Optimizing Knee Osteotomy: Realignment for Mono-Compartment OA with Paley's Principles
Key Takeaway
Knee realignment osteotomy for mono-compartment osteoarthritis preserves the native joint and delays TKR. It optimizes biomechanics by shifting load from diseased cartilage. Dr. Paley's principles, using CORA and mechanical axis deviation, guide precise surgical planning for optimal deformity correction.
Realignment for Mono Compartment Osteoarthritis of the Knee
Osteotomy for mono-compartment osteoarthritis of the knee represents one of the most common and technically demanding indications for deformity correction surgery. Because arthrosis is already present, the primary goal of surgical intervention is to preserve the native knee joint, optimize biomechanics, and delay the need for a Total Knee Replacement (TKR) for as long as possible.
Although many patients who undergo a well-executed High Tibial Osteotomy (HTO) or Distal Femoral Osteotomy (DFO) may never require arthroplasty, the realignment procedure must be meticulously planned and performed with the assumption that each patient must remain an optimal TKR candidate in the future. This requires strict adherence to the principles of deformity correction, ensuring that joint line obliquity and mechanical axis translation do not compromise future implant positioning.
The knee joint consists of three distinct compartments: the medial, the lateral, and the patellofemoral compartments. While arthritis may affect one or more of these regions, the medial compartment is overwhelmingly the most common site of isolated degenerative joint disease. This comprehensive guide focuses predominantly on Medial Compartment Osteoarthritis (MCOA) and the application of Dr. Dror Paley's principles of deformity correction to achieve optimal surgical outcomes.
Biomechanics of Knee Load Distribution
Understanding the normal and pathologic load distribution across the tibial plateau is critical for planning any realignment surgery. The goal of an osteotomy is not merely to make the leg look straight, but to mechanically unload the diseased cartilage and shift the weight-bearing forces to the healthier compartment.
In a normally aligned lower extremity, the mechanical axis passes slightly medial to the center of the knee joint. This results in a physiologic mechanical varus of approximately 1 to 2 degrees. Because of this slight medial deviation, the medial compartment bears the majority of the load during the single-leg stance phase of the gait cycle.
Load Distribution Dynamics
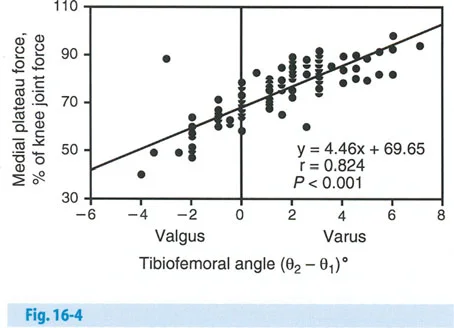
The relationship between the mechanical tibiofemoral angle and the percentage of load borne by the medial plateau is non-linear and highly sensitive to minor angular changes.
- Normal Alignment When the mechanical axis passes through the exact center of the knee, the medial compartment bears approximately 67 percent of the load. In a physiologic knee with 2 degrees of mechanical varus, the medial compartment takes roughly 70 to 75 percent of the load.
- Pathologic Varus The load shifts dramatically with increasing varus deformity. With only 6 degrees of mechanical tibiofemoral varus, the medial plateau force spikes to 95 percent. This exponential increase in load rapidly accelerates cartilage wear and subchondral bone failure in MCOA.
- Therapeutic Valgus To unload the medial compartment, the mechanical axis must be shifted laterally. When the mechanical axis is moved into 4 degrees of valgus, the load is distributed evenly, with 50 percent medial and 50 percent lateral. When the mechanical axis is moved into 6 degrees of valgus, the load shifts to 40 percent medial and 60 percent lateral.
Deformity Analysis in Medial Compartment Osteoarthritis
A successful realignment surgery requires a comprehensive understanding of where the deformity originates. Deformities associated with MCOA are rarely isolated to a single plane or a single anatomical structure. They must be systematically subdivided into bone deformities and joint or soft tissue deformities.
Bone Deformities
Structural bone deformities can occur in the femur, the tibia, or both, and may exist in multiple planes.
- Femur Deformities may present as varus or valgus in the coronal plane, recurvatum or procurvatum in the sagittal plane, and with or without torsional malalignment in the axial plane.
- Tibia The most common presentation is proximal tibial varus. However, this is frequently accompanied by torsion and sagittal plane deformities such as procurvatum or recurvatum. Failure to address the sagittal and axial planes during a coronal plane correction is a common pitfall.
Joint and Soft Tissue Deformities
Soft tissue laxity and intra-articular bone loss contribute significantly to the overall mechanical axis deviation. These must be quantified preoperatively using stress radiographs and careful clinical examination.
- Ligamentous Laxity Lateral Collateral Ligament (LCL) laxity is common in chronic varus knees due to lateral soft tissue stretching. Medial Collateral Ligament (MCL) contracture or pseudo-laxity may also be present.
- Intra Articular Bone Loss Medial tibial plateau depression or severe cartilage loss creates a "joint space" deformity.
- Dynamic Instability Lateral subluxation of the tibia on the femur, patellar maltracking, and fixed flexion contractures frequently accompany advanced MCOA.
Foundational Paley Principles for Knee Realignment
To properly plan and execute an osteotomy, orthopedic surgeons must utilize the standardized nomenclature and geometric principles popularized by Dr. Dror Paley. These principles allow for the precise calculation of the Center of Rotation of Angulation (CORA) and dictate the surgical rules for correction.
