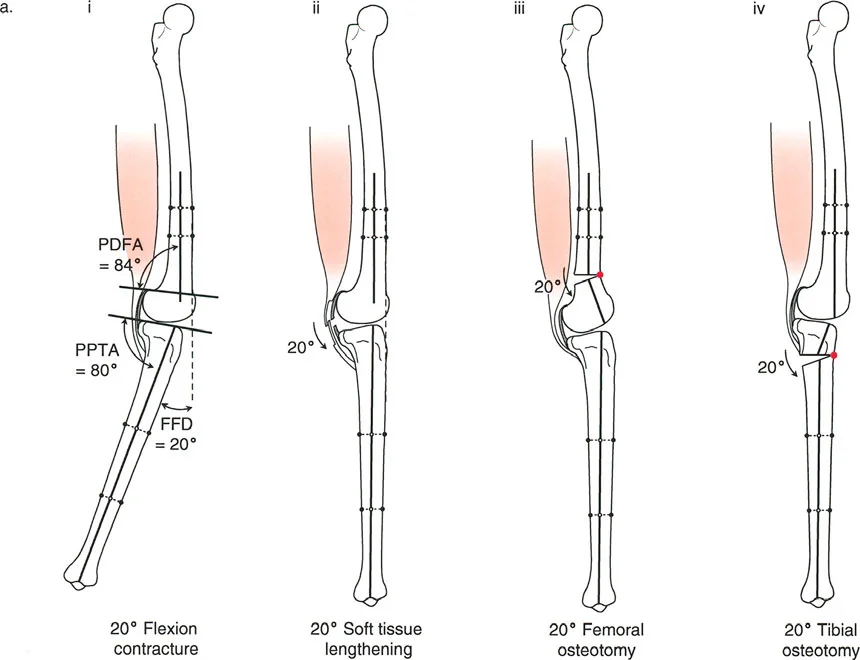
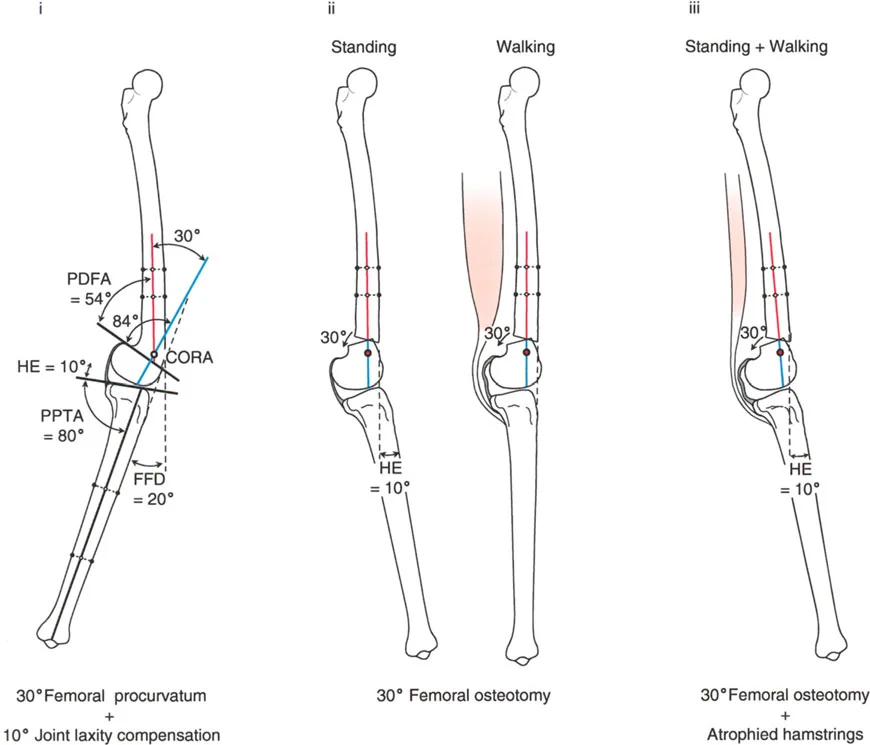
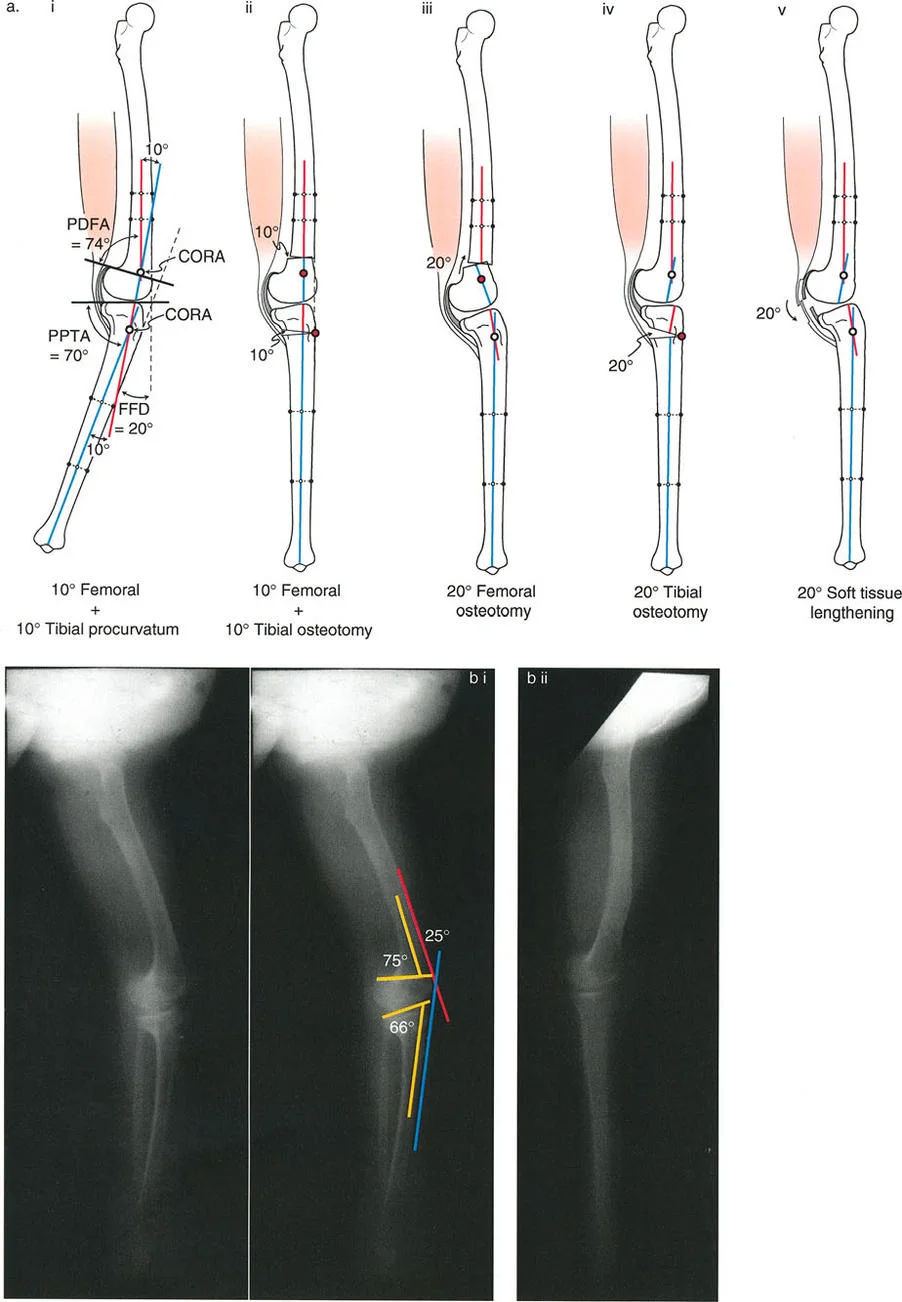
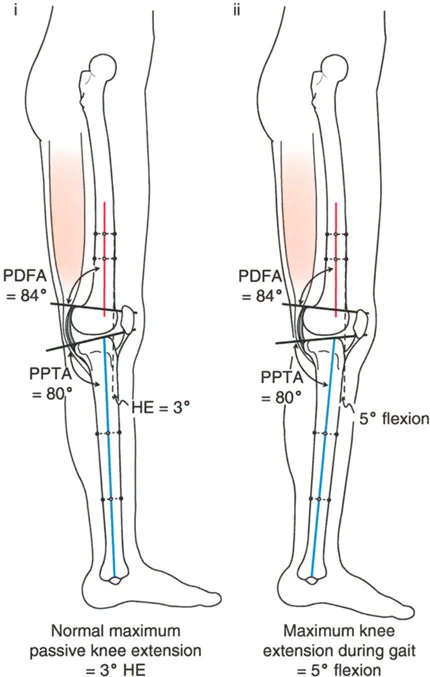
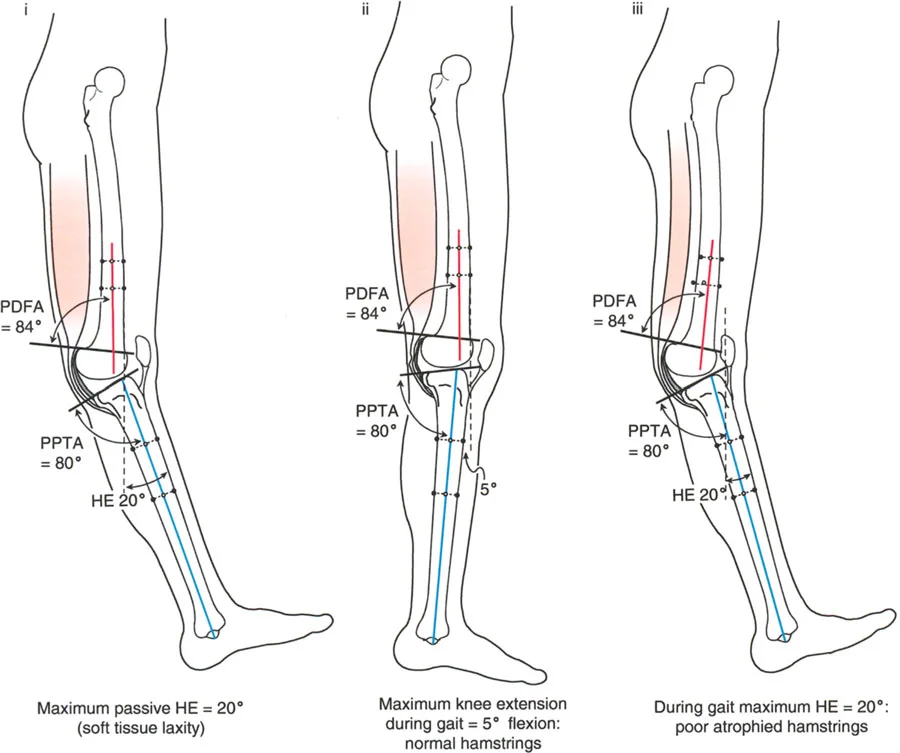
Genu recurvatum, or knee hyperextension, requires careful localization of the deformity. The surgeon must first determine if the recurvatum originates in the femur or the tibia by measuring the aPDFA and aPPTA.
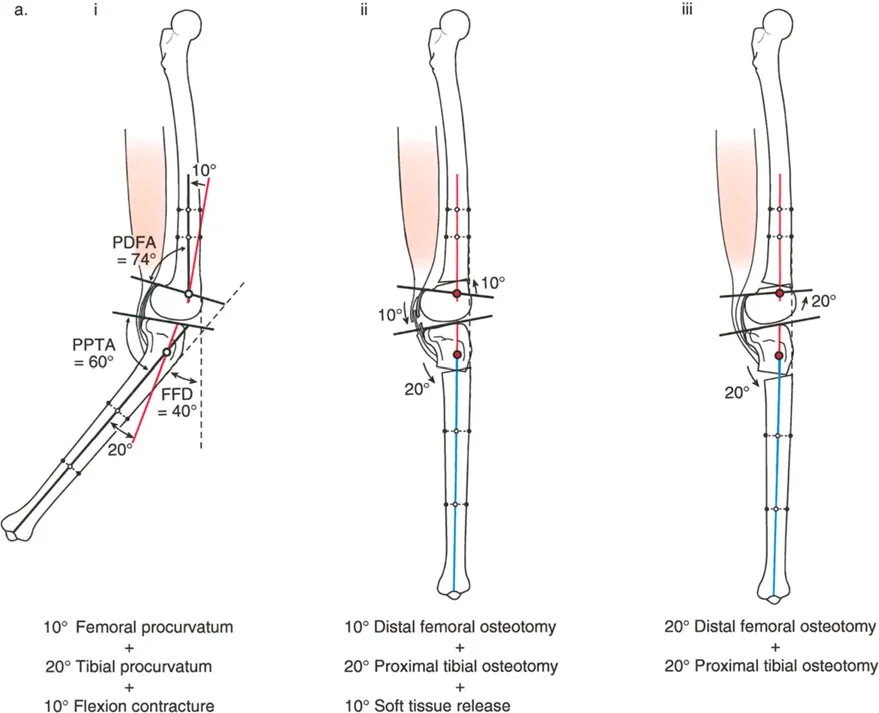
If the recurvatum deformity is localized to the femur, it must be corrected via a distal femoral osteotomy, matching the correction to the exact amount of hyperextension present in the knee.
