Paley's Principles: Advanced 3D Deformity Correction for Rotational & Angular Malalignment
Key Takeaway
Paley's principles for 3D deformity correction involve mastering axial plane understanding, precise radiographic analysis of torsion, and integrating CORA/MAD planning. This prevents complications like patellar dislocation by accurately correcting rotational and angular malalignment at the true deformity level.
Introduction to Three Dimensional Deformity Correction
Welcome to the definitive masterclass on Rotation and Angulation Rotation Deformities, heavily adapted and expanded from the foundational principles established by Dr. Dror Paley. For the orthopedic surgeon in training, mastering the frontal and sagittal planes is only the beginning. True deformity correction requires a profound spatial understanding of the axial plane and how rotational malalignment interacts with angular deformities.
When a bone is deformed in both angulation and rotation, the resulting three dimensional deformity dictates a highly specific preoperative plan. Failure to account for the exact level of the rotational deformity, the axis of correction, and the downstream effects on muscle vectors and neurovascular structures can lead to catastrophic iatrogenic complications. These include patellar dislocation, severe chondromalacia, and peroneal nerve palsy.
This comprehensive guide will walk you through the radiographic analysis of torsion, the critical decision making process for selecting osteotomy levels, the neurological minefield of rotational corrections, and the integration of rotation into Mechanical Axis Deviation and Center of Rotation of Angulation planning.
The Importance of the Axial Plane
Historically, orthopedic training has overemphasized the frontal and sagittal planes because they are easily visualized on standard orthogonal radiographs. However, the axial plane is where many functional failures occur. A femur that is perfectly straight in the coronal and sagittal planes but possesses 40 degrees of excessive anteversion will result in a severe intoeing gait, profound mechanical axis deviation during dynamic ambulation, and accelerated patellofemoral osteoarthritis.
Rotational deformities are insidious. Unlike a varus or valgus bow, torsion does not cast a clear shadow on a two dimensional X-ray. It must be actively sought out, geometrically calculated, and meticulously planned for during the execution of any corrective osteotomy.
Core Paley Principles in Rotational Deformities
To correct a complex three dimensional deformity, the surgeon must rely on the universal language of deformity correction established by Dr. Paley. This requires a thorough understanding of the Mechanical Axis, the Center of Rotation of Angulation, and the standard Joint Orientation Angles.
Center of Rotation of Angulation and Mechanical Axis Deviation
The Mechanical Axis Deviation is the distance from the center of the knee joint to the mechanical axis line drawn from the center of the femoral head to the center of the ankle mortise. In a normal limb, the MAD is zero to slightly medial (1 to 8 millimeters).
When evaluating the Center of Rotation of Angulation for an angular deformity, we find the intersection of the proximal and distal anatomical or mechanical axis lines. However, when rotation is added to the clinical picture, the concept of the CORA must be expanded into three dimensions. A rotational deformity mathematically represents an angular deformity in the transverse plane. Just as angulation has a frontal or sagittal CORA, torsion has an axial CORA.
If a derotational osteotomy is performed at a level different from the axial CORA, it induces an unintended translation of the distal segment relative to the proximal segment. This creates an iatrogenic shift in the mechanical axis, potentially worsening the patient's MAD.
Joint Orientation Angles in the Presence of Torsion
The standard joint orientation angles are the bedrock of Paley deformity planning. However, rotational deformities introduce a dangerous phenomenon known as projectional artifact.
Key angles include:
* mLDFA (Mechanical Lateral Distal Femoral Angle)
* MPTA (Medial Proximal Tibial Angle)
* LDTA (Lateral Distal Tibial Angle)
* JLCA (Joint Line Convergence Angle)
If a femur possesses severe external torsion, a standard Anteroposterior radiograph of the leg will not capture a true AP of the distal femur. The x-ray beam passes obliquely through the condyles. An anatomical valgus deformity viewed obliquely may project as a combination of valgus and flexion. Therefore, before measuring the mLDFA or MPTA, the surgeon must obtain true AP radiographs of each individual bone segment, independent of the overall limb rotation.
Radiographic Analysis of Femoral Torsion and Version
Before a surgical blade touches the skin, the surgeon must quantify the exact degree of rotational deformity. Because rotational deformities are hidden in the axial plane, they require specialized radiographic techniques and geometric analysis.
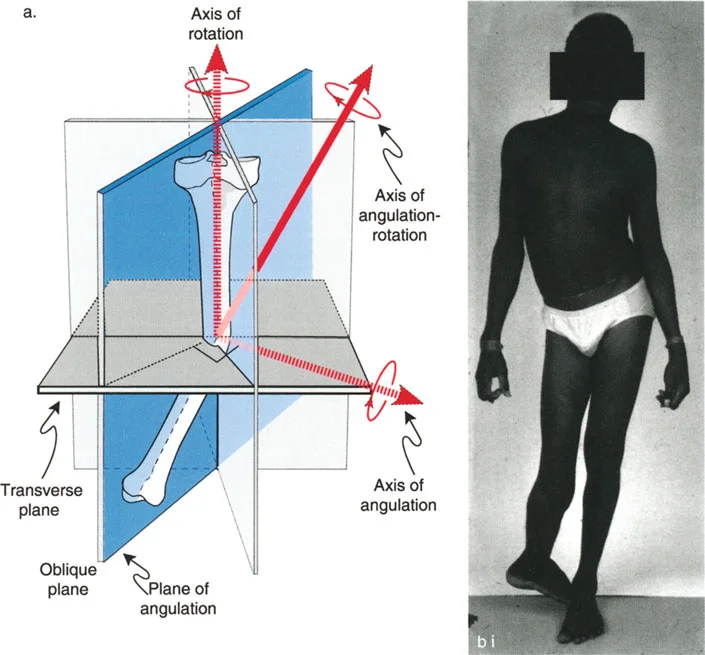
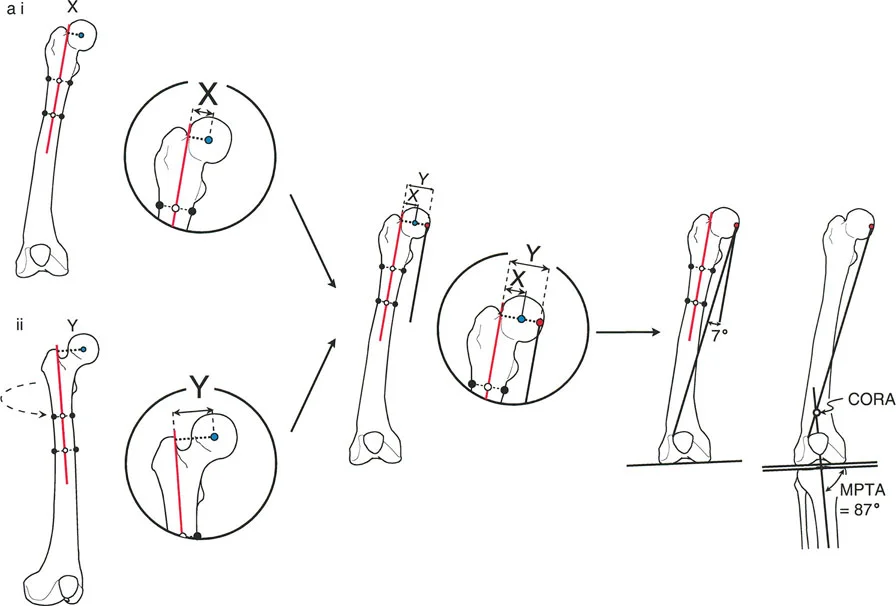
Oblique Plane Analysis for Femoral Version
The version angle of the femur can be calculated by oblique plane analysis using either graphic or trigonometric methods. The neck and the shaft of the femur are angulated to each other in a single oblique plane. The orientation of that specific oblique plane relative to the frontal plane defines the version angle.
