Paley's Principles: Mastering Rotational Deformity Correction in Orthopedics
Key Takeaway
Paley's principles for rotational deformity correction guide orthopedic surgeons in addressing axial malalignments. They emphasize understanding biomechanics, Mechanical Axis Deviation, and precise surgical planning, especially for femoral osteotomies, to restore proper lower extremity alignment and prevent iatrogenic complications.
Introduction to Rotational Deformities in Orthopedics
In the realm of orthopedic deformity correction, mastering the multi-planar nature of the lower extremity is the hallmark of an advanced surgeon. While coronal and sagittal plane deformities such as varus, valgus, procurvement, and recurvatum are readily apparent on standard two-dimensional radiographs, axial plane deformities require a profound three-dimensional spatial awareness. Specifically, rotational deformities present unique biomechanical challenges that demand meticulous preoperative planning and surgical precision.
A rotation deformity is fundamentally defined as an abnormal angulation around an axial or longitudinal axis of a bone segment. This torsional malalignment fundamentally changes the planar orientation of the critical reference planes of the lower extremity, specifically the hip, the knee, and the ankle. When these reference planes are no longer synchronized, the biomechanical consequences are severe. Patients often experience altered gait kinematics, compensatory joint subluxation, accelerated articular cartilage wear, and debilitating patellofemoral pain syndromes due to lateral tracking of the extensor mechanism.
For the surgeon in training, understanding how to clinically isolate, radiographically quantify, and surgically correct these rotational deformities using the principles pioneered by Dr Dror Paley is absolutely essential. This comprehensive guide will deconstruct the biomechanics of rotational osteotomies, the nuances of the clinical torsional profile, and the advanced imaging techniques required to execute flawless surgical corrections without inadvertently inducing Mechanical Axis Deviation.
Core Principles of Paley in Deformity Correction
To successfully correct rotational deformities, the surgeon must first possess a fluent understanding of Dr Dror Paleys core principles of deformity correction. These principles provide a universal language and a mathematical framework for analyzing the lower limb. Correcting torsion in isolation is rare; rotational deformities often coexist with angular deformities, requiring a simultaneous multi-planar correction strategy.
Understanding Mechanical Axis Deviation
The mechanical axis of the lower extremity is defined by a line drawn from the center of the femoral head to the center of the ankle plafond. In a normally aligned limb, this line passes exactly through the center of the knee joint. Mechanical Axis Deviation occurs when this line is displaced medially or laterally relative to the center of the knee. Medial displacement results in a varus mechanical alignment, increasing contact stresses on the medial compartment, while lateral displacement results in a valgus mechanical alignment, overloading the lateral compartment.
A critical tenet of Paleys teachings is that poorly planned rotational osteotomies, particularly in the femur, can inadvertently create iatrogenic Mechanical Axis Deviation. Therefore, predicting the behavior of the mechanical axis during an axial plane rotation is the most important step in surgical planning.
Defining the Center of Rotation of Angulation
The Center of Rotation of Angulation is the point at which the proximal and distal mechanical or anatomic axis lines of a deformed bone intersect. While the Center of Rotation of Angulation is most commonly discussed in the context of coronal and sagittal plane angular deformities, the concept is equally vital when planning rotational corrections, especially when combining derotation with angular correction. Identifying the apex of the deformity ensures that the osteotomy and the subsequent correction restore normal collinear alignment.
Normal Joint Orientation Angles
Joint orientation angles describe the relationship between the mechanical or anatomic axes of a bone and its respective joint lines. Evaluating these angles allows the surgeon to isolate whether a deformity is originating from the femur, the tibia, or both.
| Joint Orientation Angle | Abbreviation | Normal Value Range |
|---|---|---|
| Mechanical Lateral Distal Femoral Angle | mLDFA | 85 to 90 degrees (Avg 87) |
| Medial Proximal Tibial Angle | MPTA | 85 to 90 degrees (Avg 87) |
| Joint Line Convergence Angle | JLCA | 0 to 2 degrees |
| Lateral Distal Tibial Angle | LDTA | 86 to 92 degrees (Avg 89) |
| Mechanical Lateral Proximal Femoral Angle | mLPFA | 85 to 95 degrees (Avg 90) |
When a severe rotational deformity is present, standard anteroposterior radiographs may misrepresent these angles due to projectional artifact. For instance, severe external tibial torsion may make a normal MPTA appear artificially in varus or valgus depending on the rotation of the cassette. True joint orientation angles must be measured with the x-ray beam perfectly perpendicular to the specific joint being evaluated.