If the recurvatum is localized to the tibia, the varus deformity is treated either proximal or distal to the tibial tuberosity. The decision is dictated by the preexisting distance of the tuberosity to the joint line:
- Normal Patellar Tendon Level: If the patellar tendon insertion is at a normal level relative to the knee joint line, the osteotomy should be performed distal to the tibial tuberosity. An oblique plane correction is then executed to address both the varus and the recurvatum simultaneously.
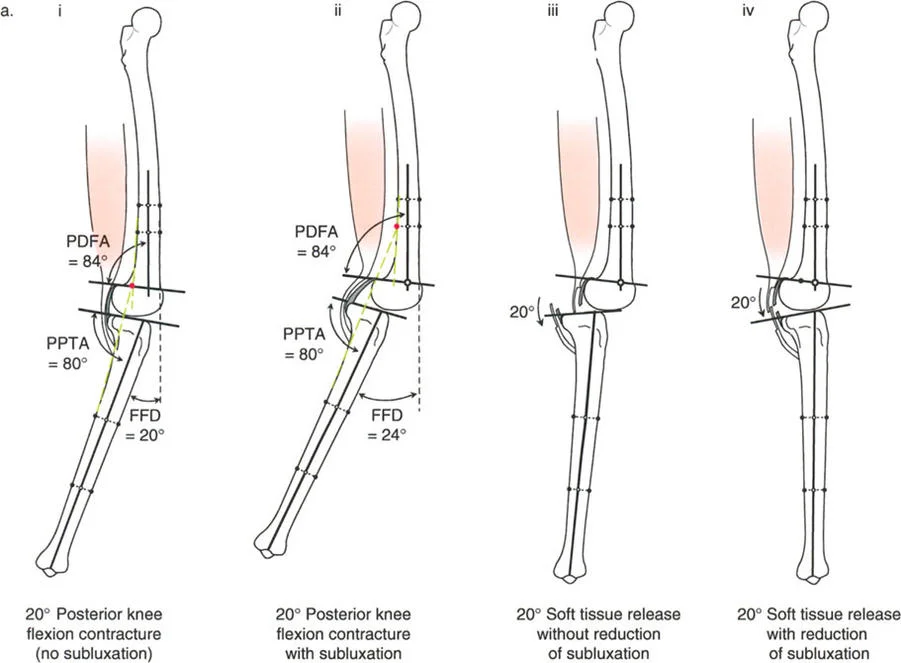
- Abnormally Proximal Patellar Tendon: In cases where the patellar tendon insertion is abnormally proximal and the tibia is posteriorly subluxed on the femur, the osteotomy must be performed proximal to the tibial tuberosity.