To accurately capture this, specific radiographic protocols must be strictly adhered to.
- Patient Positioning AP and cross table lateral radiographs of the hip are obtained with the patella facing strictly forward. This is known as the knee forward position.
- Immobilization The limb must absolutely not be moved or rotated between the two views. Instead of moving the leg, the x-ray beam is moved to obtain a cross table lateral radiograph.
- Measurement The surgeon must measure the complement of the medial Neck Shaft Angle on the AP radiograph, and the complement of the anterior Neck Shaft Angle on the lateral radiograph.
Trigonometric Versus Graphic Calculation Methods
Once the AP and lateral angles are obtained, you must calculate the oblique plane defined by these two angles.
It is highly preferable to use the trigonometric method to calculate this plane. Because one of the angles is usually substantial, simple two dimensional graphic drawings introduce significant geometric error. The trigonometric formula relies on the tangents of the measured projectional angles to derive the true version angle.
If the anterior Neck Shaft Angle is small (less than 20 degrees), the graphic method may still be accurate, especially if the complement to the medial Neck Shaft Angle is 45 degrees or less. However, in the modern era of digital templating, trigonometric calculation should be the standard of care.
Always compare the calculated version angle to the opposite, theoretically normal side, or to the established normal population range.
Key Surgical Pearls for Femoral Version
* Normal femoral anteversion ranges from 5 to 20 degrees.
* Excessive anteversion leads to an intoeing gait and increased Q angle.
* Retroversion leads to an outtoeing gait and is highly associated with slipped capital femoral epiphysis and femoroacetabular impingement.
Radiographic Analysis of Tibial Torsion
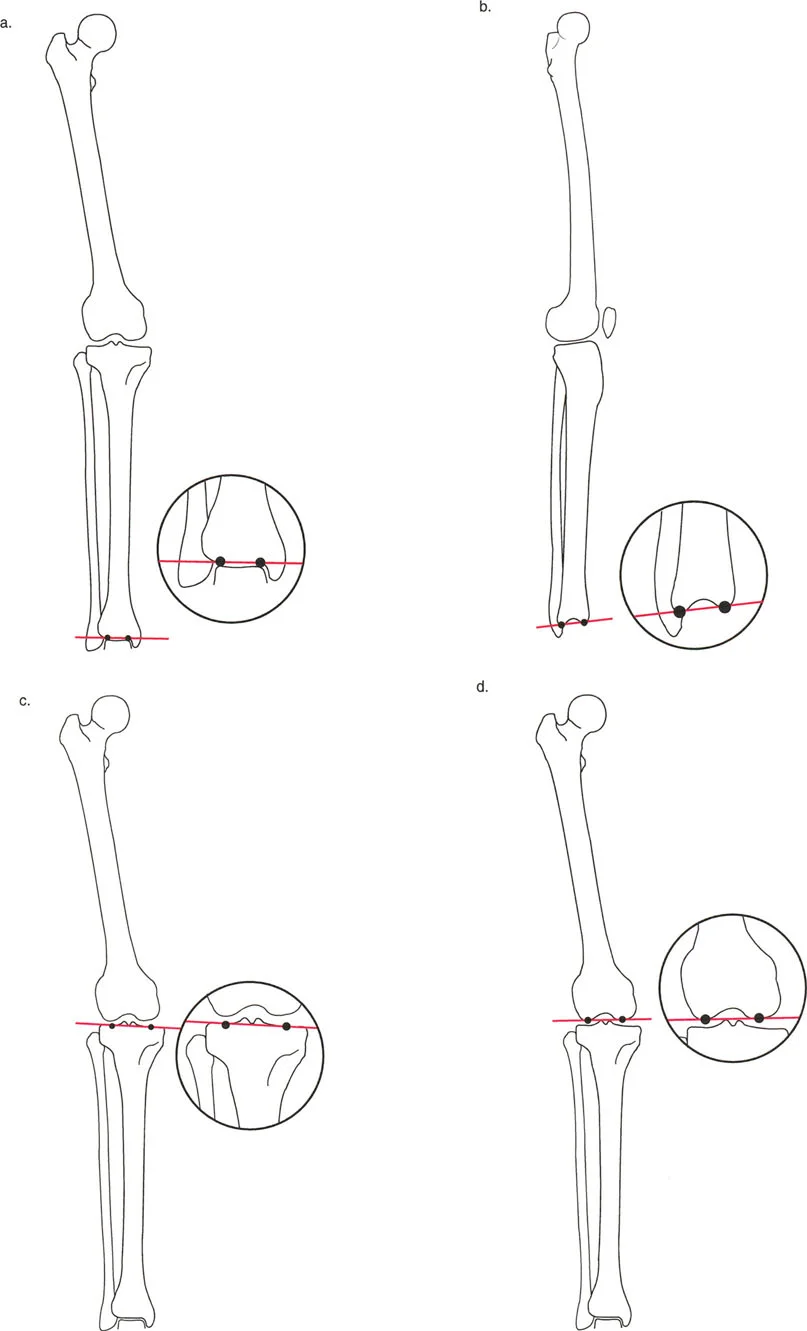
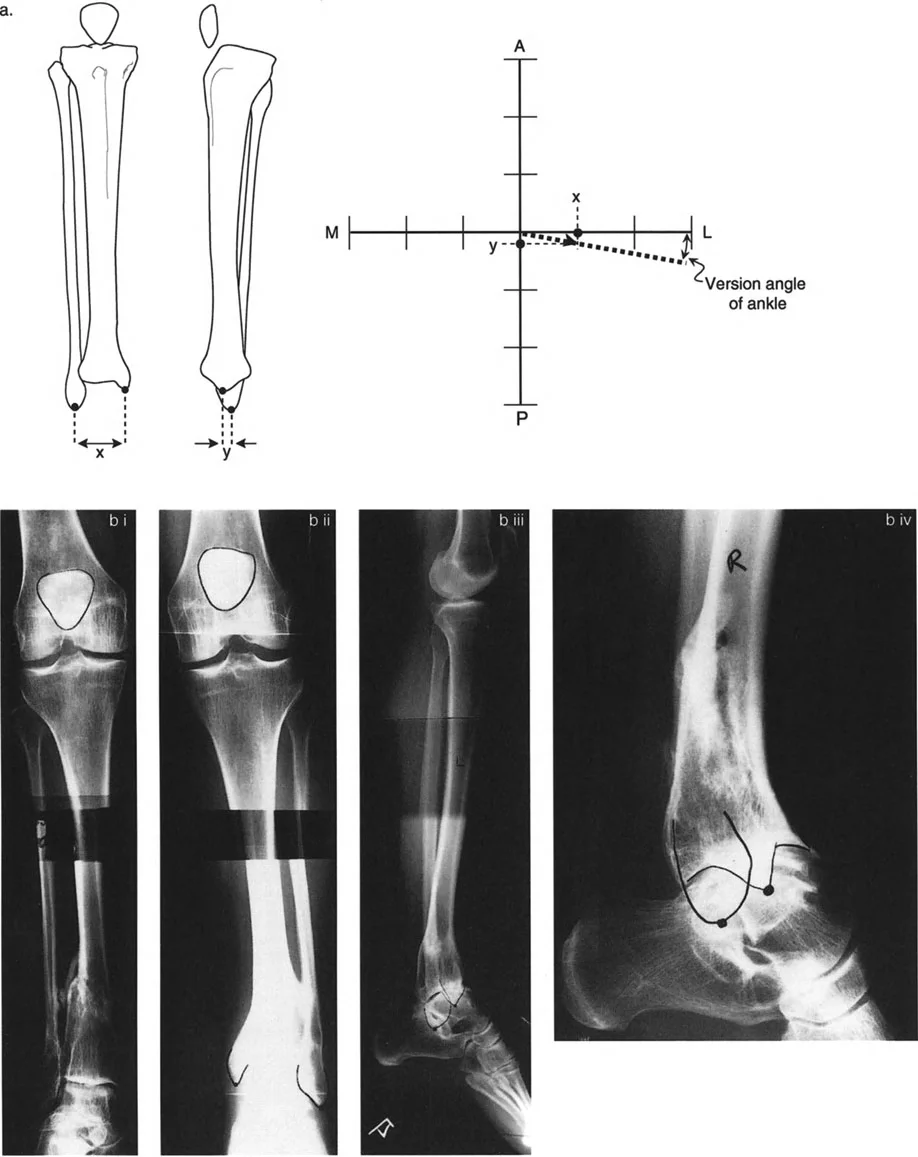