Mechanical Axis Deviation
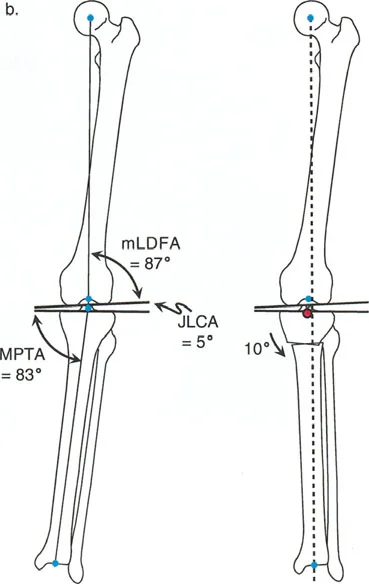
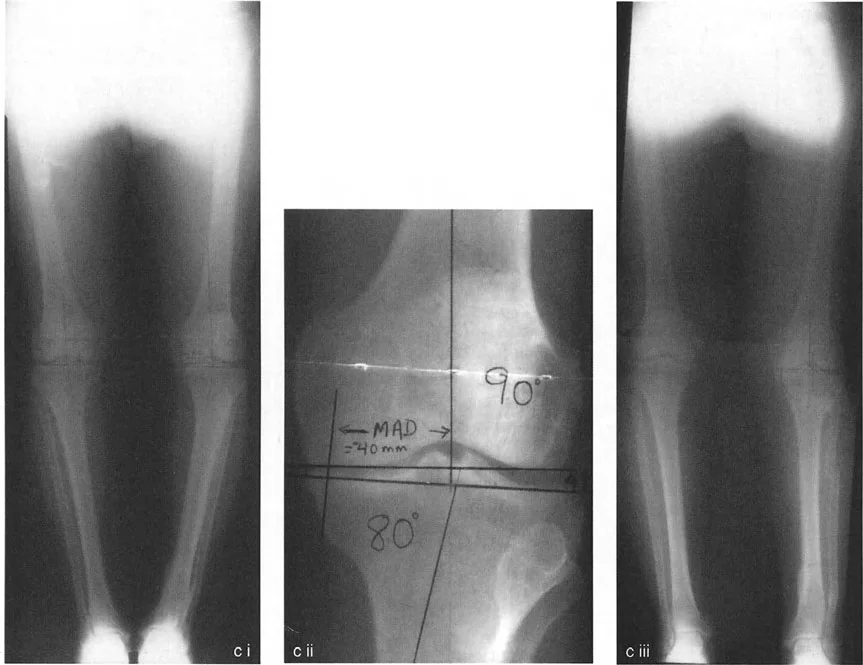
The Mechanical Axis Deviation (MAD) is the perpendicular distance from the mechanical axis line of the lower extremity (drawn from the center of the femoral head to the center of the ankle mortise) to the center of the knee joint. In a normal knee, the MAD is slightly medial (0 to 8 mm). In MCOA, the MAD is significantly increased medially.
Joint Orientation Angles
Accurate deformity analysis relies on measuring the angles between the mechanical axes of the bones and their respective joint lines.
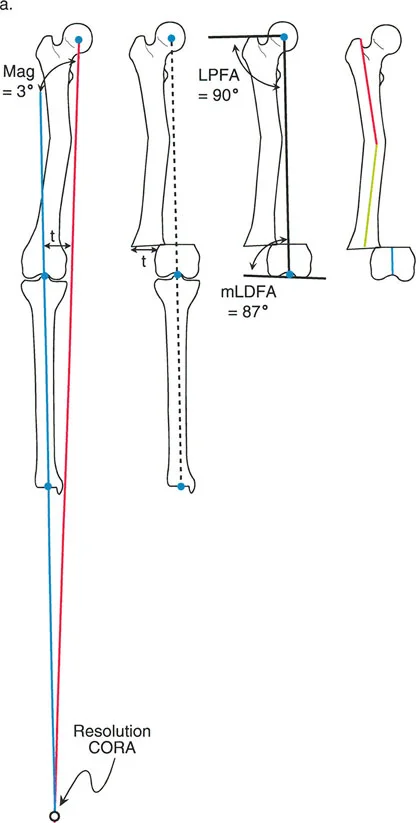
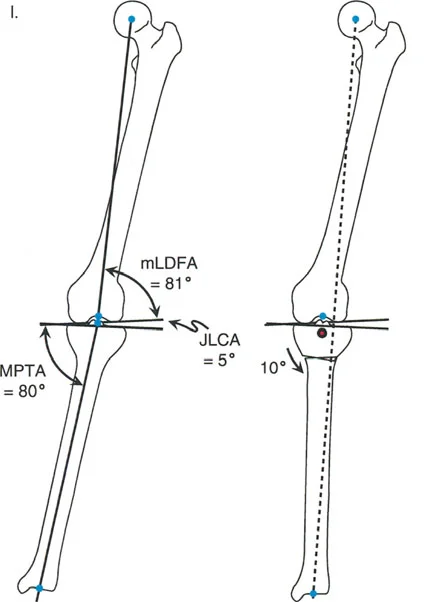
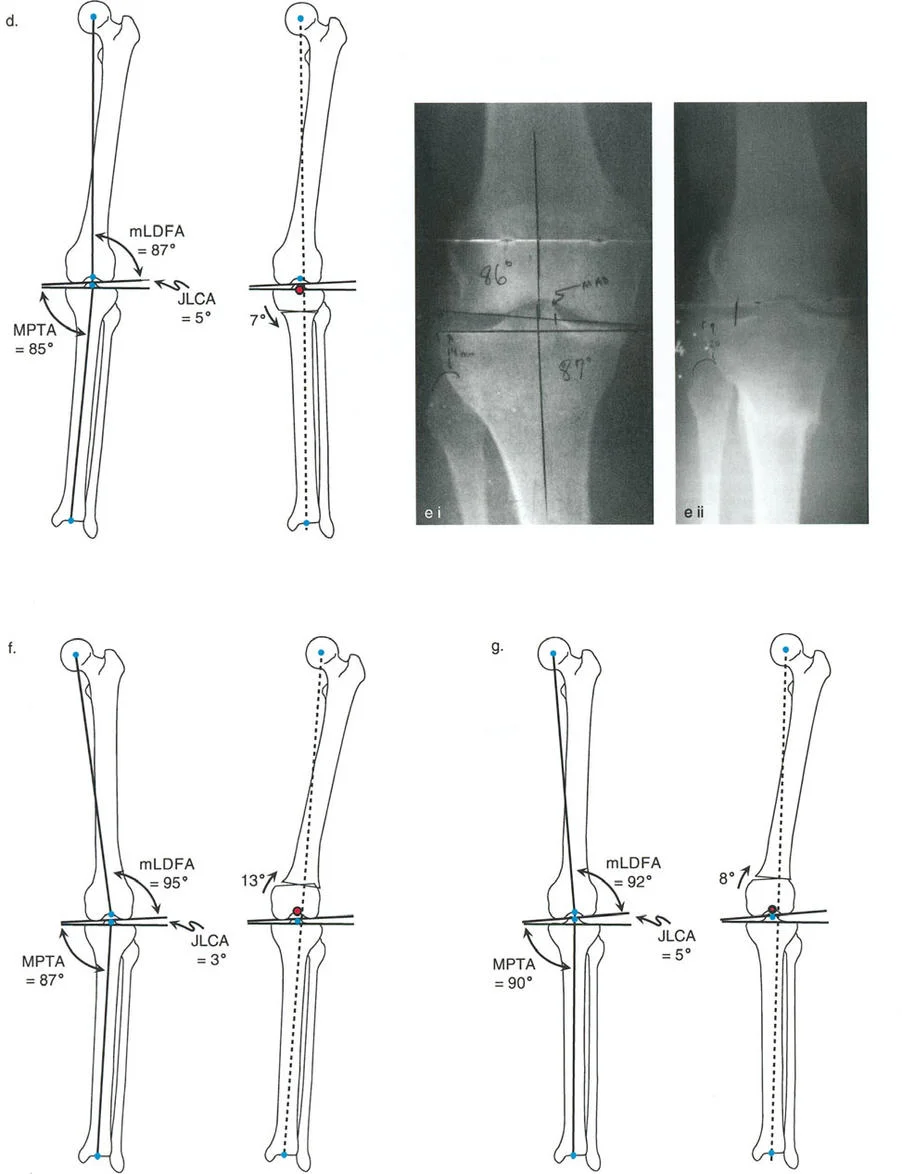