Performing the osteotomy proximal to the tuberosity in cases of proximal insertion serves a dual biomechanical purpose. It allows the surgeon to reduce the tibia using the leverage produced by the patella acting on the anterior femoral condyles. Furthermore, additional reduction and stability can be achieved by performing a distal transport of the proximal fibula, a maneuver that effectively tightens the lateral collateral ligament complex.
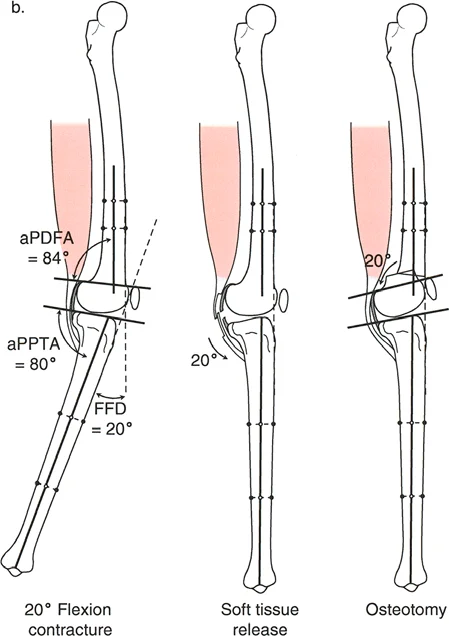
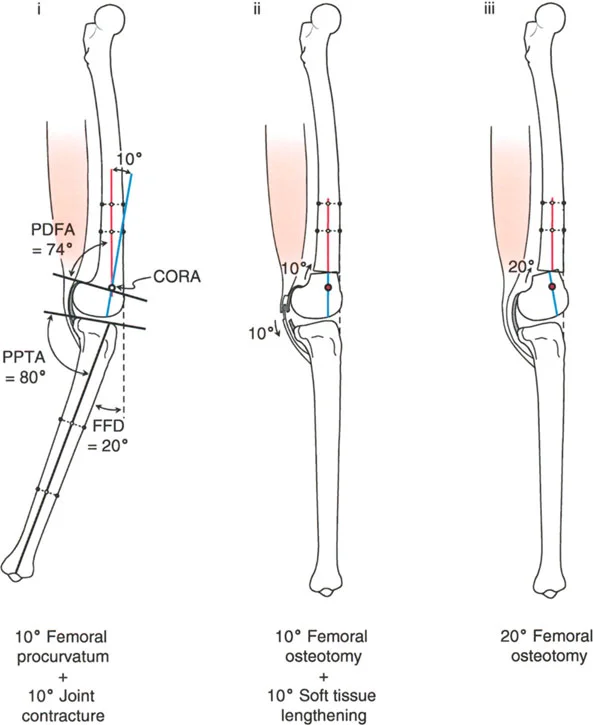
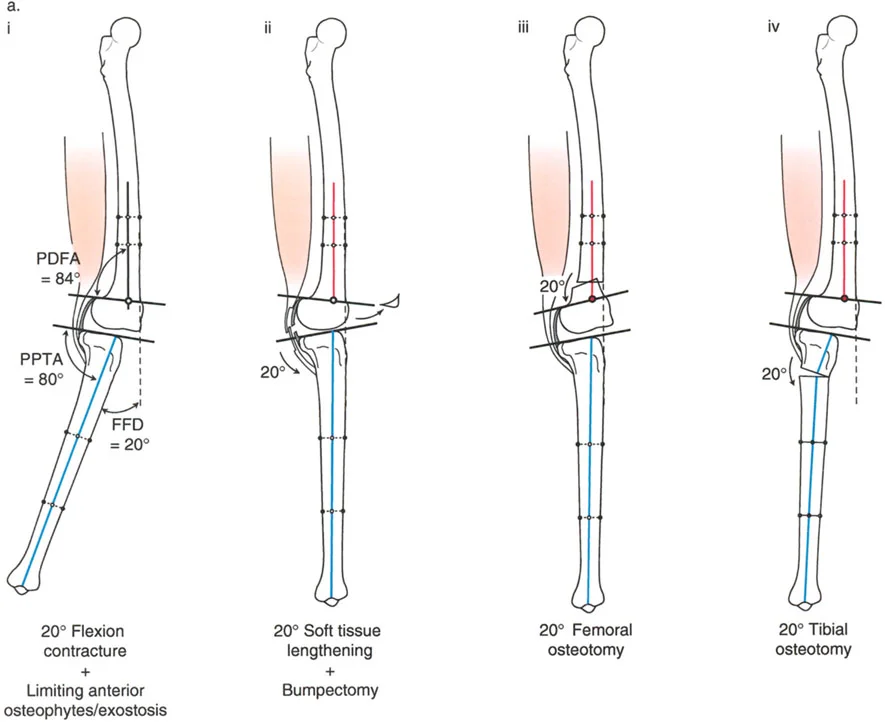
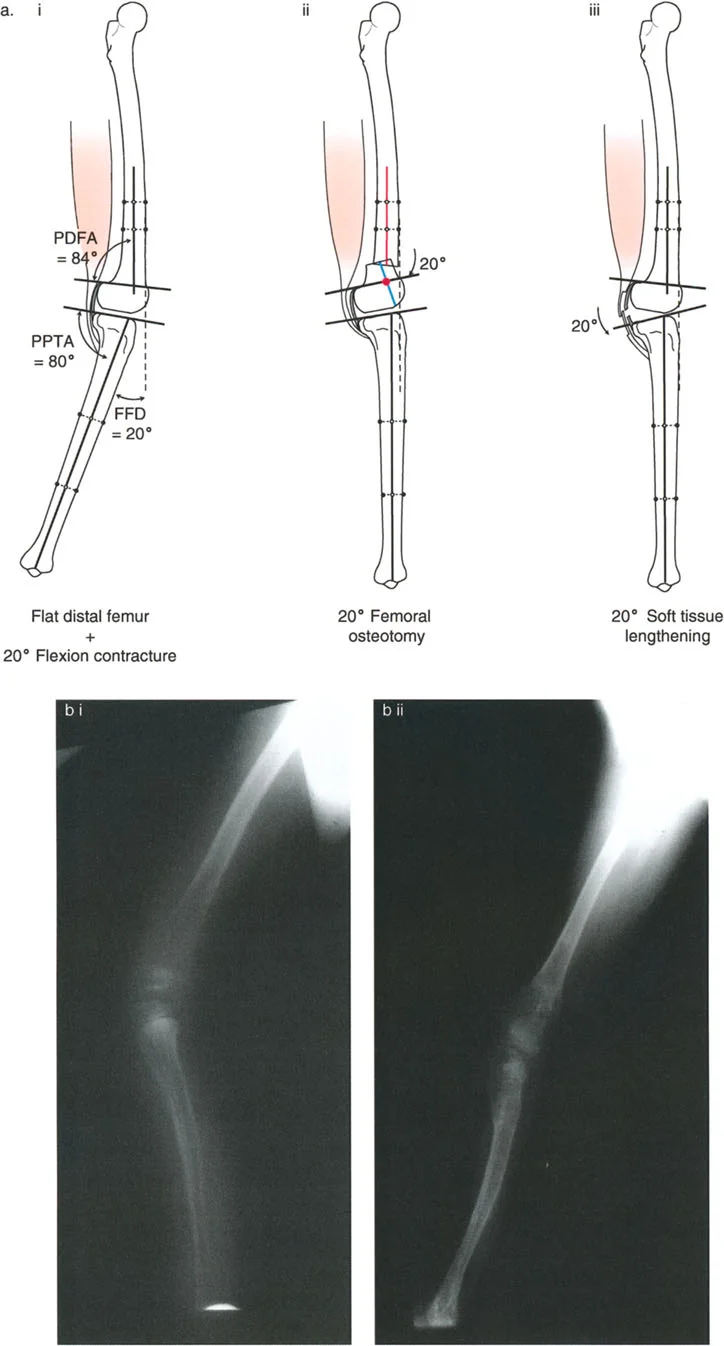
Varus Deformity with Fixed Flexion Deformity
A fixed flexion deformity of the knee must be completely eliminated during the treatment of unicompartmental osteoarthritis. Persistent flexion contractures lead to anterior impingement of the femur and tibia during the stance phase of gait, causing debilitating pain and rapid wear of the remaining cartilage.