Biomechanics of Rotational Osteotomies
The most critical concept to grasp when planning a rotational correction is the relationship between the bones anatomic axis, defined as the mid-diaphyseal line, and its mechanical axis. The behavior of a bone during a purely rotational osteotomy depends entirely on whether these two axes are parallel or divergent.
Tibial Rotational Osteotomies and the Mechanical Axis
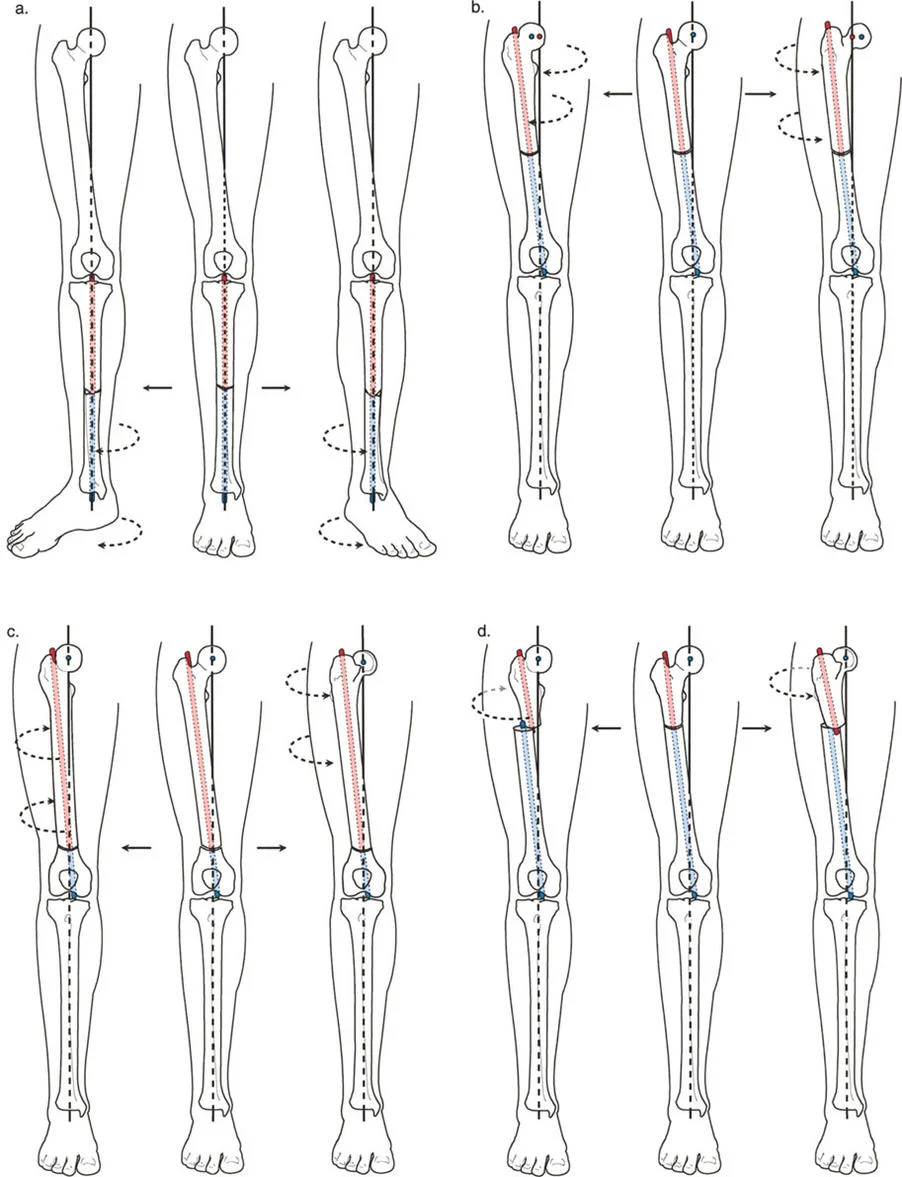
In the tibia, the mechanical axis and the anatomic axis are essentially collinear in the frontal plane. Because the mechanical axis of the lower limb passes directly down the center of the tibial diaphysis, performing a rotational osteotomy around the anatomic axis of the tibia does not displace the mechanical axis.
Therefore, rotational osteotomies around the anatomic or mechanical axis of the tibia do not produce any Mechanical Axis Deviation in the frontal plane. The rotational axis remains parallel to the mechanical axis of the lower limb, making diaphyseal tibial derotations biomechanically forgiving. A surgeon can perform a mid-shaft tibial osteotomy, rotate the distal segment internally or externally, and rest assured that the knee and ankle joint centers will remain mechanically aligned.