Tibial torsion analysis follows a similar logical framework to the femur but relies on different anatomical landmarks. The orientation of the plane intersecting the lateral and medial malleolus relative to the frontal plane corresponds to the degree of tibial version or torsion.
Malleolar Axis and Frontal Plane Orientation
To accurately measure tibial torsion without the use of a CT scan, strict radiographic protocols are required.
- Imaging Protocol AP and lateral radiographs of the ankle must be obtained relative to the patella forward position. The knee dictates the proximal reference, while the ankle dictates the distal reference.
- Measurement Measure the transverse distance between the medial and lateral malleoli on both the AP and Lateral radiographs.
- Plotting Plot these values on an oblique plane graph. Measure the orientation of the plane of the malleoli to the x-axis, which represents the frontal plane.
- Comparison Compare the plane of the malleoli with the plane of the opposite normal side or with the normal physiological range.
| Lower Extremity Parameter | Normal Physiological Range |
|---|---|
| Femoral Anteversion | 5 to 20 Degrees |
| Tibial Torsion | 10 to 20 Degrees External |
| Mechanical Axis Deviation | 0 to 8 mm Medial |
| mLDFA | 85 to 90 Degrees |
| MPTA | 85 to 90 Degrees |
Determining the True Level of Rotational Deformity
The level of the deformity is arguably the most critical factor to consider for angulation and translation. However, historically, the level of deformity is often ignored when addressing axial rotation. This is a critical error. Rotation is mathematically an angular deformity in the transverse plane, and it possesses a specific level.
The level of a rotation deformity is not immediately obvious, either clinically or radiographically.
Post Traumatic Versus Congenital Etiologies
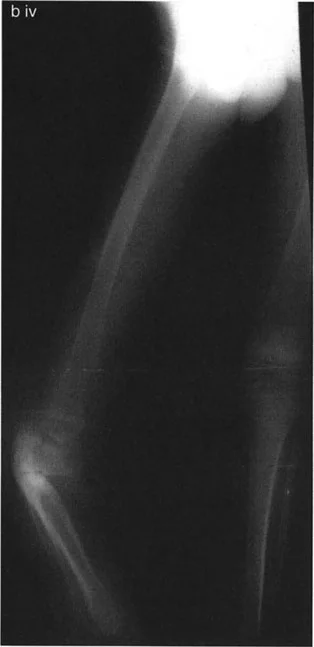
In post traumatic cases, the rotation deformity obviously occurs at the level of the healed fracture. Radiographic evidence may be present via an obvious change in the diameter of the bone at the fracture site, cortical step offs, or a visible spiral fracture pattern. The axial CORA is located exactly at the malunion site.