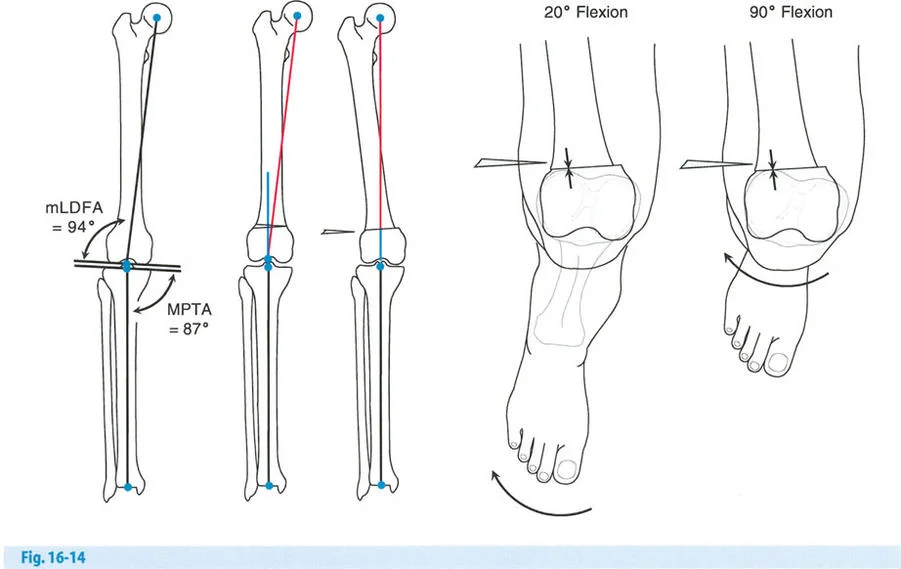
- Mechanical Lateral Distal Femoral Angle The mLDFA is the lateral angle formed by the mechanical axis of the femur and the distal femoral joint line. The normal range is 87 to 89 degrees.
- Mechanical Proximal Tibial Angle The MPTA is the medial angle formed by the mechanical axis of the tibia and the proximal tibial joint line. The normal range is 87 to 89 degrees.
- Joint Line Convergence Angle The JLCA is the angle formed between the distal femoral joint line and the proximal tibial joint line. In a normal knee, this angle is 0 to 2 degrees. In a varus arthritic knee, the JLCA increases due to medial cartilage loss and lateral ligamentous laxity.