Femoral Rotational Osteotomies and the Danger Zone
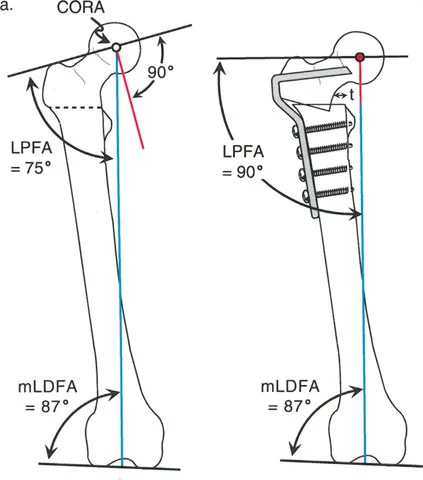
The femur presents a completely different biomechanical challenge. Unlike the tibia, the anatomic axis of the femur is not parallel to the mechanical axis of the lower limb, nor does it pass through the center of the femoral head. There is a natural angle, typically 7 degrees, between the femoral anatomic and mechanical axes.
This divergence dictates strict rules for femoral osteotomies. If a surgeon performs a rotational osteotomy through the femoral diaphysis and rotates the bone around its anatomic axis, they will inadvertently produce profound Mechanical Axis Deviation. As the distal femur rotates internally or externally around the anatomic axis, the center of the femoral head acts like a crank, swinging medially or laterally in the frontal plane relative to the anatomic axis. This creates an iatrogenic varus or valgus mechanical alignment.
To avoid this complication, one might attempt to rotate the femur around its mechanical axis. However, in the proximal femur, the mechanical axis is highly eccentric, passing through the femoral head far medial to the shaft. A proximal femoral osteotomy rotated around the mechanical axis produces massive, unacceptable translation of the diaphyseal bone ends, making it surgically impractical.
The sweet spot for femoral derotation is in the distal femur. Here, the mechanical and anatomic axis lines intersect, and the cross-section of the metaphyseal bone is at its widest. Rotation around the mechanical axis in the distal femur is highly practical, provides excellent bone contact for healing, and does not induce Mechanical Axis Deviation.
Clinical Assessment of Torsional Profiles
While advanced imaging is the gold standard for precise preoperative planning, the clinical assessment remains the cornerstone of diagnosing rotational deformities. A comprehensive physical examination must be performed to generate a complete torsional profile, as originally described by Staheli. Clinical assessment, when performed meticulously, has been shown to be highly accurate for initial diagnostic purposes and dictates the necessity of further imaging.
Evaluating the Foot Progression Angle
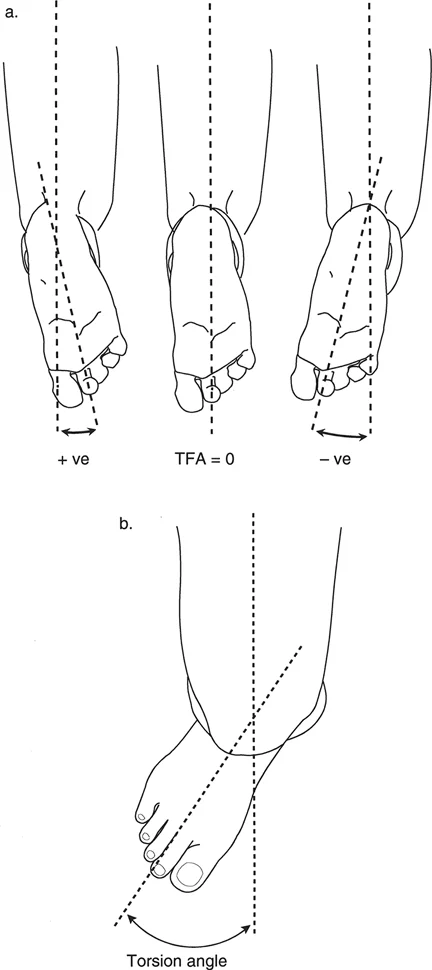
The assessment begins with observing the patients gait. The foot progression angle is the angle between the long axis of the foot and the straight line representing the direction of walking. An inward pointing foot represents a negative angle, commonly referred to as in-toeing, while an outward pointing foot represents a positive angle, known as out-toeing.
- Clinical Pearl: The foot progression angle can be highly deceptive. A patient may have a severe internal femoral torsion but present with a normal foot progression angle if they have developed a compensatory external tibial torsion. This is known as miserable malalignment syndrome. Therefore, the foot progression angle is merely an observation of the sum total of lower extremity rotation, not a diagnostic measurement of a specific bone.