In congenital and developmental cases, the level of rotation deformity must be deduced clinically by the profound effect it has on the path of muscles and tendons. There is no fracture callus to guide the surgeon. The deformity may be focal, or it may be a gradual twist along the entire diaphysis of the bone.
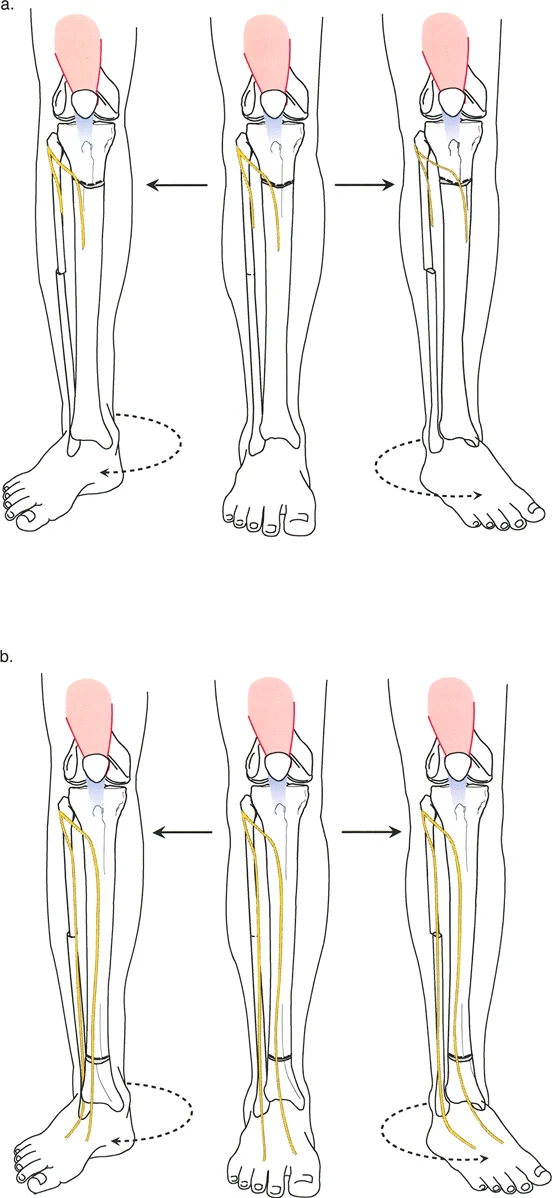
Muscle Vectors and the Quadriceps Angle
The relationship between the quadriceps muscle vector and the patellofemoral joint dictates the level of femoral osteotomy. The Q-angle is the angle formed by a line drawn from the Anterior Superior Iliac Spine to the center of the patella, and a second line drawn from the center of the patella to the tibial tubercle.
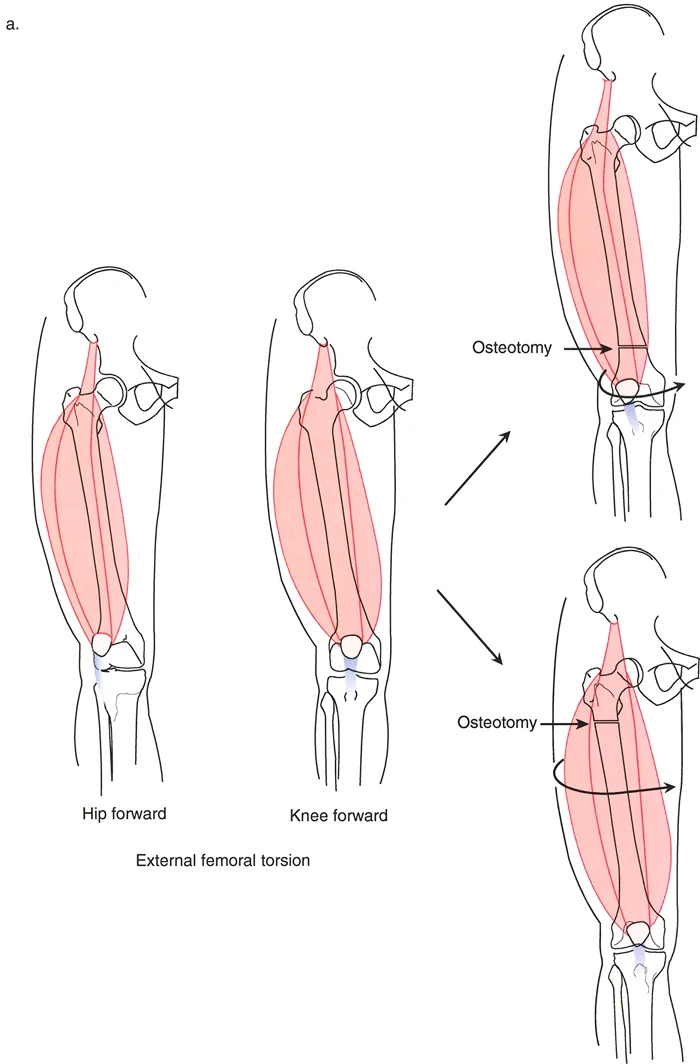
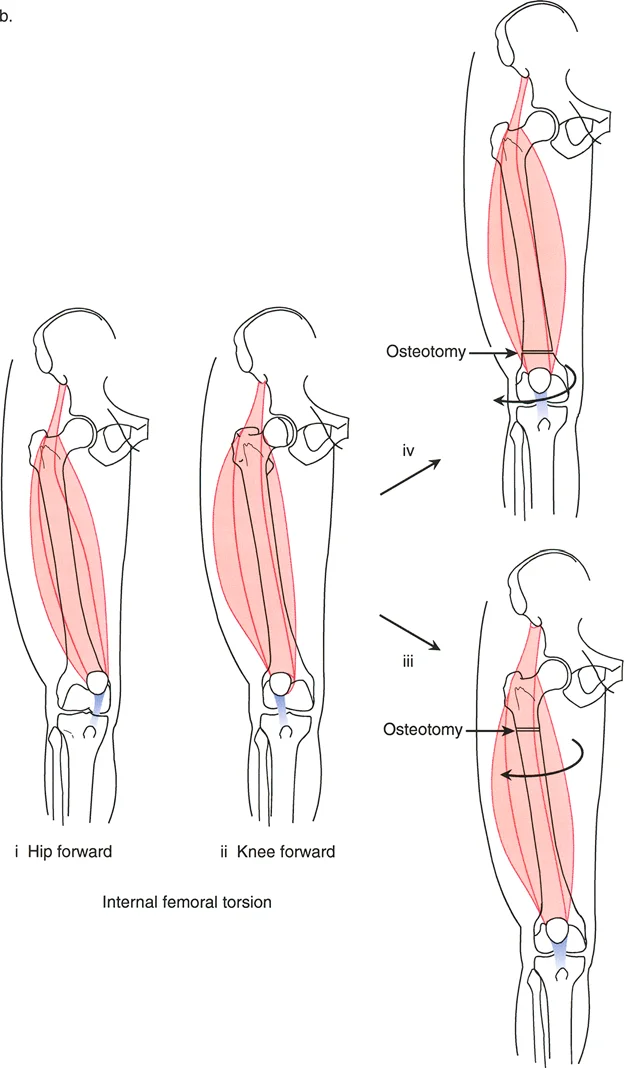
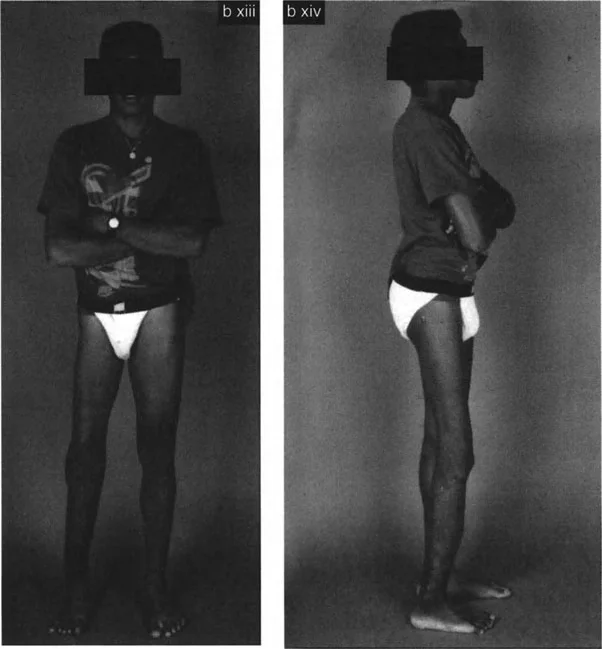
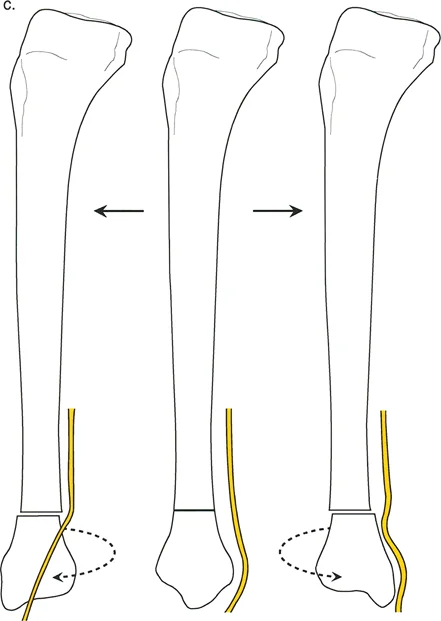
In conditions like Congenital Femoral Deficiency or congenital short femur, patients typically present with marked external rotation deformities.
Clinically, if you observe the patient, the quadriceps is laterally located relative to the hip forward position, but it is anteriorly and normally located relative to the knee forward position. This indicates that the rotational deformity is proximal to the quadriceps insertion and origin mechanics.
If the surgeon performs a distal femoral derotational osteotomy for a proximal deformity, they will successfully align the knee with the hip, but they will severely lateralize the quadriceps vector relative to the patella. This iatrogenic shift in the Q-angle guarantees lateral patellar subluxation, severe anterior knee pain, and rapid chondromalacia. Therefore, proximal deformities demand proximal osteotomies.
Applying Paley Osteotomy Rules to Angulation Rotation Deformities
Dr. Paley established three fundamental osteotomy rules for deformity correction. While traditionally taught in the context of coronal and sagittal plane angulation, these rules are absolutely vital when planning a derotational osteotomy, especially when rotation is coupled with angulation.