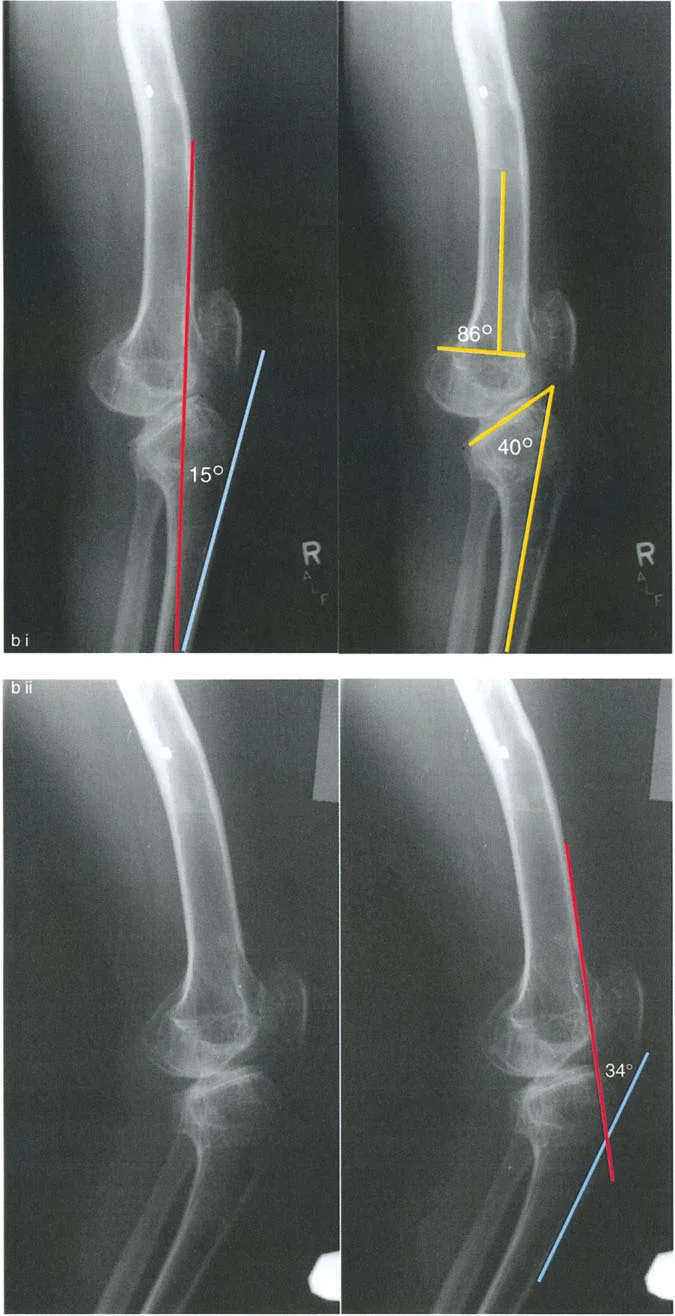
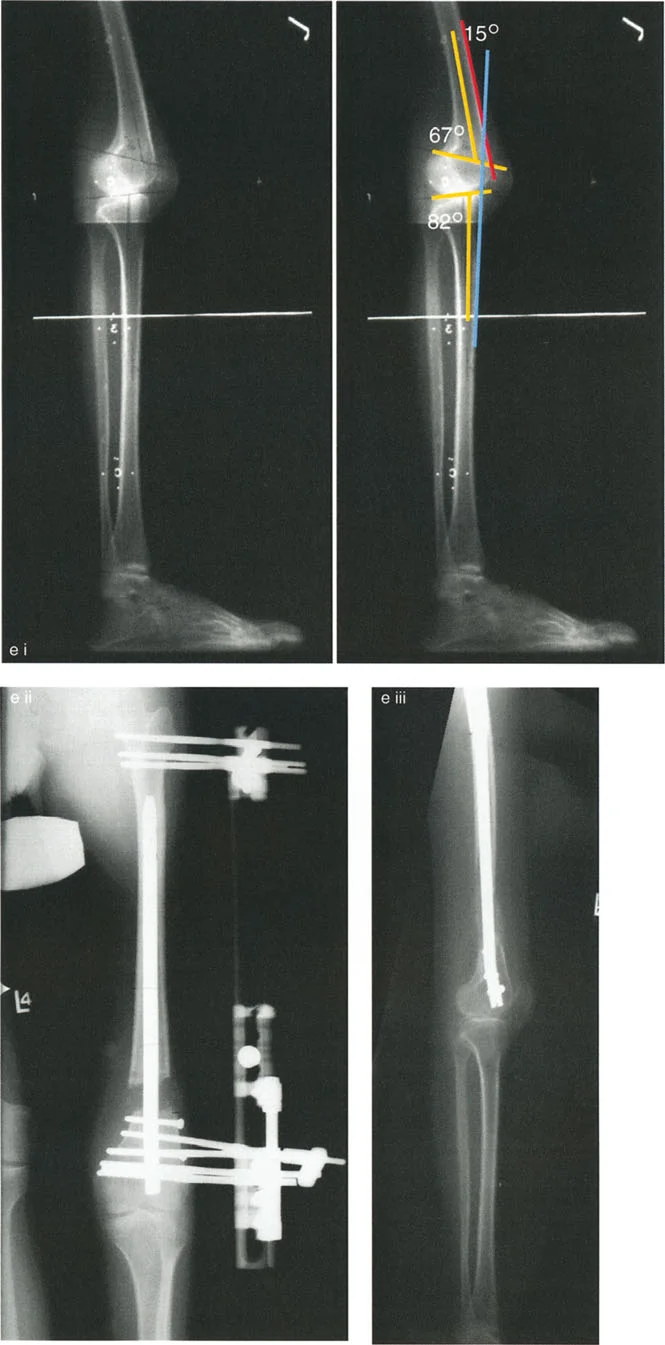
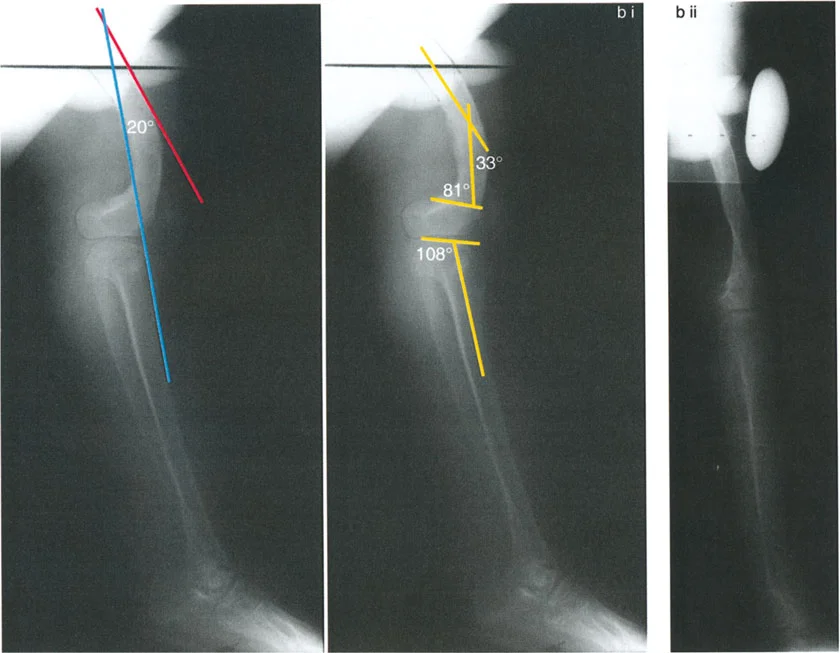
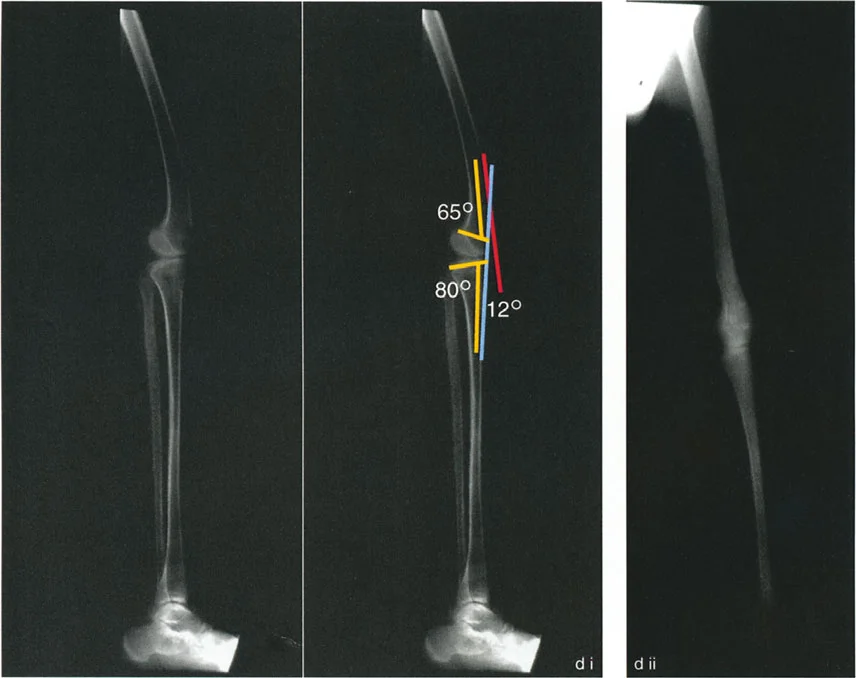
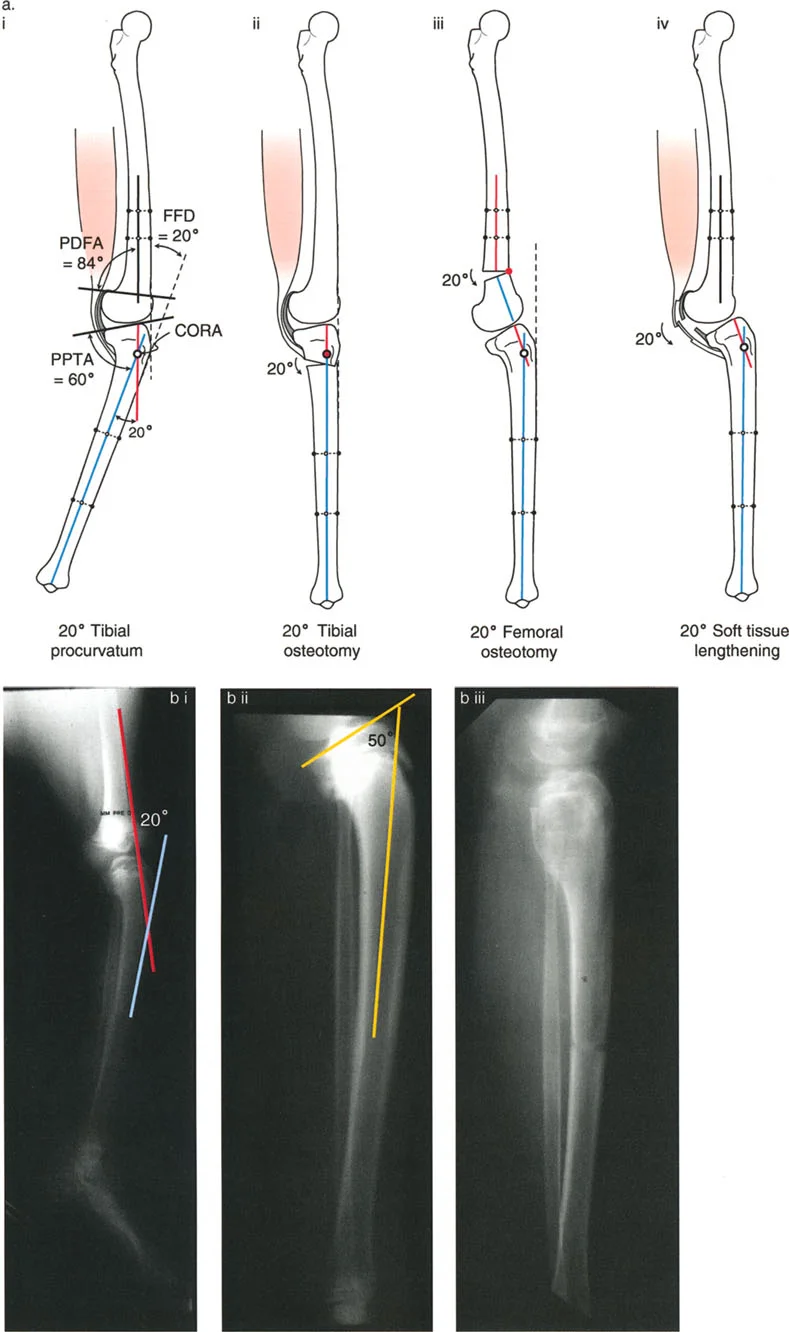
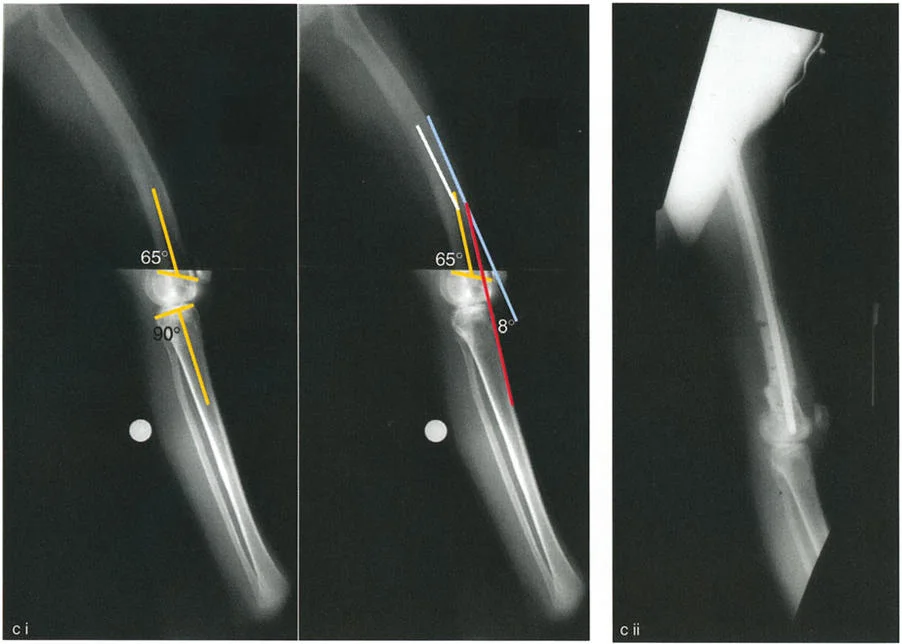
The lateral radiograph is the primary diagnostic tool. The surgeon must measure the aPPTA and aPDFA to identify any underlying procurvatum deformity of the femur or tibia.
- Addressing Procurvatum: If a procurvatum deformity is identified in either bone, an extension osteotomy of that specific bone is warranted. When correcting the tibia, the aPPTA may be corrected up to 90 degrees.
- The 90 Degree Rule: Overcorrection of the aPPTA beyond 90 degrees is strictly contraindicated. Exceeding 90 degrees results in the loss of the critical anterior bone stop, which is necessary to resist the deceleration forces of the femur during dynamic loading.