Hip Internal and External Rotation Assessment
To isolate femoral torsion, the surgeon must evaluate hip range of motion. The most accurate clinical method is to assess the patient in the prone position with the knees flexed to 90 degrees. Gravity allows the lower legs to fall outward, indicating internal hip rotation, or cross inward, indicating external hip rotation.
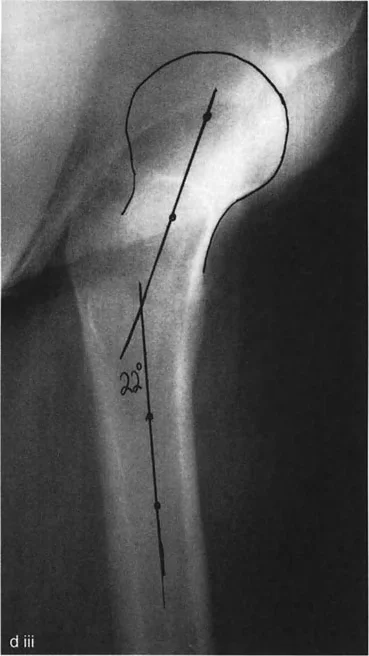
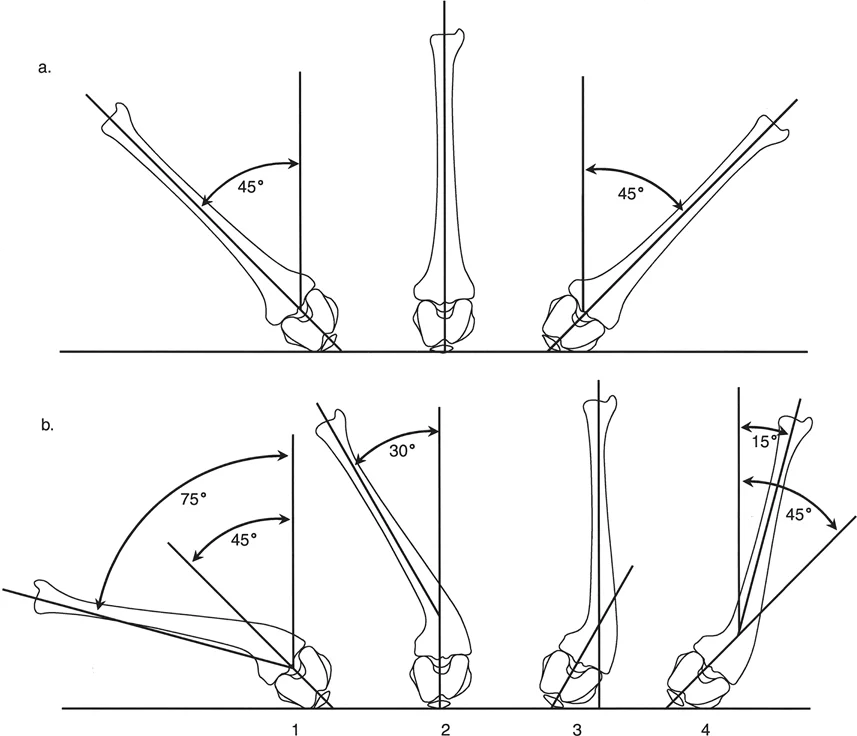
Normal internal rotation is typically between 30 and 40 degrees, and normal external rotation is between 40 and 50 degrees. In patients with excessive femoral anteversion, internal rotation will be significantly increased, often exceeding 70 degrees, while external rotation will be restricted. Craigs test can also be performed in this position by palpating the greater trochanter and internally rotating the hip until the trochanter is maximally prominent laterally. The angle of the tibia relative to the vertical axis represents the clinical estimate of femoral anteversion.
