Unlocking Paley's Principles: A Masterclass in Lower Limb Alignment & Deformity Correction
Key Takeaway
Paley's principles define normal lower limb alignment and joint orientation, crucial for orthopedic surgeons. They involve mastering mechanical and anatomic axes, tibiofemoral angles, and specific joint orientation angles (mLDFA, MPTA, LDTA) for accurate deformity correction and successful surgical outcomes.
The Foundation of Orthopedic Mastery and Lower Limb Alignment
For orthopedic surgeons in training, mastering the principles of lower limb alignment is not merely an academic exercise—it is the absolute bedrock of successful surgical intervention. Whether you are performing a complex deformity correction using a Taylor Spatial Frame, executing a High Tibial Osteotomy for unicompartmental osteoarthritis, nailing a distal femur fracture, or templating a primary Total Knee Arthroplasty, understanding Dr. Dror Paley’s principles of normal lower limb alignment and joint orientation is non-negotiable.
A single millimeter of translation or a single degree of uncorrected angulation can alter joint reaction forces exponentially. This biomechanical shift leads to premature implant failure, adjacent joint disease, catastrophic nonunions, and poor patient outcomes. This comprehensive masterclass transforms the foundational concepts of Paley’s principles into a high-yield, clinically actionable guide. We will deconstruct the mechanical axes, anatomical axes, joint lines, the Center of Rotation of Angulation, and the precise angular measurements that define the normal human lower extremity.
Mechanical and Anatomic Axes of the Lower Extremity
Before diving into specific joint orientations and complex deformity correction, we must establish the universal language of alignment. The lower extremity is governed by two distinct types of axes that dictate weight-bearing and anatomical relationships.
The Anatomic Axis
The anatomic axis is defined as the mid-diaphyseal line of a long bone. It represents the physical center of the bone cylinder.
- Femur Anatomic Axis: The anatomic axis of the femur is curved in the sagittal plane, presenting with a natural anterior bow. However, in the frontal (coronal) plane, it is generally evaluated as a straight line bisecting the proximal and distal diaphyseal medullary canal.
- Tibia Anatomic Axis: The anatomic axis of the tibia is a straight line passing directly through the center of the tibial diaphysis in both the frontal and sagittal planes.
The Mechanical Axis
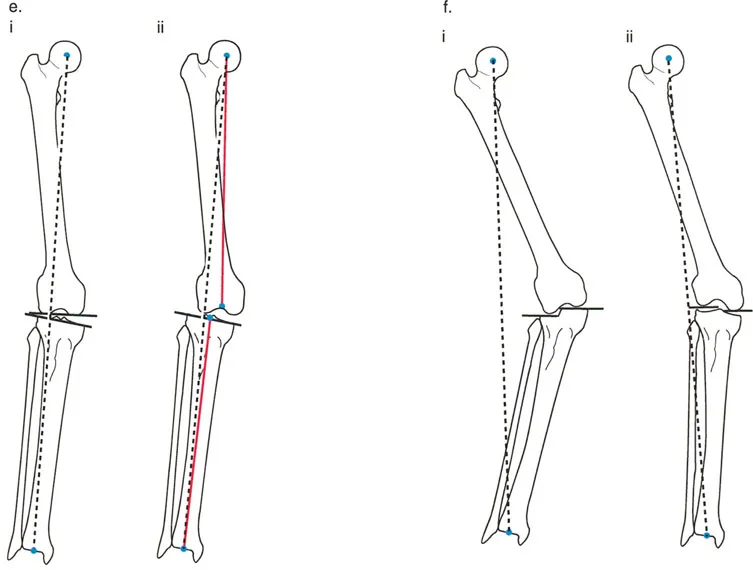
The mechanical axis represents the true line of weight-bearing and force transmission across the joints. This is the most critical axis for evaluating lower limb alignment and planning corrective osteotomies.
- Femoral Mechanical Axis: A line drawn from the exact center of the femoral head to the center of the distal femoral intercondylar notch.
- Tibial Mechanical Axis: A line drawn from the center of the proximal tibial plateau (often marked by the tibial spines) to the center of the tibial plafond at the ankle joint.