Center of Rotation of Angulation
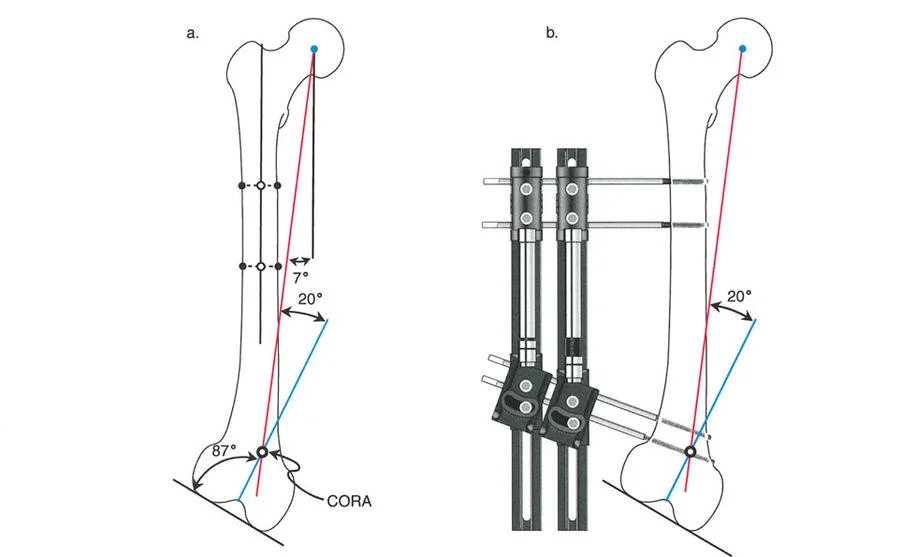
The CORA is the intersection of the proximal and distal mechanical axis lines of a deformed bone. Identifying the CORA is the most critical step in preoperative planning, as its location dictates where the osteotomy should be performed and where the hinge (Axis of Correction of Angulation, or ACA) should be placed to avoid unwanted translation.
Historical Evolution of High Tibial Osteotomy
The surgical techniques for treating MCOA have evolved significantly over the past several decades. Analyzing these historical procedures through the lens of Paley's principles reveals why certain techniques succeeded and why others led to high complication rates or compromised future arthroplasty.
The Jackson and Waugh Technique
The concept of High Tibial Osteotomy to treat MCOA is largely credited to Jackson and Waugh (1961). They performed an osteotomy distal to the tibial tuberosity in the diaphyseal bone. They utilized both closing wedge and concave distal dome osteotomies.
From a modern deformity perspective, the Jackson and Waugh osteotomy level was fairly distal to the CORA. Because the osteotomy and the ACA were separated from the true CORA, this technique invariably led to a translational deformity of the mechanical axis, creating a zigzag effect in the bone.
The Coventry Modification
Difficulties with bone healing in the dense diaphyseal bone of the subtuberosity region led Coventry (1965) to modify the procedure. Coventry reported on a closing wedge osteotomy performed proximal to the tuberosity, directly through the highly vascularized cancellous bone of the metaphysis.
This proximal location brought the osteotomy much closer to the anatomical CORA. By placing both the osteotomy and the ACA near the CORA, Coventry's technique provided a more pure angular correction with better healing rates, though it required fibular osteotomy or proximal tibiofibular joint disruption.
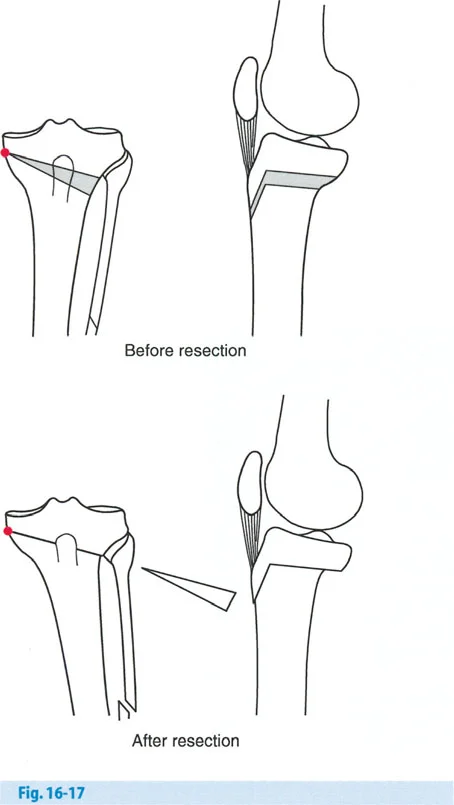
The Maquet Barrel Vault Osteotomy
Maquet (1976, 1980) introduced a concave distal dome osteotomy, often referred to as the barrel vault osteotomy. This procedure was designed to take advantage of rapid metaphyseal bone healing above the tuberosity while adding a high degree of adjustability in the coronal and sagittal planes.
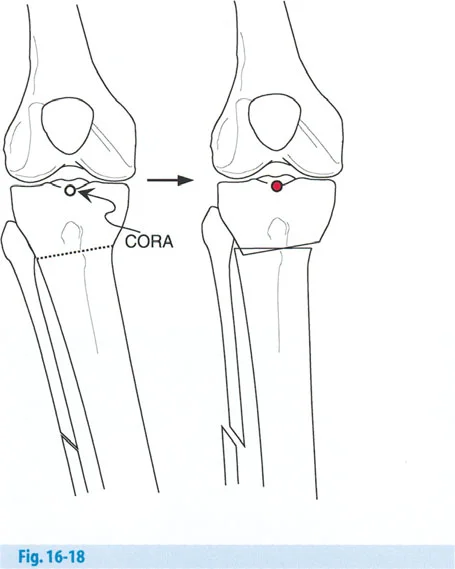
However, the Maquet dome osteotomy was made proximal to the tuberosity with the concavity facing distally. Geometrically, the center of rotation of this dome (the ACA) is located far distal to the tuberosity. Because the ACA was positioned far from the CORA, the Maquet osteotomy induced a marked translational deformity, violating Paley's first osteotomy rule.