Transmalleolar Axis and Thigh Foot Angle
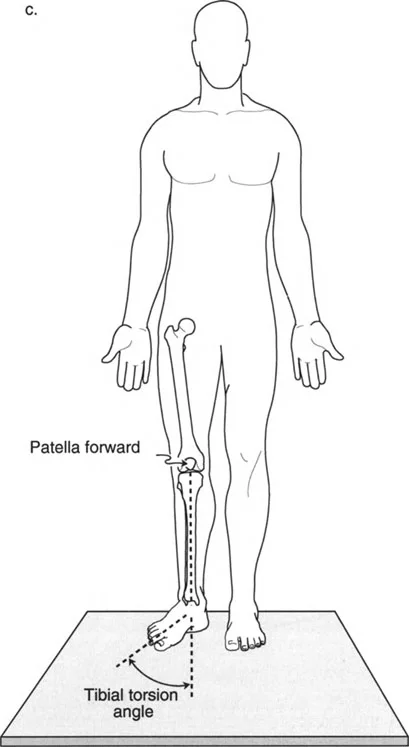
Tibial torsion is isolated by evaluating the thigh foot angle and the transmalleolar axis. With the patient prone and the knee flexed to 90 degrees, the surgeon views the foot from above. The thigh foot angle is the angle between the longitudinal axis of the thigh and the longitudinal axis of the foot. Normal values range from 10 to 15 degrees of external rotation.
Alternatively, the transmalleolar axis can be measured by placing the thumb and index finger on the medial and lateral malleoli. The angle of an imaginary line connecting these points relative to the coronal plane of the knee provides a highly accurate clinical representation of tibial torsion.
Radiographic Evaluation of Rotational Deformities
Once the clinical exam identifies a rotational abnormality, advanced imaging is required to quantify the deformity and formulate a precise surgical plan. Standard two-dimensional radiographs are insufficient for measuring torsion, though they remain critical for evaluating concurrent angular deformities and joint orientation.
Computed Tomography for Torsional Measurement
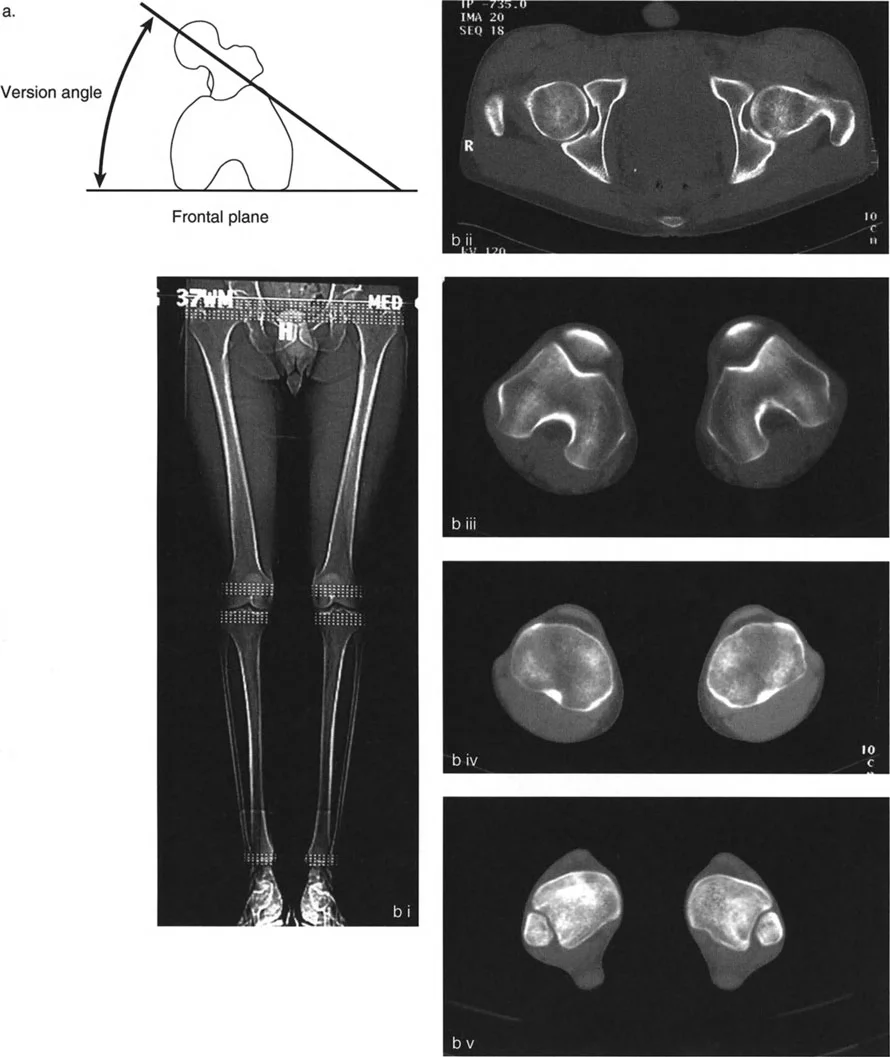
Computed Tomography is the gold standard for quantifying femoral and tibial torsion. A standard torsional CT protocol involves acquiring axial slices at specific anatomical landmarks. For the femur, slices are taken through the center of the femoral head and neck, and through the distal femoral condyles. The angle between the axis of the femoral neck and the posterior condylar axis defines true femoral version.