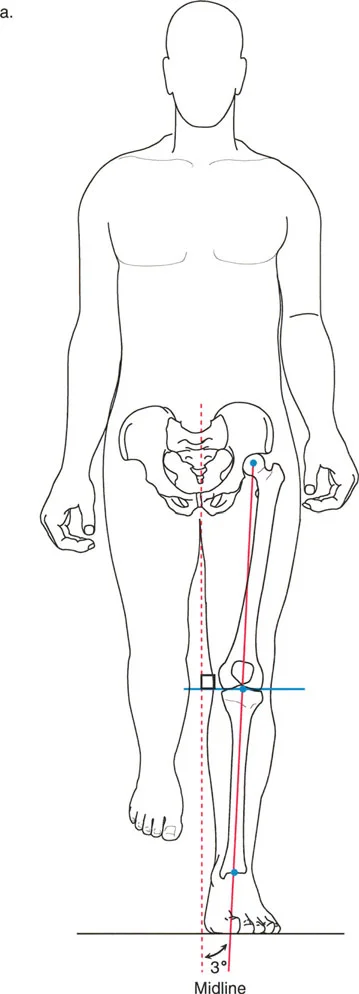
- Lower Limb Mechanical Axis: In the frontal plane, this is a continuous, straight line passing from the center of the femoral head directly to the center of the ankle plafond.
Clinical Pearl for Axes Evaluation
Always ensure radiographs are taken with the patella facing strictly forward. Rotational variations during X-ray acquisition will falsely project the mechanical and anatomic axes, leading to catastrophic errors in preoperative templating.
Calculating the Mechanical Axis Deviation
By definition, malalignment occurs when the center of the knee joint does not lie in its normal proximity to the mechanical axis of the lower limb. The distance between the mechanical axis line and the center of the knee in the frontal plane is termed the Mechanical Axis Deviation.
To accurately assess Mechanical Axis Deviation, the surgeon must obtain a long-standing, weight-bearing anteroposterior radiograph of the entire lower extremity on a single cassette.
Normal Values for Mechanical Axis Deviation
While textbook illustrations often simplify alignment by showing the mechanical axis passing perfectly through the dead-center of the knee, clinical reality dictates a slight medial offset. The normal mechanical axis actually passes immediately medial to the center of the knee joint.
- Paley et al 1994: In a retrospective study of adult knees, the normal Mechanical Axis Deviation was found to be 9.7 ± 6.8 mm medial to the center of the knee.
- Bhave et al: In a prospective study of normal lower limbs in patients older than 60 without knee pathology, the deviation was 4.1 ± 4 mm medial.
When the Mechanical Axis Deviation falls medial to the normal limits, the patient has a structural varus malalignment. When the deviation falls lateral to the center of the knee, the patient has a valgus malalignment.
Tibiofemoral Angle Analysis
The relationship between the femur and tibia can be expressed as an angle, which is a rapid way to assess overall limb alignment before breaking down individual joint orientations.
Mechanical Tibiofemoral Angle
The Mechanical Tibiofemoral Angle is the angle formed between the mechanical axis of the femur and the mechanical axis of the tibia.
* Normal Value: 1.2° to 1.3° varus.
* Interestingly, demographic studies (such as Glimet et al. on asymptomatic elderly populations) have occasionally found a mechanical tibiofemoral angle of exactly 0°. For surgical reconstruction, aiming for a neutral mechanical axis (0°) is often the accepted standard, particularly in Total Knee Arthroplasty.
Anatomic Tibiofemoral Angle
The Anatomic Tibiofemoral Angle is the angle formed between the anatomic axes of the femur and tibia. This is the angle most commonly referenced in standard clinical practice when evaluating short knee radiographs.
* Normal Value: Approximately 6° valgus. This angle is highly dependent on the patient's pelvic width and femoral length.
| Angle Type | Axis Utilized | Normal Value Range | Clinical Relevance |
|---|---|---|---|
| Mechanical Tibiofemoral | Femoral & Tibial Mechanical | 0° to 1.3° Varus | Primary target for TKA and gross deformity correction. |
| Anatomic Tibiofemoral | Femoral & Tibial Anatomic | 5° to 7° Valgus | Used for intramedullary nailing and standard knee films. |
Frontal Plane Joint Orientation Angles
Understanding the overall mechanical axis is only the first step in deformity correction. To correct a deformity, you must know exactly where the deformity lies. Is the varus coming from the femur, the tibia, or the joint space itself?
To answer this, we evaluate the joint orientation angles. By convention, Dr. Paley established a universal nomenclature: we always refer to the distal segment relative to the proximal segment, and we use specific prefixes and suffixes (m = mechanical, a = anatomic, L = lateral, M = medial, P = proximal, D = distal, F = femur, T = tibia, A = angle).