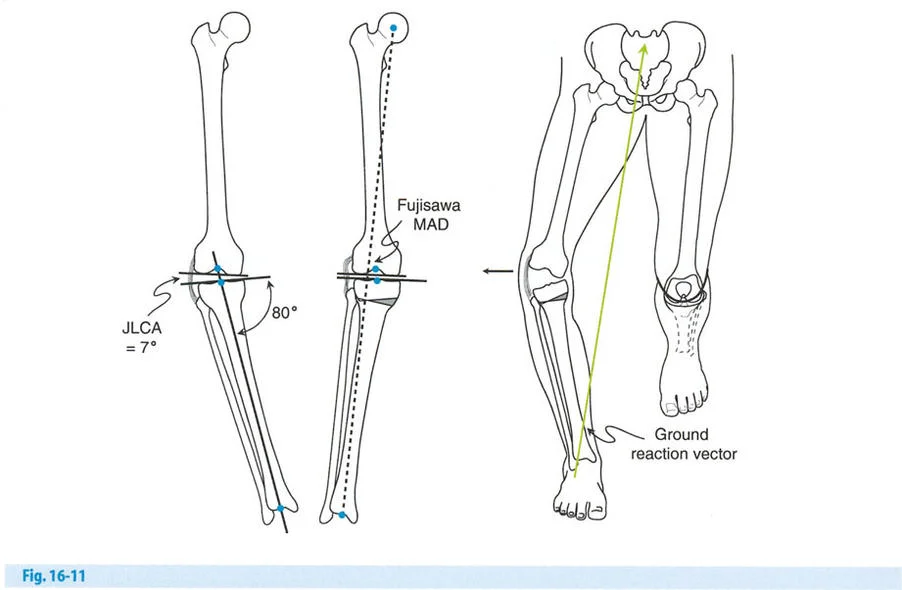
The Fujisawa Point and Target Mechanical Axis Deviation
The common goal for all HTO procedures is to shift the mechanical axis from the overloaded medial compartment to the relatively preserved lateral compartment. While it is biomechanically impractical to completely unload the medial compartment, the primary objective is to reduce the load to a level that alleviates pain and halts cartilage degradation.
Most historical and contemporary authors agree that for the successful treatment of MCOA, the mechanical alignment of the lower limb should be moved into 2 to 6 degrees of mechanical valgus. Hernigou et al. (1987) demonstrated that optimal clinical outcomes were achieved with 3 to 6 degrees of mechanical valgus, and that results rapidly deteriorated when the valgus overcorrection exceeded 6 degrees.
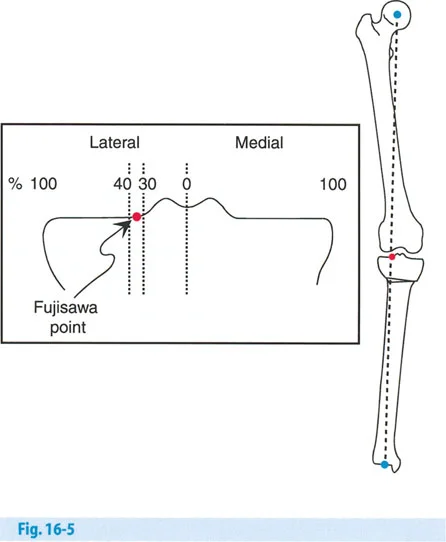
Defining the Fujisawa Point
Fujisawa et al. (1979) provided a more precise anatomical target for this correction. They divided the medial and lateral tibial plateaus by the percentage of distance from the center of the knee. The extreme medial and lateral edges of the plateaus were considered to be 100 percent, while the exact center of the knee (the tibial spines) was considered to be 0 percent.
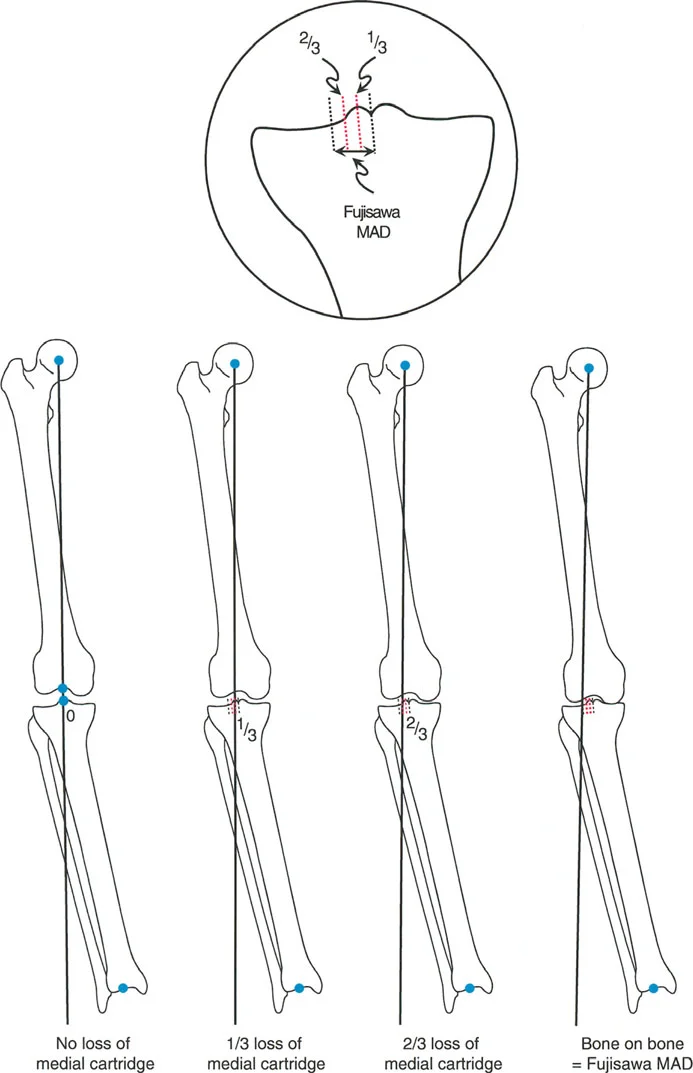
Fujisawa determined that the best long-term results from HTO were obtained when the postoperative mechanical axis line of the limb passed through the 30 percent to 40 percent region of the lateral plateau. In modern deformity planning, we refer to this specific coordinate as the Fujisawa Point or the Fujisawa MAD.