For the tibia, slices are taken through the proximal tibial plateau and the distal tibial plafond. The angle between the posterior margin of the proximal tibia and the bimalleolar axis defines tibial torsion.
When evaluating CT scans, the surgeon must be aware of normal population variances. Normal femoral anteversion in an adult is typically 15 degrees, while normal external tibial torsion is approximately 20 to 30 degrees. Deformity correction is generally indicated when measurements deviate by more than 15 degrees from the norm, particularly if the patient is symptomatic.
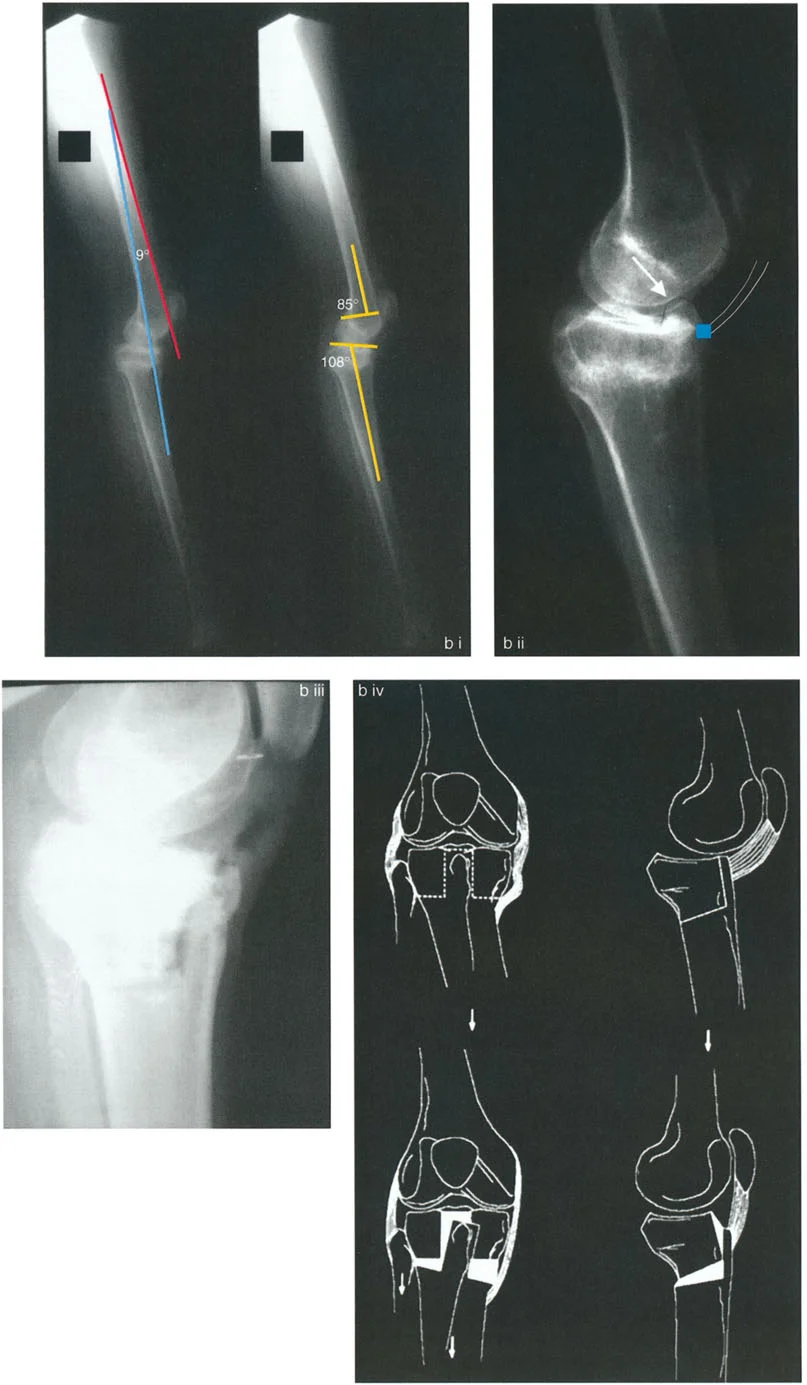
Radiographic Joint Orientation Angles
While CT handles the axial plane, standard long leg alignment radiographs are mandatory for evaluating the coronal and sagittal planes. Dr Paley emphasizes that rotational deformities rarely exist in a vacuum. The surgeon must meticulously measure the mechanical Lateral Distal Femoral Angle and the Medial Proximal Tibial Angle to ensure no hidden angular deformities are missed.