Hip Joint Orientation
The orientation of the proximal femur is critical for preoperative templating in Total Hip Arthroplasty, proximal femoral osteotomies, and pediatric hip reconstructions.
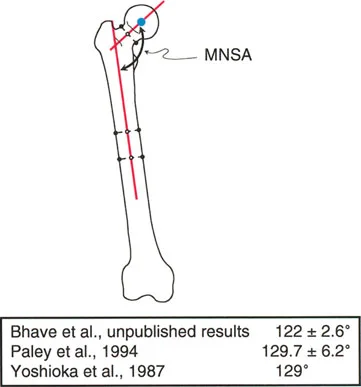
Mechanical Neck Shaft Angle
Historically, hip orientation was evaluated using the anatomic neck-shaft angle, which normally ranges from 125° to 131°. However, in deformity correction, the Mechanical Neck Shaft Angle is vital. This is the angle between the mechanical axis of the femur and the axis of the femoral neck.
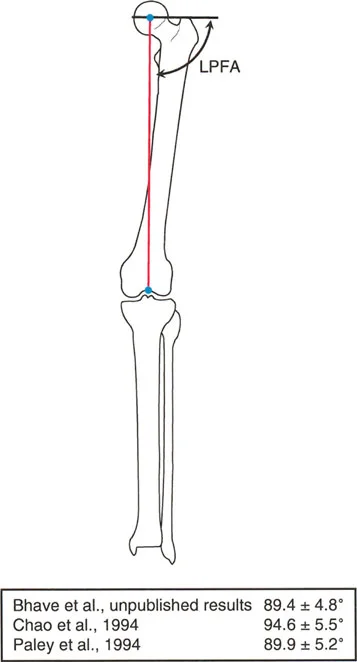
Lateral Proximal Femoral Angle
Paley and Tetsworth described a highly reproducible method to define hip orientation in the frontal plane: a line drawn from the tip of the greater trochanter to the center of the femoral head.