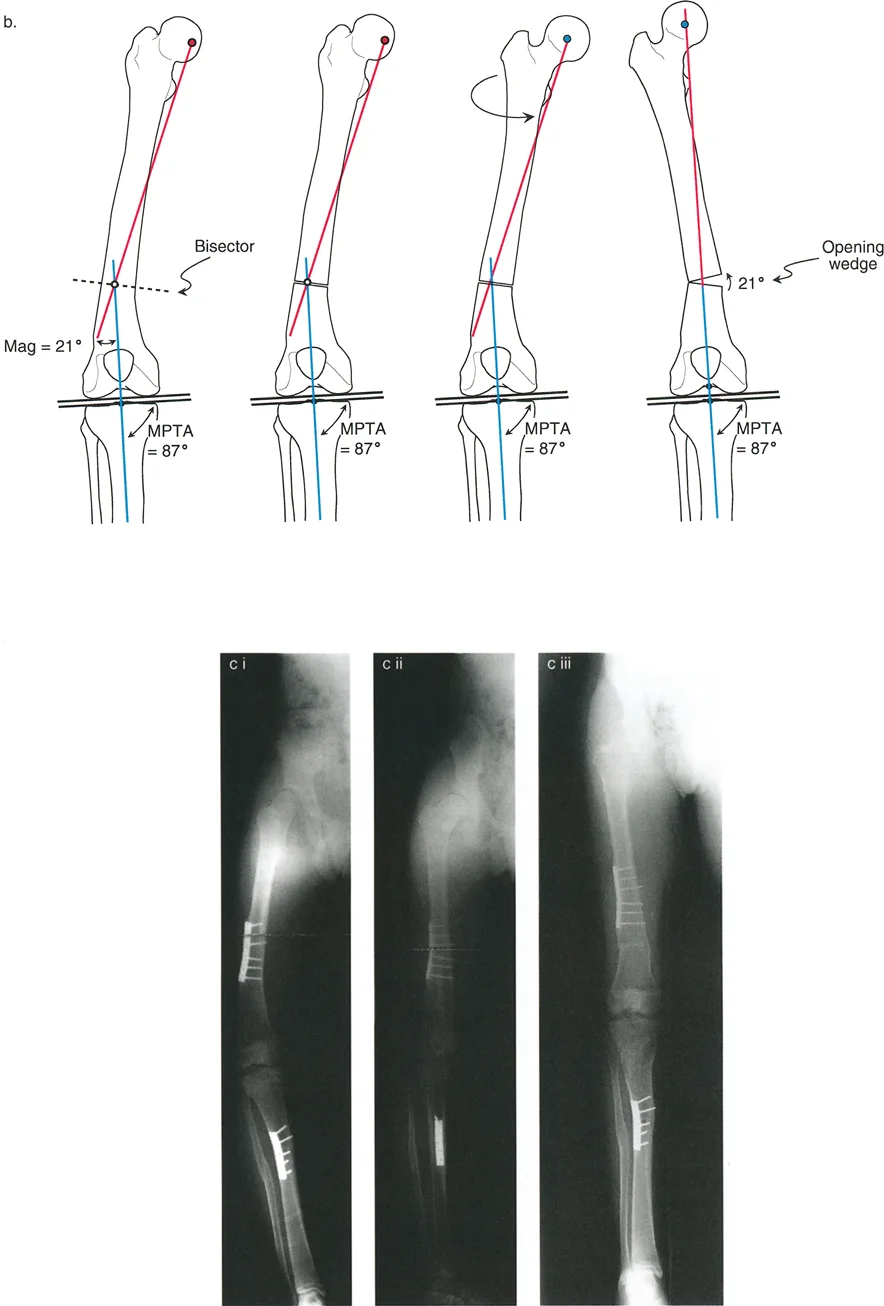
Rule One The Osteotomy and Hinge at the CORA
Paley Rule One states that when the osteotomy and the axis of correction (hinge) pass through the Center of Rotation of Angulation, complete correction of angulation and translation is achieved without creating secondary iatrogenic deformities.
In the context of a 3D deformity, if the bone has a varus bow and an internal rotation deformity at the exact same level (e.g., a midshaft femur fracture malunion), an osteotomy at this level allows for simultaneous angular correction and derotation. The mechanical axis is restored perfectly.
Rule Two The Osteotomy Outside the CORA
Paley Rule Two states that when the osteotomy is performed at a level different from the CORA, but the axis of correction remains at the CORA, the mechanical axis is restored, but a translational deformity is created at the osteotomy site.
This is highly relevant in metaphyseal deformities where poor bone stock prevents an osteotomy at the exact CORA. If a surgeon must perform a diaphyseal osteotomy to correct a juxta-articular rotational and angular deformity, they must plan for translation of the bone ends. In the transverse plane, derotating at a distance from the axial CORA physically translates the distal segment. The surgeon must allow the bone ends to shift to maintain the overall limb mechanical axis.
Rule Three The Osteotomy and Hinge Outside the CORA
Paley Rule Three states that when the osteotomy and the axis of correction are both placed outside the CORA, an iatrogenic translation deformity is created, and the mechanical axis of the limb is shifted.
This is the most common cause of failed rotational corrections. If a surgeon ignores the level of the rotational deformity and simply cuts the bone where it is surgically convenient, they are applying Rule Three. Derotating the bone around an incorrect central axis will throw the mechanical axis medial or lateral, creating a new MAD that will destroy the adjacent joints over time.
Surgical Execution of Derotational Osteotomies
Executing a derotational osteotomy requires meticulous preoperative planning and precise intraoperative technique. The choice of osteotomy geometry dictates the stability and healing potential of the correction.
Preoperative Planning Steps
- Define the Deformity Obtain long leg standing radiographs, true AP/Lateral views of each segment, and clinical rotational profiles. Calculate MAD, mLDFA, MPTA, and version angles.
- Locate the CORA Identify the exact level of the angular and rotational deformity.
- Select the Osteotomy Level Based on Paley's Rules and muscle vectors (Q-angle), choose the optimal level for the bone cut.