The Jakob and Murphy Cartilage Loss Rules
While the Fujisawa point provides an excellent baseline, Jakob and Murphy (1992) recognized that the degree of overcorrection should be titrated based on the severity of medial compartment cartilage loss. They developed a proportional rule for targeting the postoperative MAD.
- Normal Medial Joint Space If the medial compartment joint space is entirely normal (e.g., treating an isolated varus deformity without arthrosis), the correction goal is a MAD of 0 (the mechanical axis passes directly through the center of the knee).
- One Third Cartilage Loss If the medial compartment joint space is decreased by one third, the correction goal is a MAD equal to one third of the distance to the Fujisawa point.
- Two Thirds Cartilage Loss If the medial compartment joint space is decreased by two thirds, the correction goal is a MAD equal to two thirds of the distance to the Fujisawa point.
- Bone on Bone Arthrosis If the medial compartment joint space is completely obliterated (bone on bone), the correction goal is a MAD of three thirds (100 percent) of the Fujisawa point, placing the axis squarely at the 30 to 40 percent lateral mark.
Paley Osteotomy Rules Applied to the Proximal Tibia
When planning the surgical execution of an HTO, the surgeon must decide between an opening wedge, a closing wedge, or a dome osteotomy. The choice of technique dictates the location of the ACA and the resulting translation of the bone segments. These decisions are governed by Paley's three osteotomy rules.
Rule One Pure Angulation
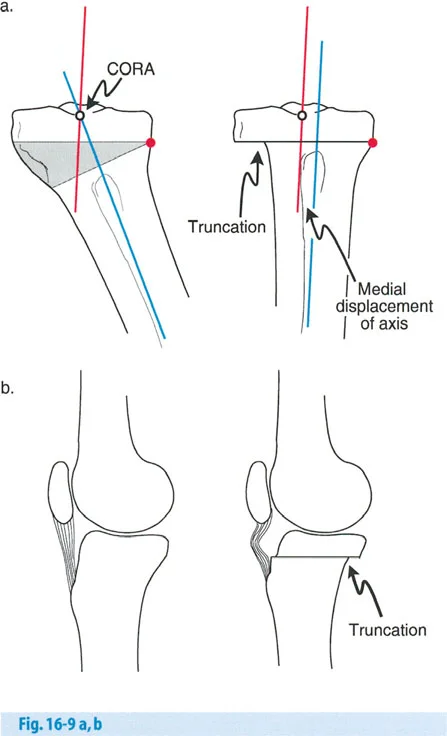
If the osteotomy and the ACA are both located at the CORA, the result is pure angulation without any translation. In a proximal tibial varus deformity, the CORA is typically located at the joint line. Because it is impossible to cut through the joint line, Rule One is rarely achieved in standard HTO.
Rule Two Angulation with Intentional Translation
If the ACA is placed at the CORA, but the osteotomy is performed at a different level (e.g., in the proximal metaphysis), the mechanical axis will be fully realigned. However, this will result in a planned, predictable translation of the bone segments at the osteotomy site. This is the most common scenario for a well-planned opening or closing wedge HTO. The translation is acceptable and often necessary to restore the overall mechanical axis.
Rule Three Unwanted Mechanical Axis Shift
If the osteotomy and the ACA are both located at a level different from the CORA (as seen in the Maquet dome osteotomy), the mechanical axis lines will not intersect at the CORA. Instead, they will shift parallel to one another, resulting in a translational deformity of the entire limb. This violates the principles of proper realignment and can lead to abnormal joint shear forces.
Step by Step Preoperative Planning for Knee Realignment
Surgical success in deformity correction is achieved in the planning room, not just in the operating theater. A rigorous, step-by-step approach to preoperative planning ensures precision and minimizes intraoperative surprises.
Step One Image Acquisition
Standardized imaging is non-negotiable. Obtain full-length, weight-bearing, standing anteroposterior (AP) radiographs of both lower extremities on a single cassette. The patellae must be facing strictly forward to control for rotation. Additional views should include weight-bearing PA flexion (Rosenberg) views, lateral views, and Merchant views of the patellofemoral joint.
Step Two Joint Angle Measurement
Draw the mechanical axes of the femur and tibia. Measure the mLDFA, MPTA, and JLCA. Compare these values to population norms and to the contralateral limb. This determines whether the varus deformity is driven by the femur, the tibia, or intra-articular soft tissue wear.
Step Three Determining the Target MAD
Based on the degree of medial cartilage wear (utilizing the Jakob and Murphy criteria), mark the target postoperative mechanical axis on the radiograph. Draw a line from the center of the femoral head through the desired Fujisawa point on the lateral tibial plateau, extending it down to the level of the ankle.