* The angle formed between this line and the mechanical axis of the femur is the Lateral Proximal Femoral Angle.
* Based on pooled institutional data, the accepted normal Lateral Proximal Femoral Angle is approximately 90° (range 85° to 95°).
Knee Joint Orientation
The knee joint is the most common site of lower extremity malalignment. Accurate measurement of the distal femur and proximal tibia is the cornerstone of joint preservation surgery.
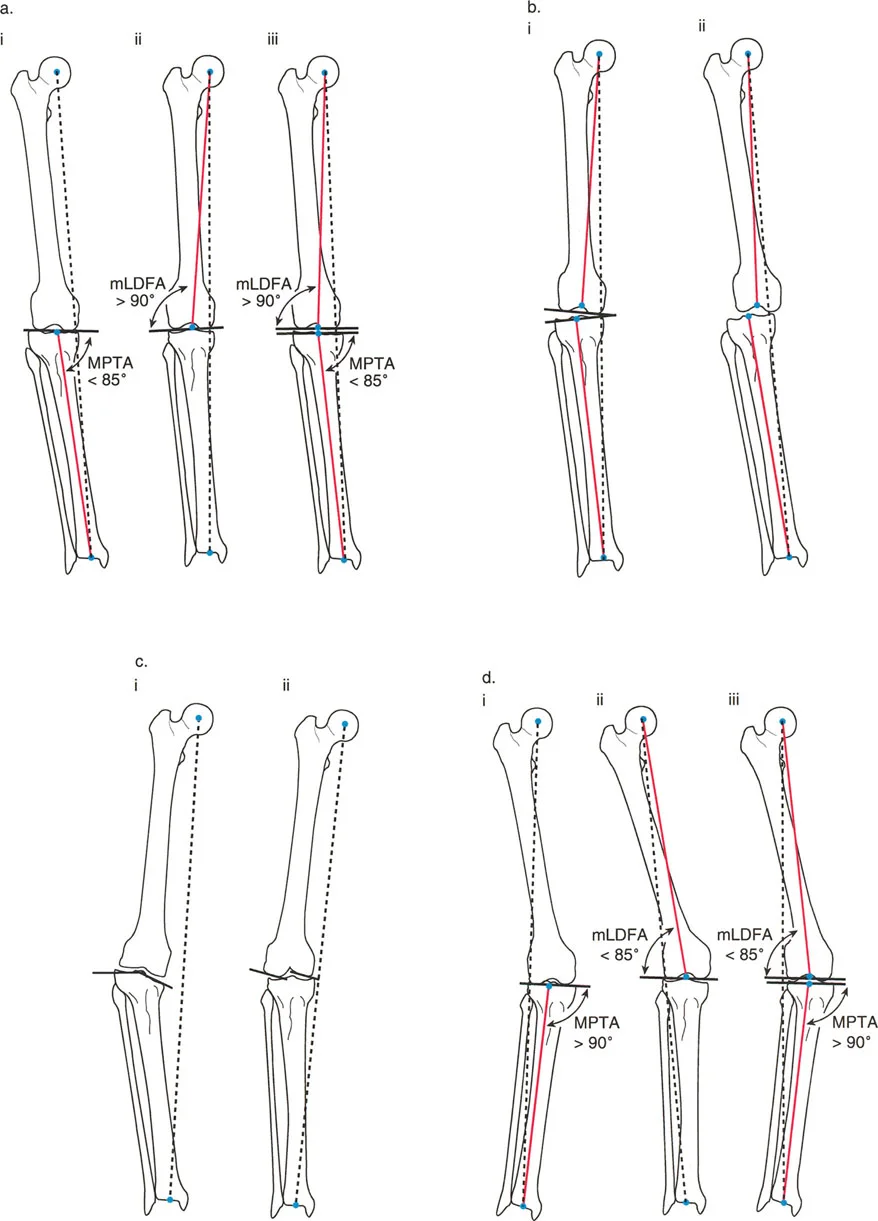
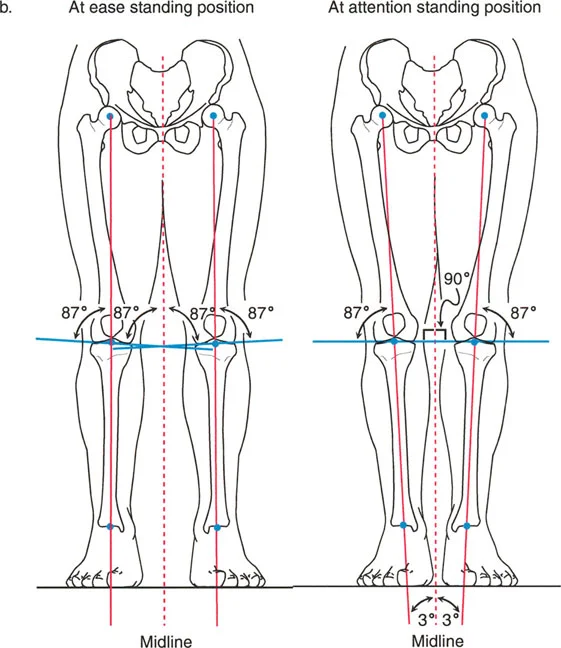
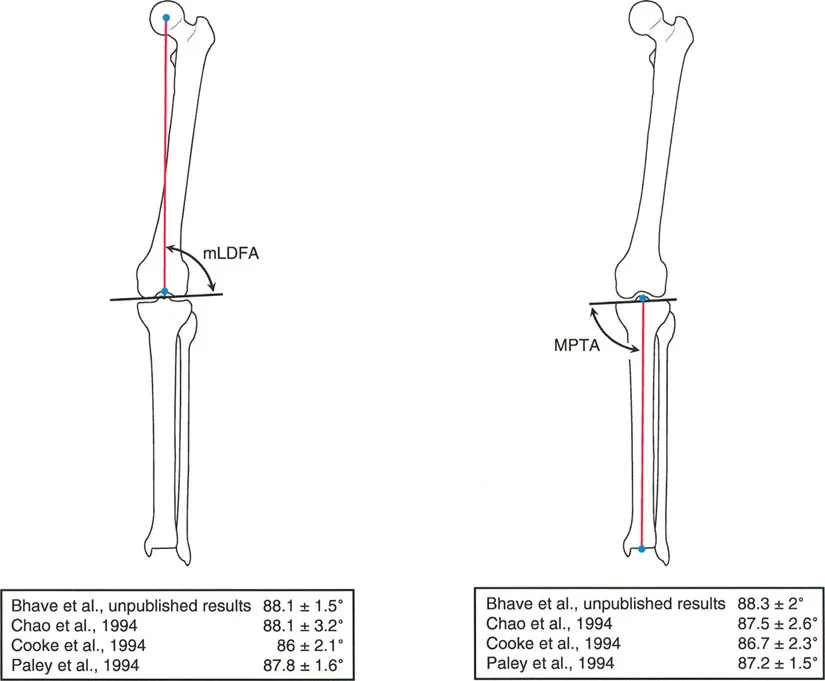
Mechanical Lateral Distal Femoral Angle
The mechanical Lateral Distal Femoral Angle (mLDFA) is the lateral angle formed between the mechanical axis of the femur and the knee joint line of the distal femur.