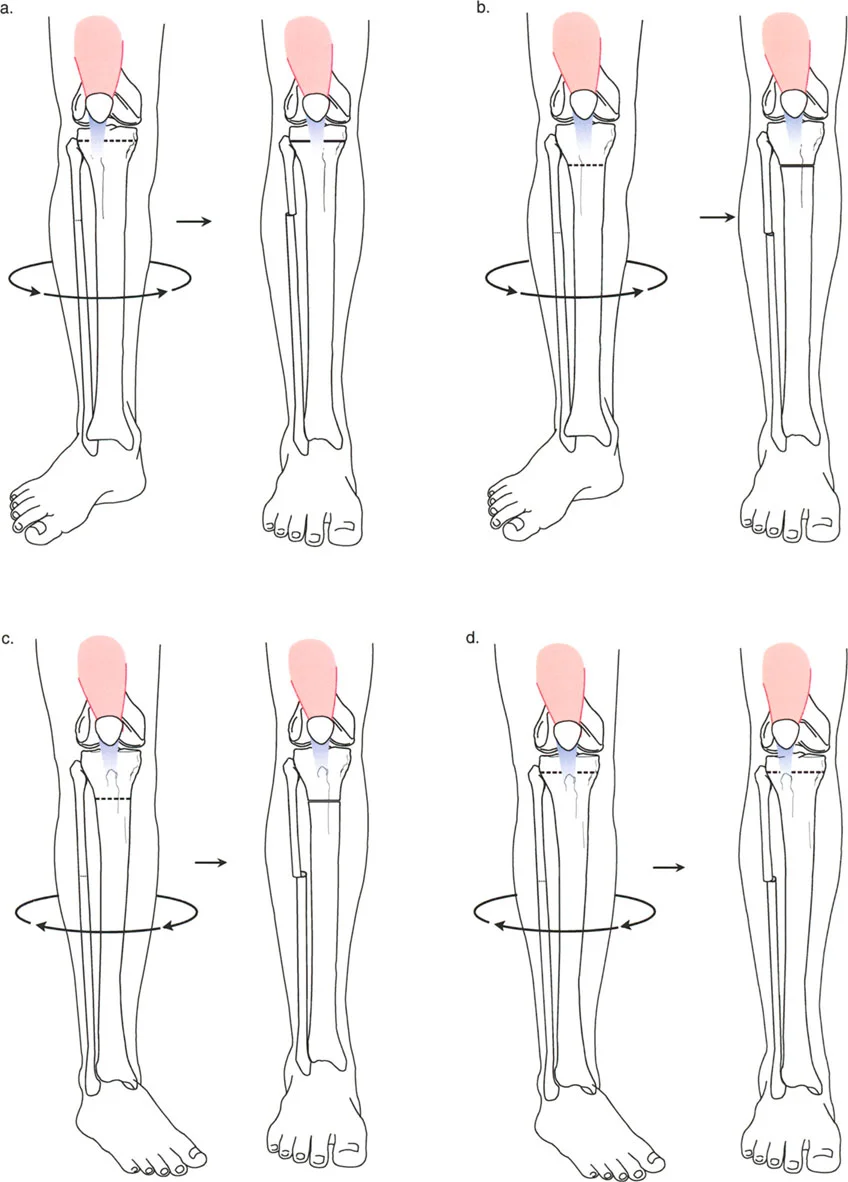
- Choose the Osteotomy Type
- Transverse Osteotomy: Excellent for pure rotation, but lacks inherent stability. Requires robust internal fixation (intramedullary nail or heavy plate).
- Focal Dome Osteotomy: Ideal for combined angulation and rotation. The cylindrical cut allows the bone ends to rotate and angulate without losing bony contact.
- Step-Cut Osteotomy: Provides excellent surface area for healing but couples rotation with lengthening or shortening depending on the geometry.
Key Surgical Pearls for Execution
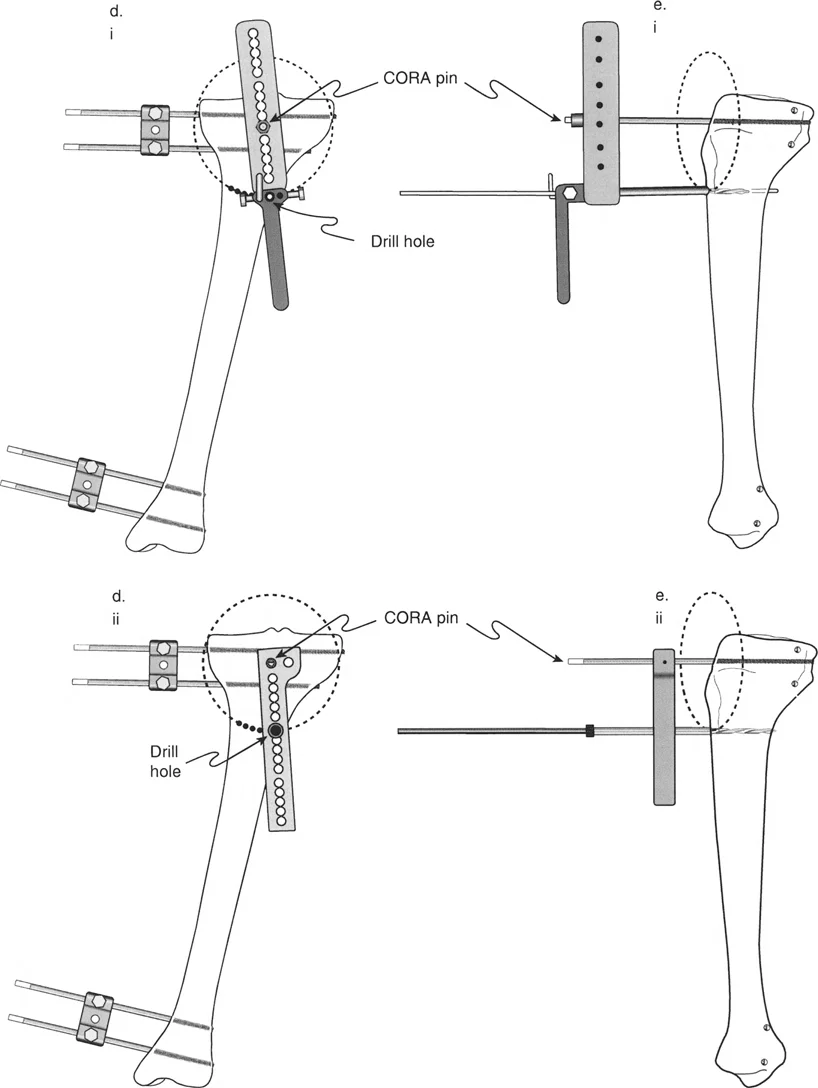
* Always place rotational reference pins proximal and distal to the planned osteotomy site before making the cut. Once the bone is divided, all anatomical landmarks are lost.
* Use a sterile goniometer intraoperatively to measure the exact degree of rotation between the reference pins.
* Ensure the soft tissue envelope is adequately released to permit the rotation without tethering.
Neurovascular Considerations and Complication Avoidance
Rotational corrections are notorious for causing neurovascular compromise. The soft tissues, nerves, and vessels are accustomed to the deformed position. Sudden acute derotation stretches these structures across unyielding fascial bands.
The most vulnerable structure in the lower extremity is the common peroneal nerve during proximal tibial derotational osteotomies.
Internal rotation of the distal tibia relative to the proximal tibia wraps the peroneal nerve tightly around the fibular neck. If an internal derotation of more than 15 to 20 degrees is planned, the surgeon must strongly consider a prophylactic peroneal nerve decompression. This involves releasing the lateral compartment fascia and the fibrous arch of the peroneus longus muscle.