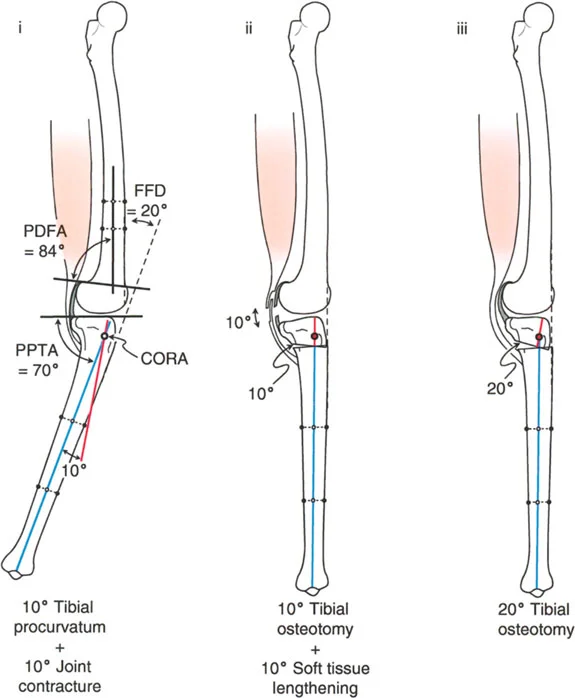
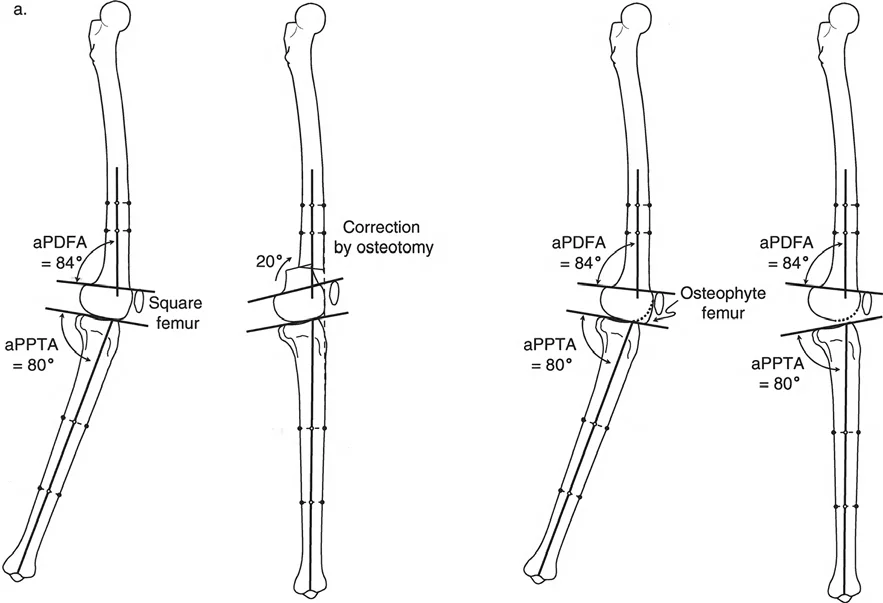
If the radiographic analysis reveals that neither tibial nor femoral procurvatum is present, the lack of extension is typically driven by intra-articular pathology, specifically anterior osteophytes or severe soft tissue joint contracture.
- Anterior Osteophyte Impingement: Large medial and anterior osteophytes act as mechanical blocks. The medial osteophyte is often associated with locking of the knee, while the anterior osteophyte limits full terminal extension. These impinging osteophytes must be meticulously resected from the femur or the tibia using either open arthrotomy or arthroscopic techniques. However, relying on resection of the osteophytes alone is historically unreliable for restoring full extension.
- Joint Contracture Management: If a soft tissue joint contracture is the primary culprit, posterior soft tissue releases or gradual distraction techniques can be employed. Alternatively, an extension osteotomy of the distal femur can be performed to functionally bypass the contracture.
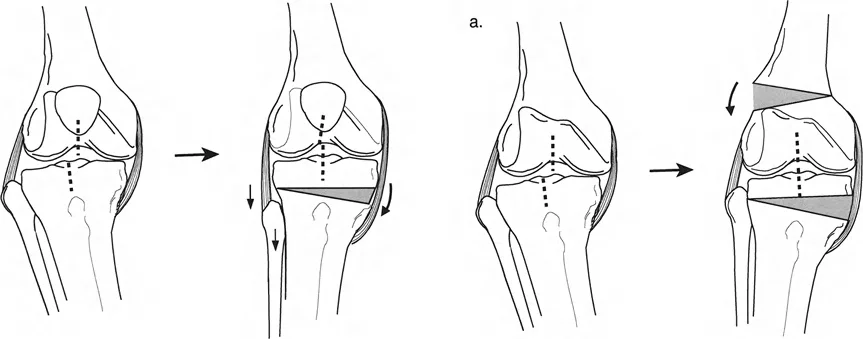
When treating varus associated with a procurvatum deformity, the choice between opening and closing wedge osteotomies dictates the osteotomy level:
* Opening Wedge Osteotomy: May be performed either proximal or distal to the tibial tuberosity, as it does not significantly alter the absolute level of the patellar tendon insertion relative to the joint line.
* Closing Wedge Osteotomy: A closing wedge proximal to the tuberosity moves the insertion closer to the joint line (patella baja). Therefore, closing wedge osteotomies for this indication are preferable distal to the tuberosity to avoid narrowing this critical distance.
Managing Medial Compartment Osteoarthritis with Coronal Plane Instability
Chronic varus malalignment often leads to adaptive changes in the soft tissue envelope of the knee. Over time, the lateral structures stretch, and the medial structures contract. In advanced cases, this can lead to lateral subluxation of the tibia relative to the femur.
Lateral Subluxation and Ligamentous Retensioning
Lateral subluxation, particularly in the absence of severe bone loss or depression of the medial tibial plateau, represents a state of dynamic instability. The Joint Line Convergence Angle will be significantly elevated on weight-bearing films.


To treat this, the surgeon cannot rely on bony realignment alone. The subluxation must be addressed by retensioning the medial collateral ligament and the lateral collateral ligament in conjunction with the realignment osteotomy.
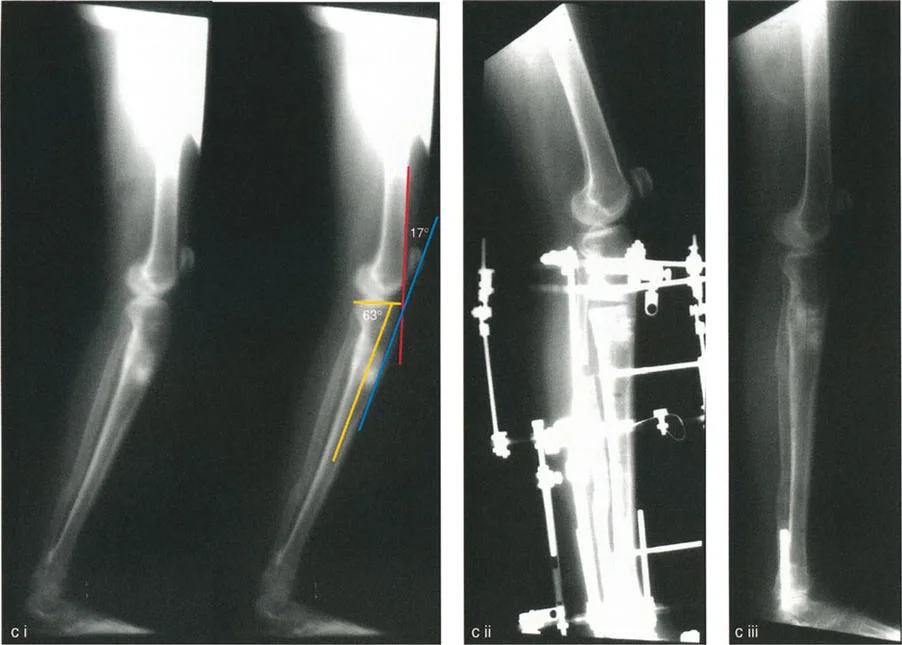
During a valgus-producing high tibial osteotomy, the mechanical axis is shifted laterally. By carefully managing the osteotomy gap and utilizing specialized fixation techniques, the surgeon can effectively tension the lateral collateral ligament. If there is no significant plateau depression, restoring the mechanical axis and correcting the soft tissue tension will recenter the joint and eliminate the lateral subluxation.