* Normal Value: 87.5° (Range: 85° to 90°).
* An mLDFA greater than 90° indicates a varus deformity of the distal femur. An mLDFA less than 85° indicates a valgus deformity.
Medial Proximal Tibial Angle
The Medial Proximal Tibial Angle (MPTA) is the medial angle formed between the mechanical axis of the tibia and the knee joint line of the proximal tibia.
* Normal Value: 87.5° (Range: 85° to 90°).
* An MPTA less than 85° indicates a varus deformity of the proximal tibia (common in Blount's disease or medial compartment osteoarthritis). An MPTA greater than 90° indicates a valgus deformity.
Ankle Joint Orientation
Evaluating the ankle is essential, especially when planning supramalleolar osteotomies or analyzing post-traumatic malunions of the distal tibia.
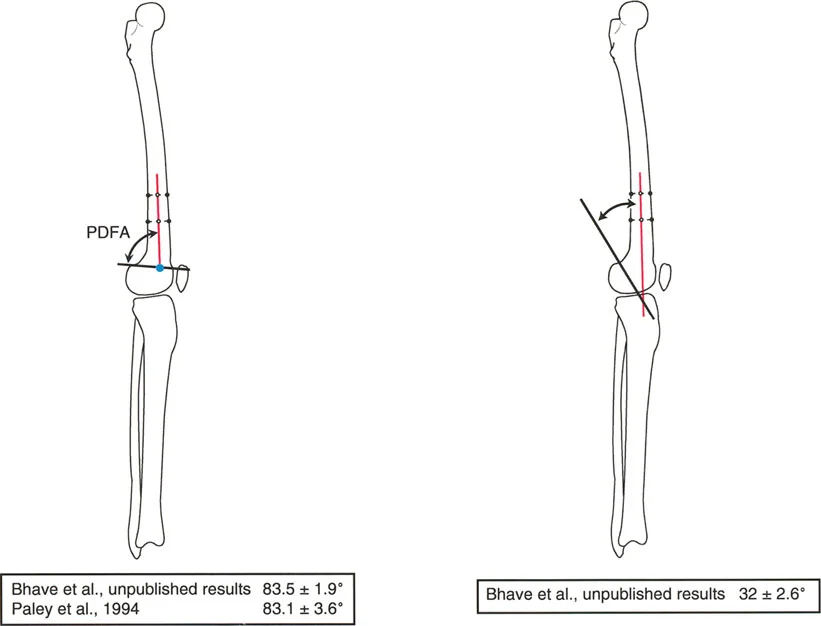
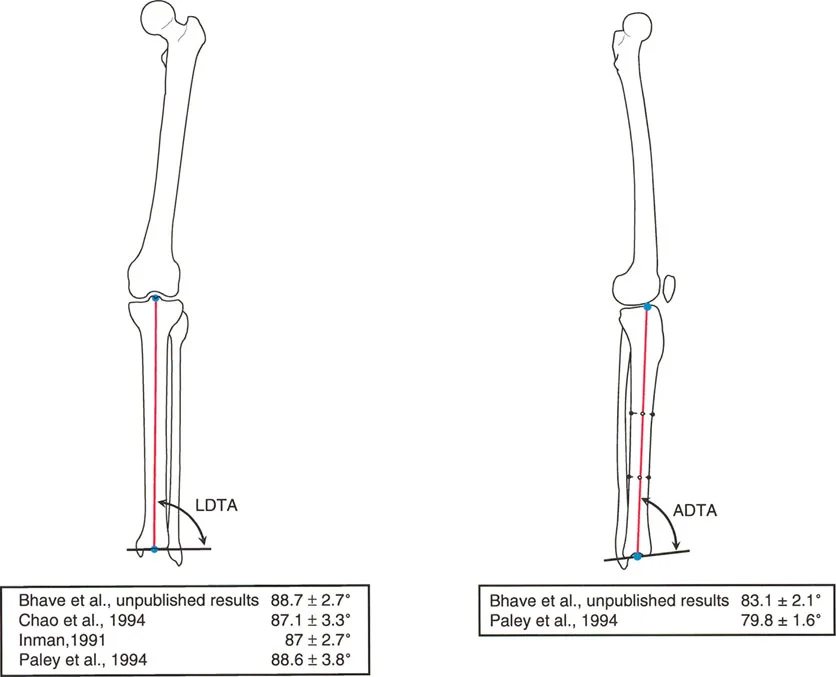
Lateral Distal Tibial Angle
The Lateral Distal Tibial Angle (LDTA) is the lateral angle formed between the mechanical axis of the tibia and the ankle joint line (tibial plafond).
