Precision Osteotomy: Correcting Complex Angulation-Translation Deformities
Key Takeaway
Angulation-translation deformity correction involves understanding the a-t CORA and applying Paley's osteotomy rules. Surgeons choose between osteotomy at the a-t CORA for biological safety or at the malunion site for cosmetic and intramedullary nailing compatibility, aiming to restore mechanical axis and function.
Introduction to Complex Malunions and the Angulation Translation Paradigm
In the realm of orthopedic deformity correction, pure angular deformities or pure translational deformities are relatively straightforward to conceptualize and treat. However, the clinical reality is rarely so forgiving. Most post-traumatic malunions and congenital anomalies present as a combination of both angulation and translation, often spanning multiple anatomical planes. For the orthopedic surgeon in training, mastering angulation translation deformity correction is the gateway to advanced limb reconstruction.
Relying on the foundational principles established by Dr. Dror Paley, this comprehensive guide will dissect the biomechanics, preoperative planning, and surgical execution of osteotomies designed to tackle these complex, multi-dimensional challenges. Whether you are dealing with a diaphyseal malunion of the tibia or a complex femoral deformity, understanding the relationship between the Center of Rotation of Angulation, the mechanical axis deviation, and the anatomical axes is paramount.
When a bone heals with both an angular and a translational offset, the mechanical axis of the limb is displaced. This displacement leads to abnormal joint reactive forces, premature osteoarthritis, and significant functional impairment. Correcting these deformities requires a deep understanding of the angulation translation CORA and the strategic decision-making process regarding exactly where to make the bone cut.
Core Biomechanical Principles Defining the Angulation Translation CORA
Before delving into surgical strategies, the orthopedic surgeon must establish the geometric foundation of the deformity.
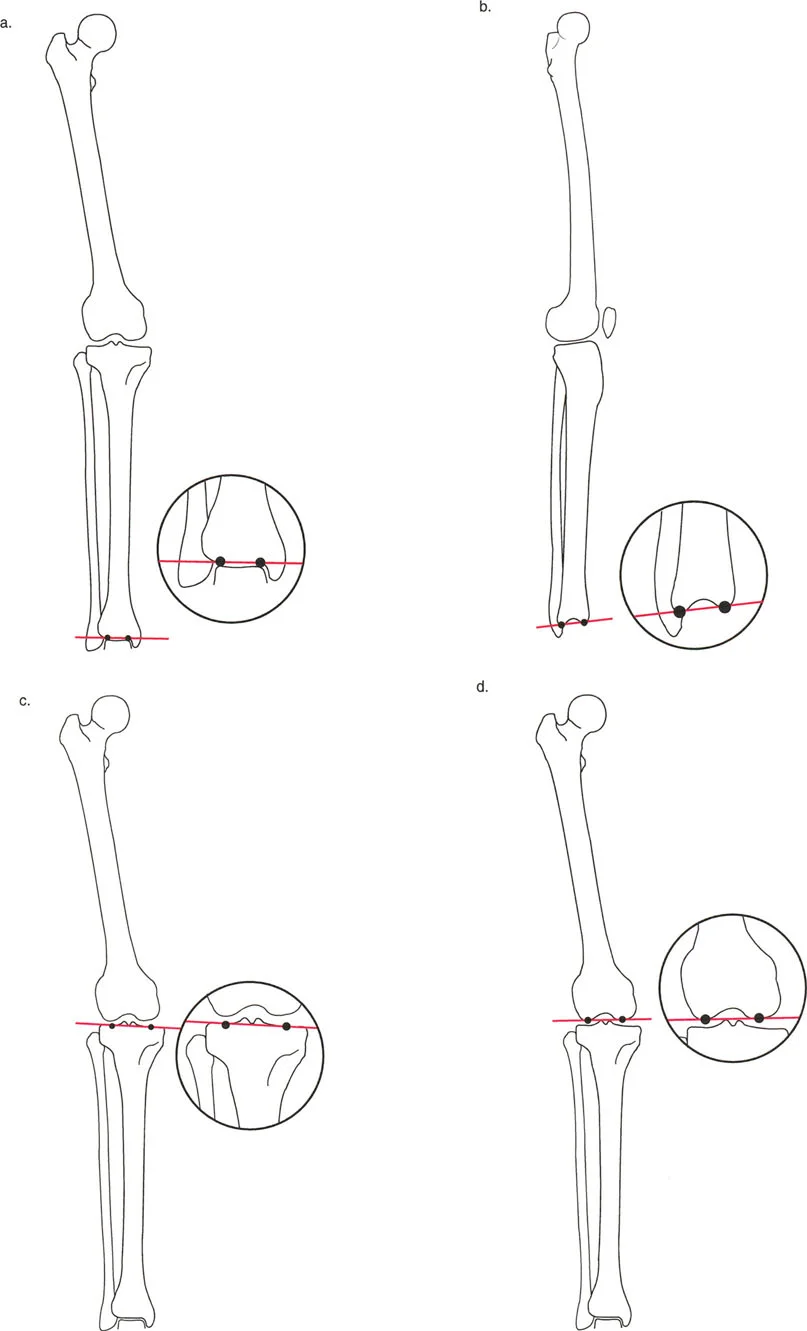
In a pure angular deformity, the proximal and distal anatomical axes intersect precisely at the apex of the deformity, forming the standard Center of Rotation of Angulation. However, when translation is introduced into the system, the anatomical axes no longer intersect at the site of the original fracture or pathology. Because the distal segment is shifted relative to the proximal segment, the lines of the axes are offset.