Advanced Surgical Execution and Osteotomy Rules
The physical execution of the osteotomy requires strict adherence to the preoperative plan and an understanding of how different bone cuts affect three-dimensional space.
Opening Wedge versus Closing Wedge Techniques
The decision between an opening wedge and a closing wedge osteotomy depends on the patient's specific anatomy, the required magnitude of correction, and the desired effect on leg length.
| Osteotomy Characteristic | Opening Wedge | Closing Wedge |
|---|---|---|
| Leg Length Effect | Increases leg length | Decreases leg length |
| Patellar Height Effect | Lowers patella (if distal to tuberosity) | Raises patella (if proximal to tuberosity) |
| Bone Graft Requirement | Often required for large gaps | Not required |
| Early Weight Bearing | Delayed | Generally permitted earlier |
| Fibular Osteotomy | Not always required | Mandatory |

Executing the L Cut Osteotomy
When performing the L-shaped osteotomy for combined varus and rotational deformities, the vertical cut is made posterior to the tibial tuberosity, exiting proximally into the joint or just distal to the joint line depending on the specific variation. The horizontal cut is made in the metaphyseal bone.
This design inherently provides tremendous rotational stability once the desired correction is achieved. It maximizes the surface area for rapid bone healing while allowing the tuberosity to remain attached to the proximal or distal segment, depending on the desired effect on the patellofemoral mechanism.
Fixation Strategies
Rigid internal or external fixation is mandatory to maintain the correction and allow for early rehabilitation.
- Internal Fixation: Locking plate technology has revolutionized high tibial osteotomies. TomoFix or similar rigid locking plates provide sufficient stability to maintain opening wedge corrections without the absolute need for structural bone graft in gaps less than 10-12mm.
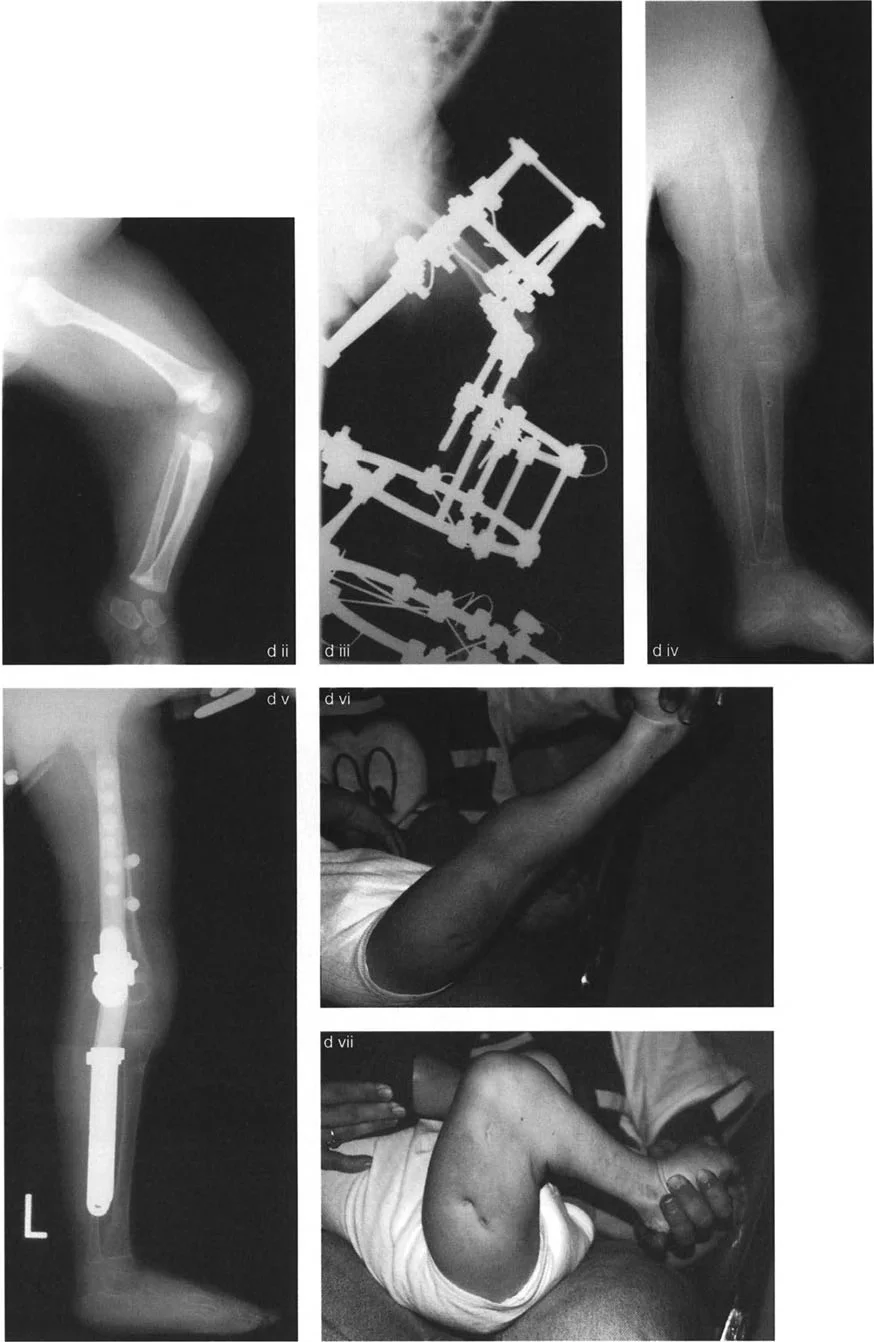
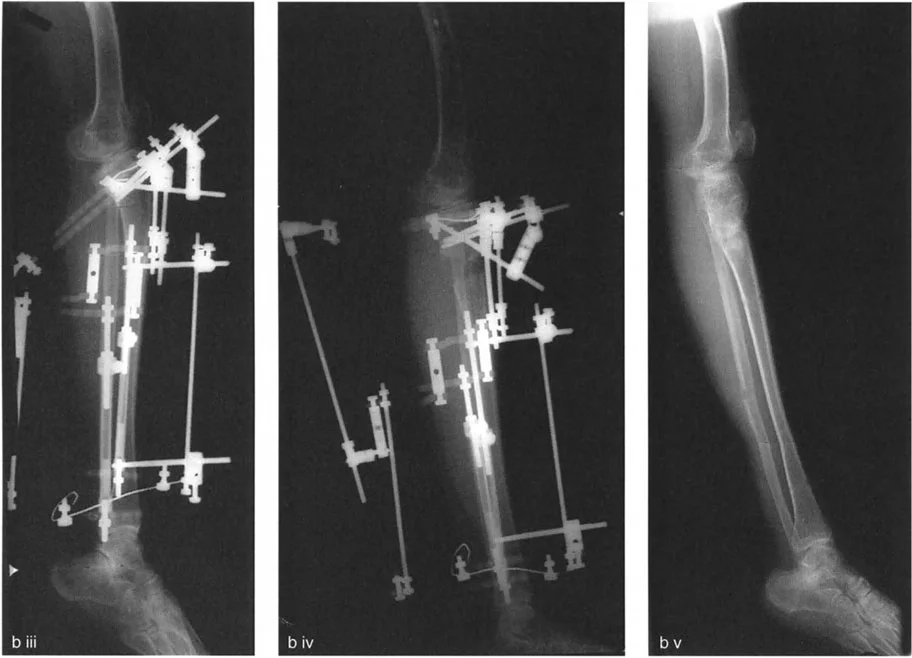
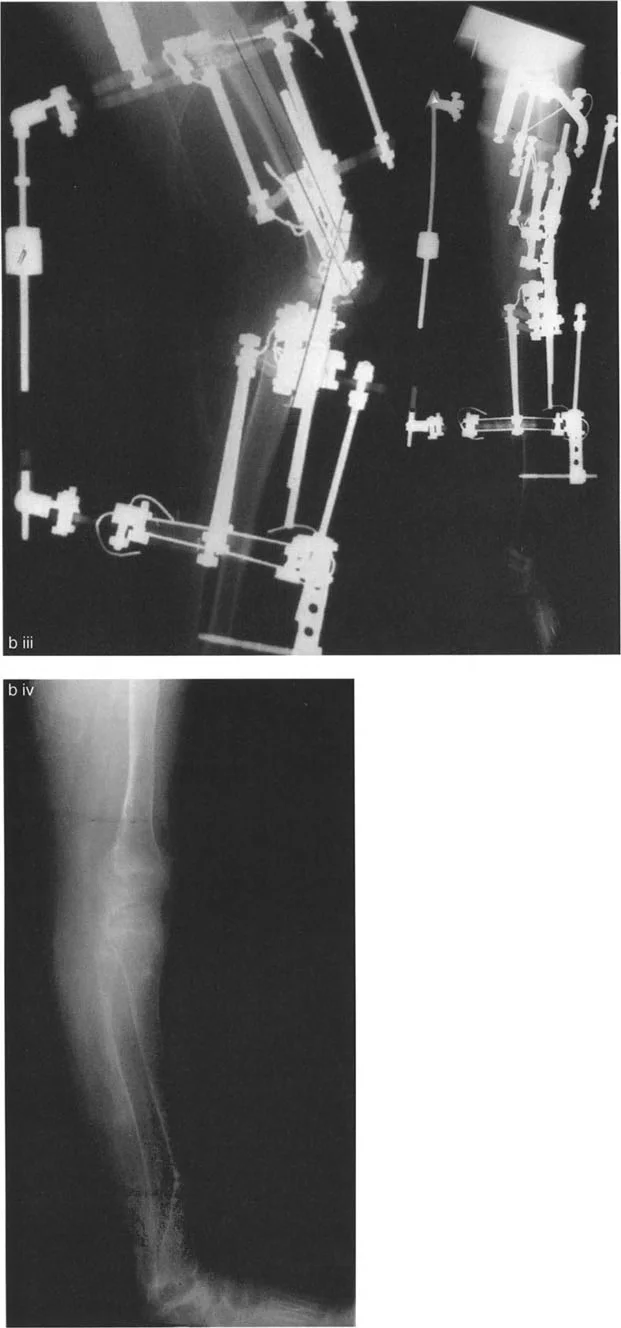
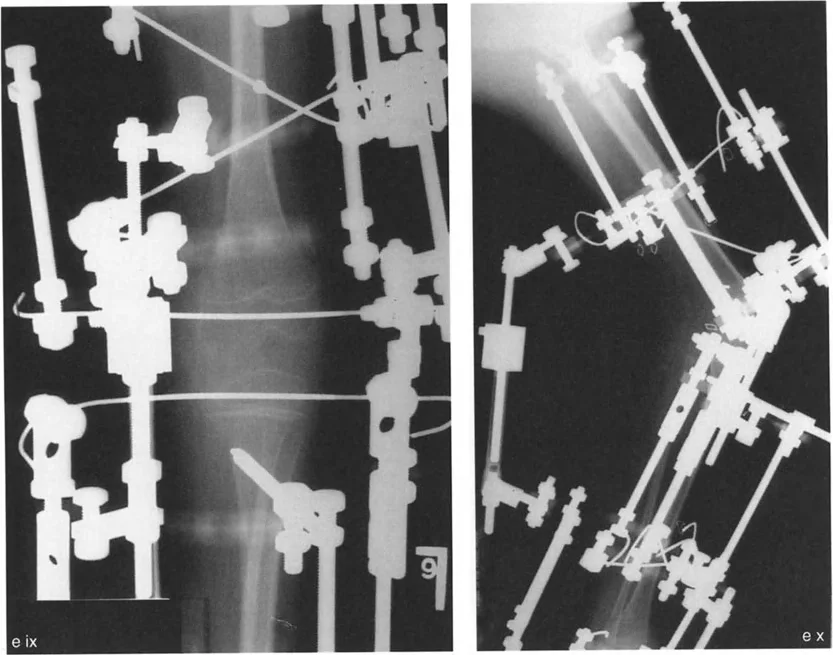
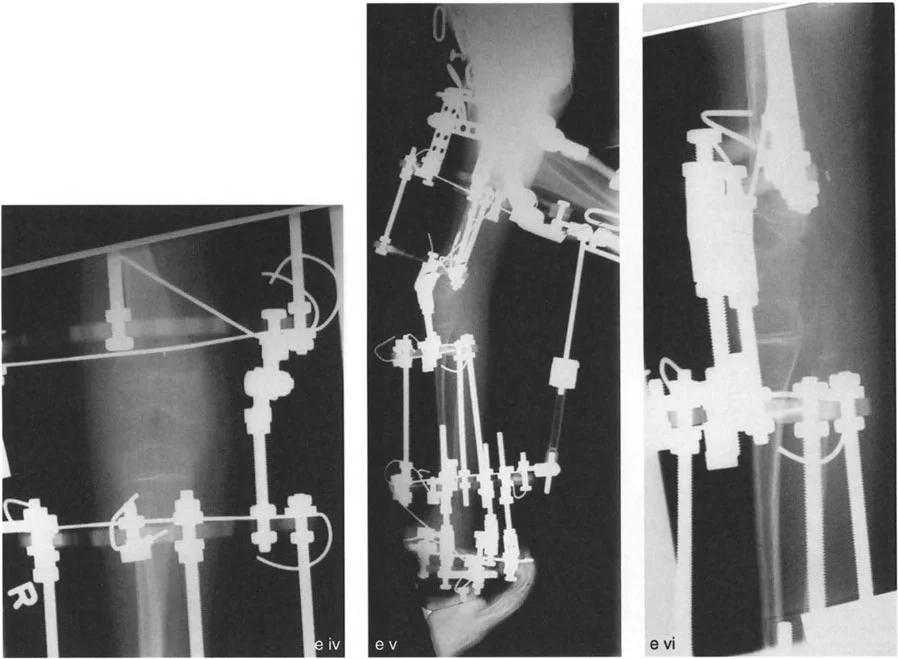