* Normal Value: 89° (Range: 86° to 92°).
* Alterations in the LDTA significantly change the contact stresses across the tibiotalar joint, leading to rapid onset post-traumatic arthritis if left uncorrected.
Joint Line Convergence Angle and Soft Tissue Assessment
Not all mechanical axis deviations are caused by bony deformities. Ligamentous laxity, cartilage loss, and soft tissue contractures play a massive role in overall limb alignment. This is quantified by the Joint Line Convergence Angle.
The Joint Line Convergence Angle is the angle formed between the distal femoral joint line and the proximal tibial joint line.
* Normal Value: 0° to 2° (medial convergence).
* In a perfectly healthy knee, the joint lines are nearly parallel.
If a patient presents with a severe varus Mechanical Axis Deviation, but their mLDFA and MPTA are within normal limits, the deformity is likely intra-articular. A Joint Line Convergence Angle opening laterally indicates lateral collateral ligament laxity or severe medial compartment cartilage loss. Failing to recognize an abnormal Joint Line Convergence Angle will result in over-correcting the bone during an osteotomy.
Center of Rotation of Angulation and Deformity Apex
Dr. Paley revolutionized orthopedic deformity correction by formalizing the concept of the Center of Rotation of Angulation (CORA). Understanding the CORA is the most critical step in transitioning from simply measuring a deformity to actively correcting it.
Defining the CORA
The CORA is the point where the proximal mechanical (or anatomic) axis intersects with the distal mechanical (or anatomic) axis of a deformed bone. It represents the true apex of the deformity.
To find the CORA:
1. Draw the normal mechanical axis of the proximal bone segment.
2. Draw the normal mechanical axis of the distal bone segment.
3. The exact point where these two lines intersect is the CORA.
Single vs Multiple CORAs
A bone may have a single uniapical deformity, resulting in one distinct CORA. However, in complex trauma, osteogenesis imperfecta, or metabolic bone diseases, bones may have multiapical deformities. In these cases, the surgeon must identify multiple CORAs and plan multi-level osteotomies to restore the mechanical axis without creating secondary translation.
Paley Osteotomy Rules for Deformity Correction
Once the CORA is identified, the surgeon must decide where to cut the bone (the osteotomy site) and where to hinge the correction (the axis of correction). Dr. Paley established three fundamental rules of osteotomy that dictate how a bone will behave when corrected.
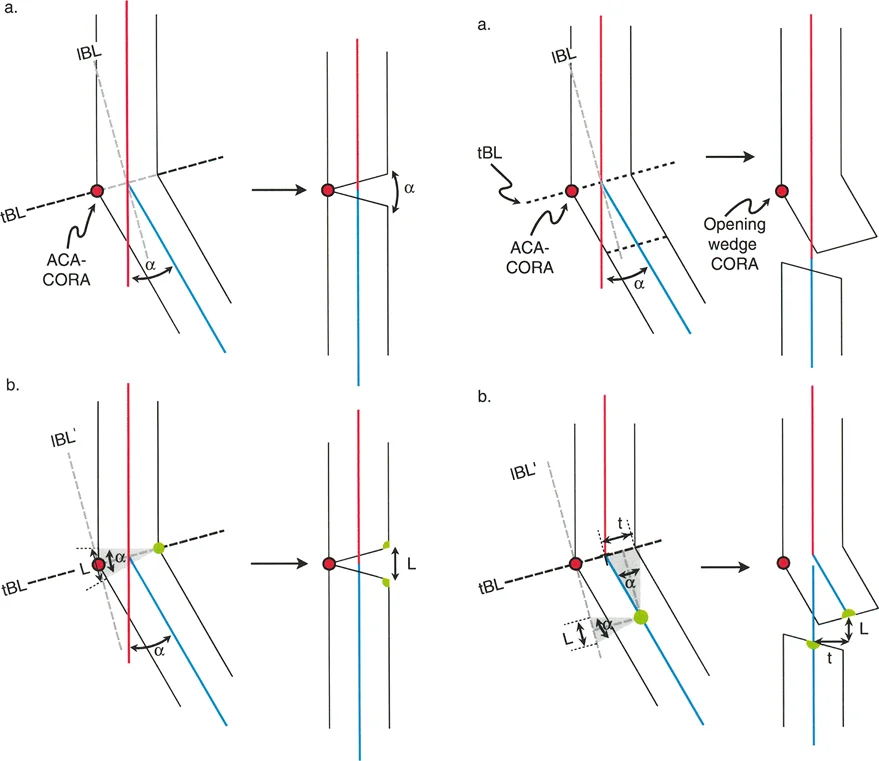
Osteotomy Rule 1
The Rule: The osteotomy and the hinge (axis of correction) are both placed exactly at the CORA.