If an angular deformity is identified alongside a rotational deformity, the surgeon must plan a multi-planar correction. This involves calculating the true magnitude and direction of the deformity using Paleys multiplier method or modern deformity planning software, ensuring that the osteotomy addresses all planes simultaneously.
Surgical Planning Using the CORA Method
The execution of a flawless rotational osteotomy relies heavily on the application of Paleys Osteotomy Rules. These rules dictate the relationship between the osteotomy site, the Center of Rotation of Angulation, and the resulting alignment of the bone segments.
Determining the Center of Rotation of Angulation
The first step in surgical planning is locating the Center of Rotation of Angulation. On a standing long leg radiograph, the surgeon draws the proximal and distal mechanical axes of the deformed bone. The point where these lines intersect is the Center of Rotation of Angulation.
In a pure rotational deformity without angular deviation, the mechanical axes are collinear, meaning the Center of Rotation of Angulation is technically infinite or nonexistent in the coronal plane. However, when combined with varus or valgus, pinpointing this intersection is mandatory.
Applying Paleys Osteotomy Rules
Dr Paley outlined three fundamental rules for osteotomies that every orthopedic surgeon must memorize.
- Rule One: When the osteotomy passes through the Center of Rotation of Angulation, and the axis of correction is at the Center of Rotation of Angulation, the bone ends will angulate without translation, restoring perfect collinear alignment of the mechanical axis.
- Rule Two: When the osteotomy is performed outside the Center of Rotation of Angulation, but the axis of correction remains at the Center of Rotation of Angulation, the mechanical axis will be restored to a collinear state, but the bone ends will translate at the osteotomy site. This translation is often necessary for diaphyseal healing but must be accounted for in hardware placement.
- Rule Three: When the osteotomy and the axis of correction are both outside the Center of Rotation of Angulation, the proximal and distal mechanical axes will become parallel but not collinear, resulting in an iatrogenic translation deformity and Mechanical Axis Deviation.
When correcting pure torsion, Rule One and Rule Two are most applicable. The surgeon must ensure that the axis of rotational correction aligns with the true mechanical axis of the limb, particularly in the femur, to avoid violating Rule Three.
Execution of Femoral Derotation Osteotomies
Executing a femoral derotation requires meticulous intraoperative technique to ensure the exact degree of planned rotation is achieved without inducing unwanted coronal or sagittal plane translation.
Distal Femoral Osteotomy Techniques
As established in the biomechanics section, the distal femur is the optimal location for femoral derotation. The surgical approach typically involves a lateral incision over the distal femur. Before the osteotomy is performed, reference wires are absolutely critical.
The surgeon places a smooth Kirschner wire into the anterior aspect of the distal femur, parallel to the joint line. A second Kirschner wire is placed proximal to the planned osteotomy site. The angle between these two wires in the axial plane should precisely match the planned degree of rotational correction.
Once the reference wires are placed, a transverse or slightly oblique osteotomy is performed in the supracondylar region. The distal segment is then rotated until the two reference wires are perfectly parallel. Fixation is typically achieved using a lateral locking plate or a retrograde intramedullary nail. Intramedullary nailing offers the advantage of load sharing and excellent control of the mechanical axis, provided the entry point is perfectly aligned with the mechanical axis of the distal femur.
Proximal Femoral Osteotomy Considerations
While distal osteotomies are preferred for pure rotation, proximal femoral osteotomies are indicated when the rotational deformity is combined with a proximal angular deformity, such as coxa vara, or when addressing complex hip dysplasia.
Subtrochanteric osteotomies require extreme care. Because the osteotomy is far from the mechanical axis, any rotation must be strictly controlled to prevent lateral or medial translation of the femoral shaft. Fixation is usually achieved with a cephalomedullary nail or a proximal femoral locking plate. The surgeon must accept that some degree of anatomical axis translation is inevitable and must prioritize mechanical axis alignment over radiographic appearance of the bone cortex.
Execution of Tibial Derotation Osteotomies
Tibial derotation is biomechanically more forgiving than femoral derotation but presents its own unique set of soft tissue and anatomical challenges, most notably the presence of the fibula and the proximity of the common peroneal nerve.
Tibial Diaphyseal Derotation Strategies
Tibial osteotomies can be performed in the proximal metaphysis, the diaphysis, or the distal metaphysis. Diaphyseal osteotomies are highly effective for pure rotational corrections.