- External Fixation: Circular spatial frames (such as the Taylor Spatial Frame) are incredibly powerful tools for complex, multi-planar deformities. They allow for gradual correction of varus, recurvatum, and torsion simultaneously, utilizing the Center of Rotation of Angulation principles via a software-driven virtual hinge.
Postoperative Care and Rehabilitation Protocols
The success of a realignment osteotomy is heavily dependent on the postoperative rehabilitation phase. The goals are to protect the osteotomy site, restore range of motion, and rebuild muscular strength.
Early Postoperative Phase (Weeks 0-6)
- Weight Bearing: For opening wedge osteotomies with internal fixation, patients are typically restricted to toe-touch or partial weight-bearing for the first 4 to 6 weeks to prevent hardware failure or loss of correction. Closing wedge osteotomies may allow for earlier weight-bearing depending on bone quality and fixation rigidity.
- Range of Motion: Early, aggressive range of motion is critical, particularly to prevent the recurrence of fixed flexion deformities. Continuous Passive Motion machines or dedicated physical therapy should begin immediately postoperatively. Focus is placed on achieving full terminal extension.
Intermediate to Late Phase (Weeks 6-12 and Beyond)
- Radiographic Assessment: At 6 weeks, anteroposterior and lateral radiographs are obtained to assess callus formation and healing at the osteotomy site.
- Progression of Weight Bearing: Once radiographic healing is evident, patients are progressively transitioned to full weight-bearing.
- Strengthening: Rehabilitation shifts focus to quadriceps and hamstring strengthening. The altered mechanical axis will change the resting tension of these muscle groups, requiring neuromuscular re-education.
By rigorously applying Paley's principles of deformity correction, orthopedic surgeons can reliably manage the complex biomechanical environment of mono-compartment knee osteoarthritis. Through precise preoperative planning, accurate identification of the Center of Rotation of Angulation, and flawless surgical execution of multi-planar corrections, joint preservation becomes a highly successful and durable intervention.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like