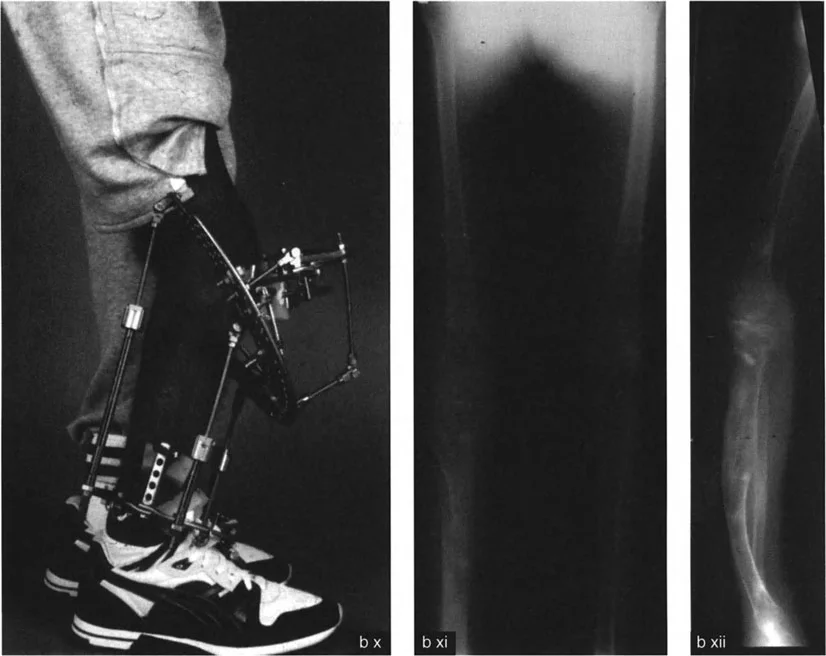
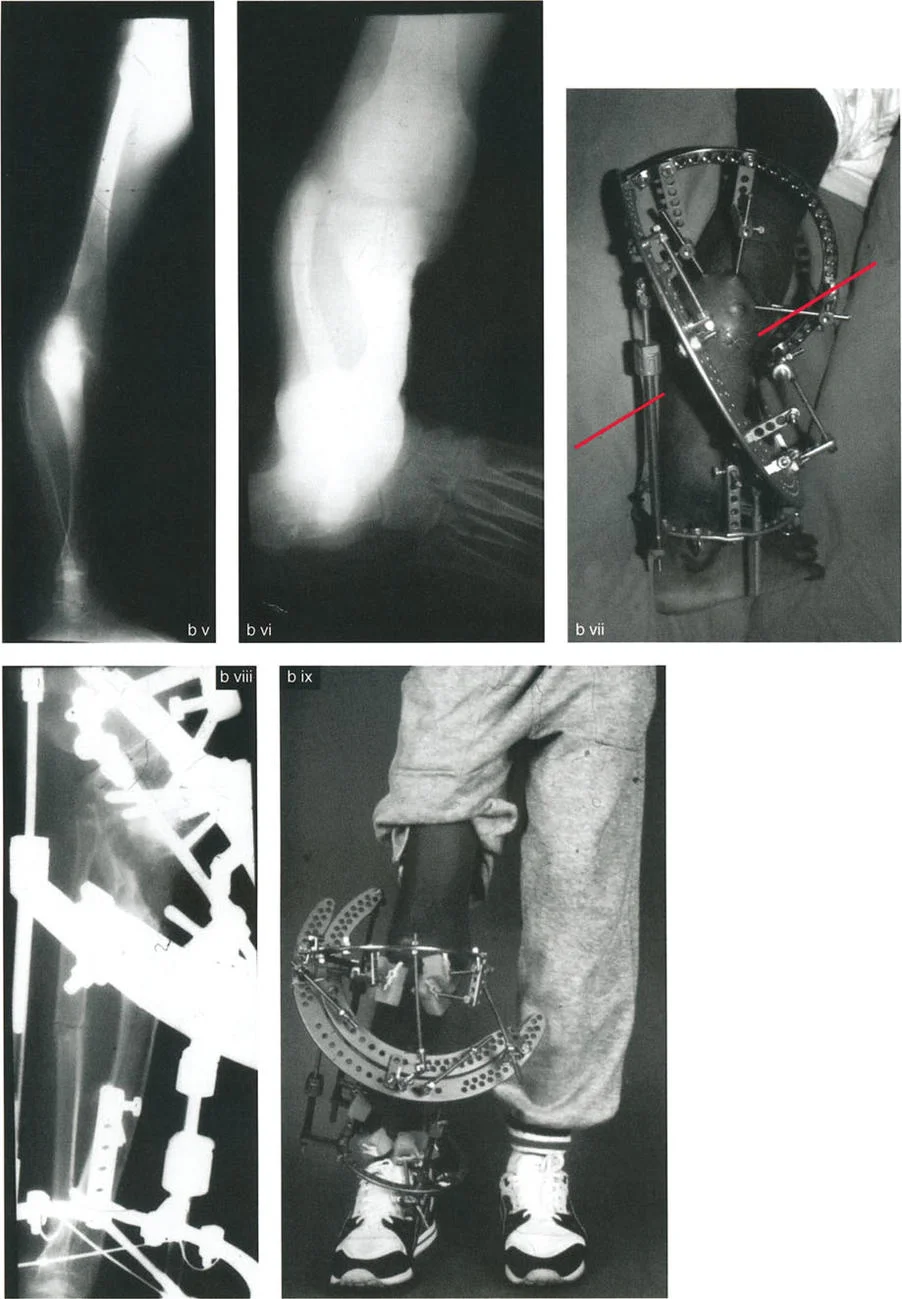
Similarly, acute external rotation of the femur can stretch the femoral artery and vein against the adductor hiatus. Careful monitoring of distal pulses and compartment pressures is mandatory in the immediate postoperative period. If vascular compromise is detected, the rotation must be dialed back, or the correction must be achieved gradually using a circular external fixator (such as an Ilizarov or Taylor Spatial Frame).
Mastering rotation and angulation rotation deformities separates the average orthopedic surgeon from the master deformity correction specialist. By rigorously applying the Paley principles of CORA, respecting the axial plane, and meticulously managing muscle vectors and neurovascular anatomy, you can achieve profound, life altering corrections for your patients.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like