Step Four Calculating the Correction Angle
Using the Miniaci method, place a hinge point (the ACA) on the lateral cortex of the proximal tibia (for an opening wedge HTO). Draw a line from the ACA to the center of the ankle mortise. Draw a second line from the ACA to the point where the new target mechanical axis intersects the ankle joint line. The angle between these two lines is the exact degree of angular correction required.
Preserving the Knee for Future Total Knee Replacement
A paramount consideration during HTO is the preservation of optimal anatomy for a future Total Knee Replacement. If an osteotomy creates severe anatomical distortion, a subsequent TKR transitions from a primary procedure to a complex, highly morbid revision-style surgery.
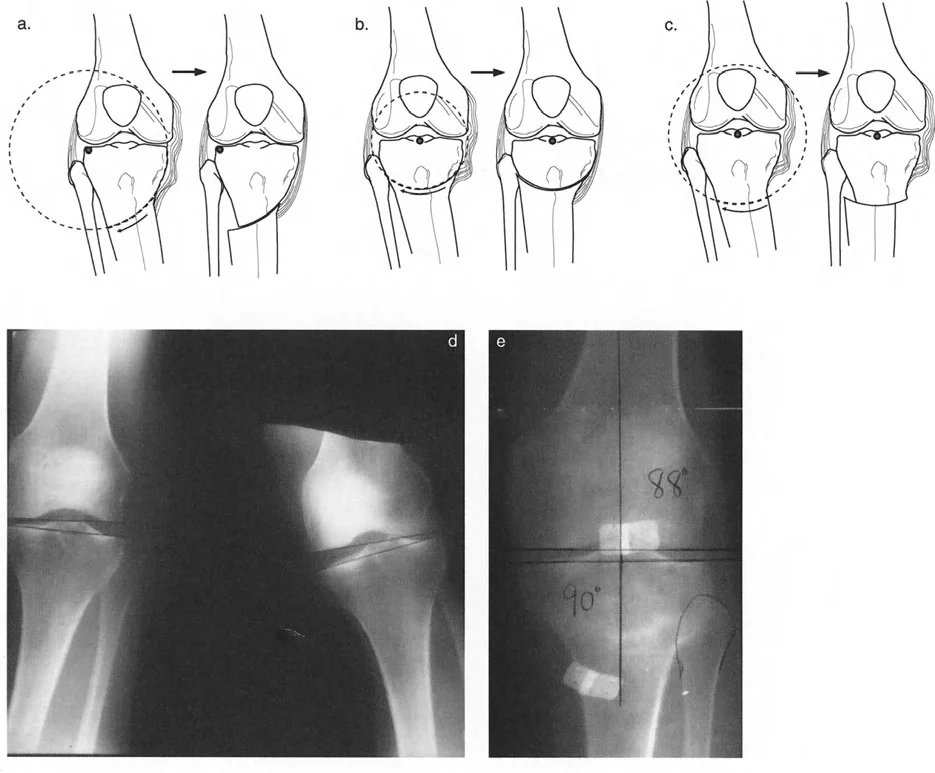
Managing Joint Line Obliquity
The goal of an HTO is to correct the MAD, but this must not come at the expense of severe joint line obliquity. If a massive proximal tibial varus deformity is corrected entirely through the tibia, it may result in an MPTA that exceeds 95 degrees. A severely valgus proximal tibial joint line creates sheer forces that accelerate cartilage wear and makes balancing a future TKR exceedingly difficult.
If the required correction would push the MPTA beyond 90 to 92 degrees, the surgeon must consider a double-level osteotomy (performing both a distal femoral and a proximal tibial osteotomy) to share the correction and maintain a horizontal joint line.
Controlling the Sagittal Plane
Changes in the coronal plane frequently induce unintended changes in the sagittal plane. The proximal tibia has a natural posterior slope of approximately 7 to 10 degrees.
- Opening Wedge HTO Because the anterior cortex of the tibia is curved and the posterior cortex is flat, an anteromedial opening wedge naturally increases the posterior tibial slope if the gap is opened symmetrically. To maintain the native slope, the anterior gap must be approximately half the size of the posterior gap. Increased posterior slope alters knee kinematics, increasing tension on the Anterior Cruciate Ligament (ACL).
- Closing Wedge HTO Conversely, a lateral closing wedge HTO tends to decrease the posterior tibial slope. This can be beneficial in ACL-deficient knees but detrimental in Posterior Cruciate Ligament (PCL) deficient knees.
Minimizing Metaphyseal Translation
Excessive lateral translation of the distal tibial segment (often seen with large closing wedge osteotomies or Rule Three violations) creates a metaphyseal offset. When a future TKR is performed, the tibial baseplate stem will impinge on the lateral cortex of the tibial diaphysis, requiring offset stems or complex bone grafting. Proper ACA placement minimizes this translation.
Surgical Pearls and High Yield Takeaways
For the orthopedic surgeon in training, mastering the nuances of knee realignment requires synthesizing biomechanics, geometry, and surgical technique.
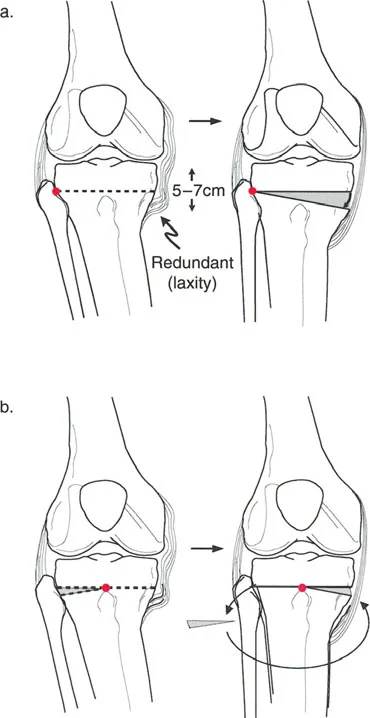
- Assess the Soft Tissues Always measure the JLCA. If the JLCA is greater than 2 degrees, a portion of the varus deformity is dynamic (soft tissue laxity or cartilage loss). Correcting the entire deformity through the bone will result in severe overcorrection once the limb is loaded and the lateral soft tissues tighten.