Intraoperative control of rotation is achieved similarly to the femur, using parallel reference wires placed proximal and distal to the planned cut. The surgeon must ensure that the osteotomy is perfectly transverse. An oblique osteotomy cut will inadvertently cause coronal or sagittal plane angulation when the bone is rotated, turning a simple axial plane correction into a complex multi-planar deformity.
Fixation of tibial diaphyseal osteotomies is most commonly performed with a reamed antegrade intramedullary nail. The nail provides excellent bending stability while allowing the surgeon to lock the rotation dynamically. External fixation, particularly hexapod circular frames, is another powerful tool in the Paleys armamentarium. Circular frames allow for gradual, precise postoperative adjustment of rotation, which is highly advantageous in complex cases or when soft tissue compliance is a concern.
Managing the Fibula During Tibial Derotation
A critical surgical pearl in tibial derotation is the management of the fibula. The tibia cannot be rotated more than a few degrees without intact fibular resistance causing massive stress on the proximal and distal tibiofibular joints. Therefore, a concomitant fibular osteotomy is almost always required.
The fibular osteotomy should be performed at a different level than the tibial osteotomy to avoid creating a single plane of severe instability and to reduce the risk of cross union. Typically, a mid shaft or distal third fibular osteotomy is preferred. Resecting a small 1 centimeter segment of the fibula ensures that the bone ends do not impinge during the rotational correction of the tibia.
Complications and Pitfalls in Torsional Correction
Despite meticulous planning, rotational deformity correction carries significant risks. The surgeon must be prepared to anticipate and manage these complications to ensure a successful outcome.
Neurological Injury and Nerve Palsy
The most feared complication during tibial derotation, particularly internal rotation of the distal segment, is injury to the common peroneal nerve. As the distal tibia and fibula are rotated internally, the soft tissue envelope, including the peroneal nerve as it wraps around the fibular neck, is placed under immense tension.
- Surgical Pearl: Prophylactic peroneal nerve decompression should be strongly considered for any tibial internal rotation correction exceeding 15 degrees. The surgeon must release the superficial fascia of the lateral compartment and the fibrous arch of the peroneus longus to allow the nerve to glide freely during the correction.
Compartment Syndrome
Acute compartment syndrome is a devastating complication that can occur following both femoral and tibial osteotomies. The trauma of the osteotomy, combined with the volumetric changes in the muscular compartments caused by rotating the bone, significantly increases intracompartmental pressures. Continuous clinical monitoring of the extremity is mandatory. If the surgeon utilizes an intramedullary nail for fixation, the reaming process further increases the risk. Any signs of disproportionate pain or pain with passive stretch must be met with an immediate four compartment fasciotomy.
Iatrogenic Mechanical Axis Deviation
As thoroughly discussed, iatrogenic Mechanical Axis Deviation is the hallmark of a poorly planned femoral osteotomy. If a surgeon realizes postoperatively that they have induced a varus or valgus deformity by rotating around the anatomic axis of the femur, revision surgery is often required. This underscores the absolute necessity of preoperative templating, understanding Paleys axis rules, and utilizing intraoperative fluoroscopy to verify mechanical alignment before final fixation is applied.
Summary of Key Takeaways for the Orthopedic Surgeon
Mastering rotational deformities requires a transition from two-dimensional radiographic thinking to three-dimensional spatial execution. By adhering to the principles established by Dr Dror Paley, surgeons can consistently achieve excellent clinical outcomes.
- Clinical Assessment is Paramount: Never rely solely on the foot progression angle. A complete torsional profile, including hip rotation and the thigh foot angle, is mandatory to isolate the level of the deformity.
- Respect the Axes: The tibia is forgiving because the anatomic and mechanical axes are collinear. The femur is dangerous because of the 7 degree divergence between these axes.
- The Distal Femur is the Safe Zone: Always attempt to perform pure femoral derotations in the distal metaphysis where the mechanical and anatomic axes intersect, avoiding iatrogenic Mechanical Axis Deviation.
- Utilize Reference Wires: Intraoperative visual estimation of rotation is notoriously inaccurate. Always use proximal and distal reference K-wires inserted at the exact planned angle of correction before making the osteotomy cut.
- Protect the Soft Tissues: Concomitant fibular osteotomies are required for tibial derotation, and prophylactic peroneal nerve release must be considered for large magnitude internal tibial rotations.
By internalizing these biomechanical concepts and surgical techniques, the orthopedic surgeon can confidently approach even the most complex torsional malalignments, restoring normal kinematics and improving the long term joint health of their patients.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like