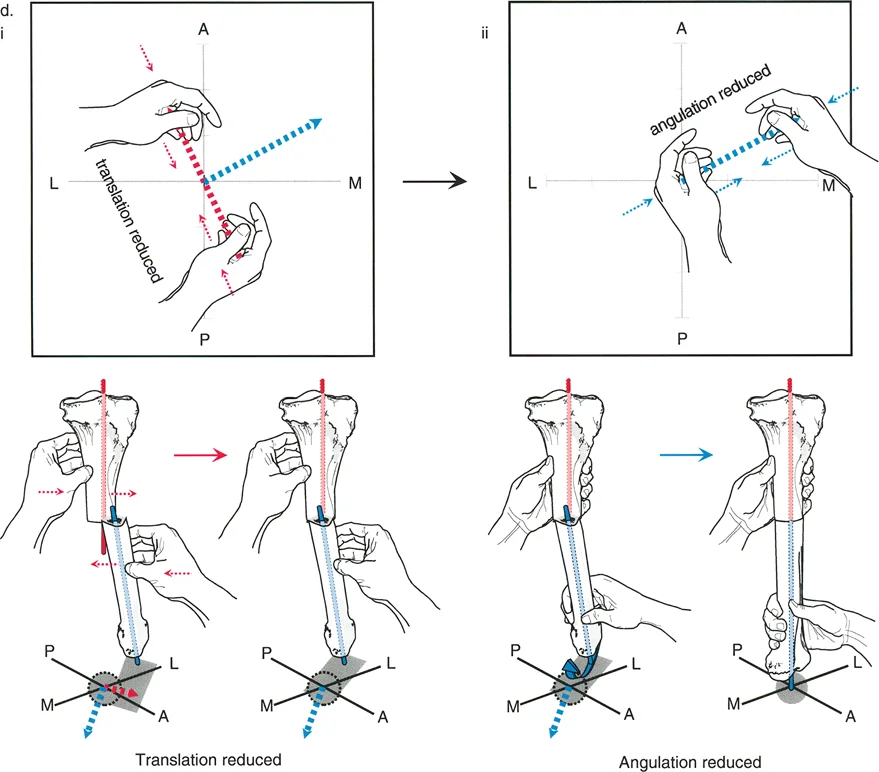
The Result: The bone undergoes pure angulation. The proximal and distal mechanical axes realign perfectly into a single, collinear straight line. There is no translation. This is the ideal scenario for deformity correction.
Osteotomy Rule 2
The Rule: The osteotomy is placed at a different level than the CORA, but the hinge (axis of correction) remains at the CORA.
The Result: The bone undergoes both angulation and translation. The proximal and distal mechanical axes realign perfectly into a collinear straight line. The translation that occurs at the osteotomy site is a necessary geometric consequence to ensure the overall mechanical axis is restored. This is frequently used when the CORA is located too close to a joint line to safely perform an osteotomy.
Osteotomy Rule 3
The Rule: The osteotomy and the hinge are both placed away from the CORA.
The Result: The bone undergoes angulation, but the proximal and distal mechanical axes do NOT become collinear—they end up parallel, resulting in a translational deformity. This creates an iatrogenic zig-zag deformity. Rule 3 is generally considered a surgical error unless the surgeon is intentionally trying to create translation to compensate for a deformity elsewhere.