- Respect the Hinge In an opening wedge HTO, the lateral cortex acts as the hinge. Preserving the integrity of this lateral cortical hinge is vital for rotational stability and bone healing. If the hinge fractures, rigid internal fixation (such as a locking plate) must be applied to prevent unwanted translation or collapse.
- Release the Superficial MCL To safely open a medial wedge without fracturing the lateral hinge or increasing compartment pressures, the superficial medial collateral ligament and the pes anserinus must be meticulously released or elevated off the proximal tibia.
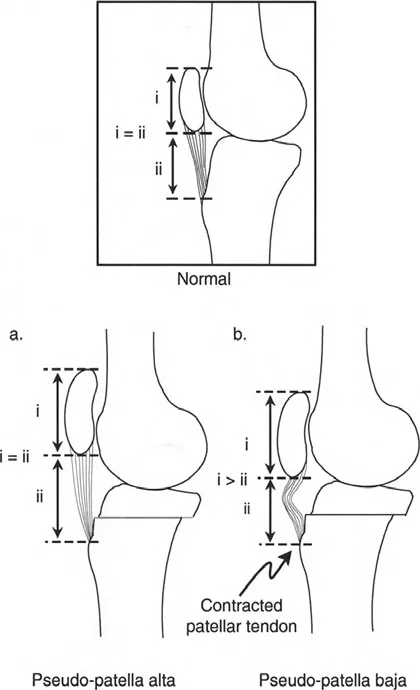
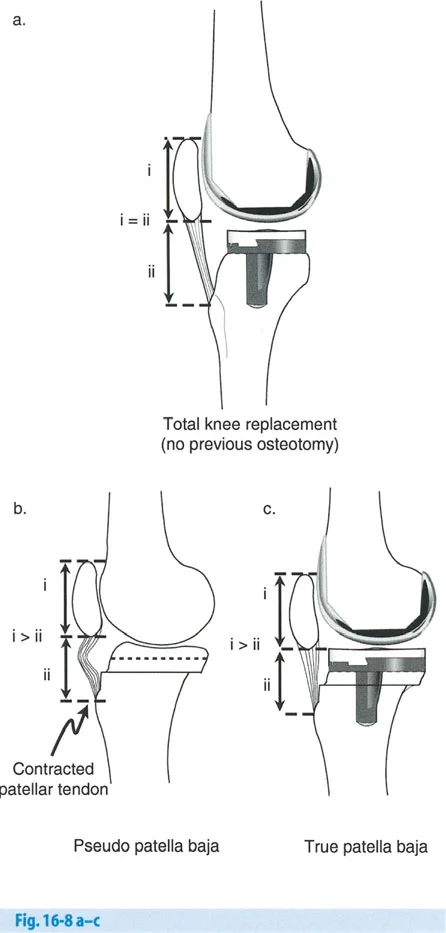
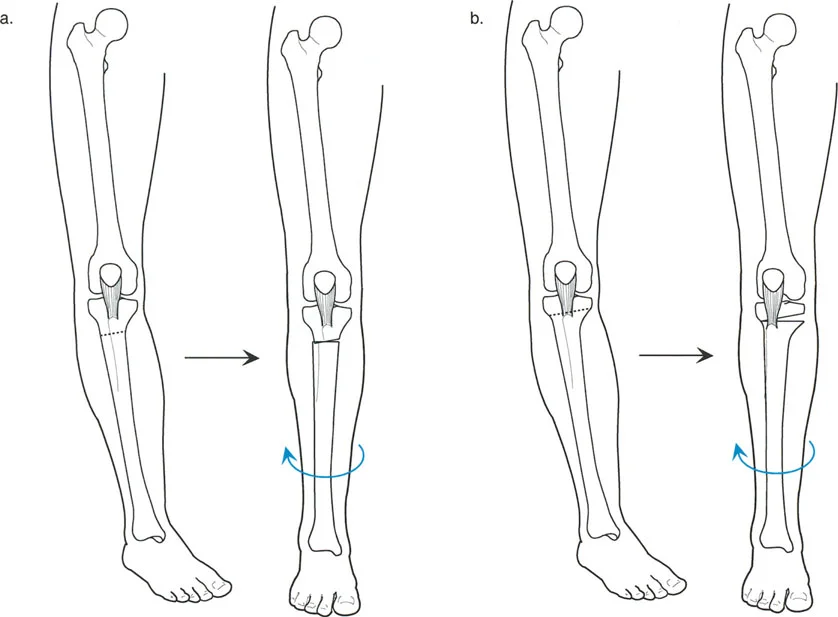
- Plan for the Patella An opening wedge HTO distal to the tibial tubercle effectively lowers the patella (patella infera), which can complicate a future TKR. If patella infera is a concern, the osteotomy can be planned bi-planar, leaving the tubercle attached to the proximal segment.
By strictly adhering to Paley's principles of deformity correction, accurately calculating the CORA and target MAD, and respecting the biomechanical limits of the knee joint, orthopedic surgeons can reliably execute realignment procedures that relieve pain, restore function, and successfully bridge the gap to future arthroplasty.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like