Surgical Pearls for Osteotomy Execution
* Cortical Hinge: Always preserve a cortical hinge on the convex side of the deformity when using external fixation. This adds stability and guides the trajectory of the correction.
* Rule 2 Application: When performing a High Tibial Osteotomy for a CORA located inside the knee joint, you are applying Rule 2. The hinge is at the joint (CORA), but the cut is metaphyseal. This naturally results in medial translation of the distal shaft, which must be accepted to restore the mechanical axis.
Step by Step Preoperative Templating Guide
To synthesize all of Paley's principles into a clinical workflow, the surgeon must perform the "Malalignment Test." This is a systematic, step-by-step approach to evaluating every long-standing lower extremity radiograph.
Step 1: Determine the Mechanical Axis Deviation
Draw the limb mechanical axis from the center of the femoral head to the center of the ankle. Measure the distance from this line to the center of the knee. Is it varus, valgus, or normal? If abnormal, proceed to Step 2.
Step 2: Assess the Joint Line Convergence Angle
Evaluate the joint space. Is the malalignment coming from cartilage loss or ligamentous laxity? If the Joint Line Convergence Angle is abnormal, factor this soft tissue deformity into your final correction angle.
Step 3: Evaluate the Femur (mLDFA)
Measure the mechanical Lateral Distal Femoral Angle. If it falls outside the 85° to 90° range, the femur is contributing to the deformity.
Step 4: Evaluate the Tibia (MPTA)
Measure the Medial Proximal Tibial Angle. If it falls outside the 85° to 90° range, the tibia is contributing to the deformity.
Step 5: Locate the CORA and Plan the Osteotomy
If the tibia is the source of the deformity, draw the proximal and distal mechanical axes of the tibia to find the CORA. Apply Paley's Osteotomy Rules to determine the ideal level for your bone cut and hinge placement. Decide between an opening wedge, closing wedge, or dome osteotomy based on limb length discrepancies and soft tissue constraints.
Clinical Applications in Orthopedic Surgery
Paley's principles are not restricted to specialized deformity correction using Ilizarov or Taylor Spatial Frames; they are universally applicable across orthopedic subspecialties.
High Tibial Osteotomy and Distal Femoral Osteotomy
Joint preservation relies entirely on shifting the mechanical axis away from diseased cartilage. In a medial opening wedge High Tibial Osteotomy, the surgeon actively manipulates the MPTA to push the Mechanical Axis Deviation laterally, offloading the medial compartment. Precise calculation of the CORA ensures the hinge pin is placed perfectly to prevent unwanted changes in tibial slope.
Total Knee Arthroplasty
Primary and revision Total Knee Arthroplasty are essentially intra-articular deformity corrections. When templating a TKA, the surgeon uses the anatomic axes (via intramedullary guides) or mechanical axes (via navigation/robotics) to cut the distal femur at an mLDFA of 90° and the proximal tibia at an MPTA of 90°, restoring a neutral mechanical axis to the limb.
Trauma and Intramedullary Nailing
When treating distal third femur fractures or proximal third tibia fractures, the wide metaphyseal canal often leads to malreduction (the "bell-clapper" effect). By utilizing Poller screws (blocking screws) placed according to Paley's principles, the surgeon can artificially narrow the canal, forcing the intramedullary nail to align with the true anatomic axis, thereby preventing varus or valgus malunions.
Key Takeaways for the Orthopedic Surgeon
- The Mechanical Axis is King: Always evaluate the weight-bearing line from the center of the hip to the center of the ankle. A medial deviation indicates varus; a lateral deviation indicates valgus.
- Joint Orientation Dictates the Source: Use mLDFA, MPTA, and LDTA to pinpoint exactly which bone segment is responsible for the malalignment. Never assume a varus knee is strictly a tibial problem.
- Respect the Soft Tissues: The Joint Line Convergence Angle will reveal if ligamentous laxity or cartilage wear is masquerading as a bony deformity.
- Find the CORA: The intersection of the proximal and distal axes is the true apex of deformity.
- Follow the Rules: Adhering to Paley's Osteotomy Rules ensures predictable correction. Hinging at the CORA guarantees restoration of the mechanical axis without iatrogenic translation.
Mastering normal lower limb alignment and joint orientation is a lifelong pursuit. By internalizing Dr. Paley's principles, the orthopedic surgeon transitions from merely fixing bones to truly reconstructing the biomechanical foundation of the human body.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like