If you extend the proximal anatomical axis distally, and the distal anatomical axis proximally, they will eventually cross at a distinct point in space. This intersection point is known as the angulation translation Center of Rotation of Angulation or the a-t CORA.
Understanding the location of the a-t CORA is the linchpin of deformity planning because it dictates the geometric rules of correction. The spatial relationship between the osteotomy site, the hinge point, and the a-t CORA will determine whether the final limb alignment is perfectly restored or inadvertently worsened.
The Concept of Mechanical Axis Deviation
The Mechanical Axis Deviation is the absolute distance between the mechanical axis of the lower extremity and the center of the knee joint. In a normal lower limb, a line drawn from the center of the femoral head to the center of the ankle joint should pass slightly medial to the center of the knee, typically by about eight millimeters.
When an angulation translation malunion occurs, the Mechanical Axis Deviation shifts dramatically. A varus deformity shifts the mechanical axis medially, overloading the medial compartment of the knee. A valgus deformity shifts the axis laterally, overloading the lateral compartment. The primary goal of any osteotomy strategy is to restore the Mechanical Axis Deviation to a neutral, physiologic baseline, thereby normalizing joint reactive forces and preserving the articular cartilage.
Joint Orientation Angles in Deformity Planning
To accurately locate the a-t CORA and plan the correction, the surgeon must be fluent in the standard joint orientation angles. These angles define the relationship between the mechanical or anatomical axes of the long bones and the joint lines of the hip, knee, and ankle. Dr. Paley's nomenclature is the universal standard for these measurements.
| Angle Acronym | Full Definition | Normal Physiologic Range |
|---|---|---|
| mLDFA | Mechanical Lateral Distal Femoral Angle | 85 to 90 degrees |
| MPTA | Medial Proximal Tibial Angle | 85 to 90 degrees |
| JLCA | Joint Line Convergence Angle | 0 to 2 degrees |
| mLPFA | Mechanical Lateral Proximal Femoral Angle | 85 to 95 degrees |
| LDTA | Lateral Distal Tibial Angle | 88 to 92 degrees |
By drawing the normal joint orientation angles on the preoperative radiographs, the surgeon can reconstruct the ideal proximal and distal mechanical and anatomical axes. The intersection of these reconstructed axes reveals the true magnitude and location of the deformity.
Paley Osteotomy Rules for Deformity Correction
Dr. Paley outlined three fundamental rules of osteotomy that govern the relationship between the bone cut, the corrective hinge, and the CORA. Mastering these rules is non-negotiable for any surgeon attempting complex limb reconstruction.
Osteotomy Rule One
When the osteotomy and the corrective hinge are both placed exactly at the CORA, the deformity is corrected by pure angulation. The bone ends will simply rotate around the hinge point, and the proximal and distal mechanical axes will perfectly align. There is no unintended translation created by this maneuver.
Osteotomy Rule Two
When the osteotomy is placed at a different level than the CORA, but the corrective hinge remains at the CORA, the mechanical axis will still be perfectly restored. However, the bone ends at the osteotomy site will undergo a combination of angulation and translation. The bone ends will slide past each other. This is a critical concept when dealing with angulation translation deformities, as it allows the surgeon to correct the deformity while choosing an osteotomy site that is biologically or mechanically advantageous.
Osteotomy Rule Three
When the osteotomy and the corrective hinge are both placed away from the CORA, a new translational deformity is created. The mechanical axis will not be restored, and a secondary "zig-zag" deformity will be introduced into the limb. Rule Three is generally considered a surgical error unless it is intentionally utilized to compensate for a multi-apical deformity or joint line obliquity.
Deformities in the Same Plane Two Competing Strategies
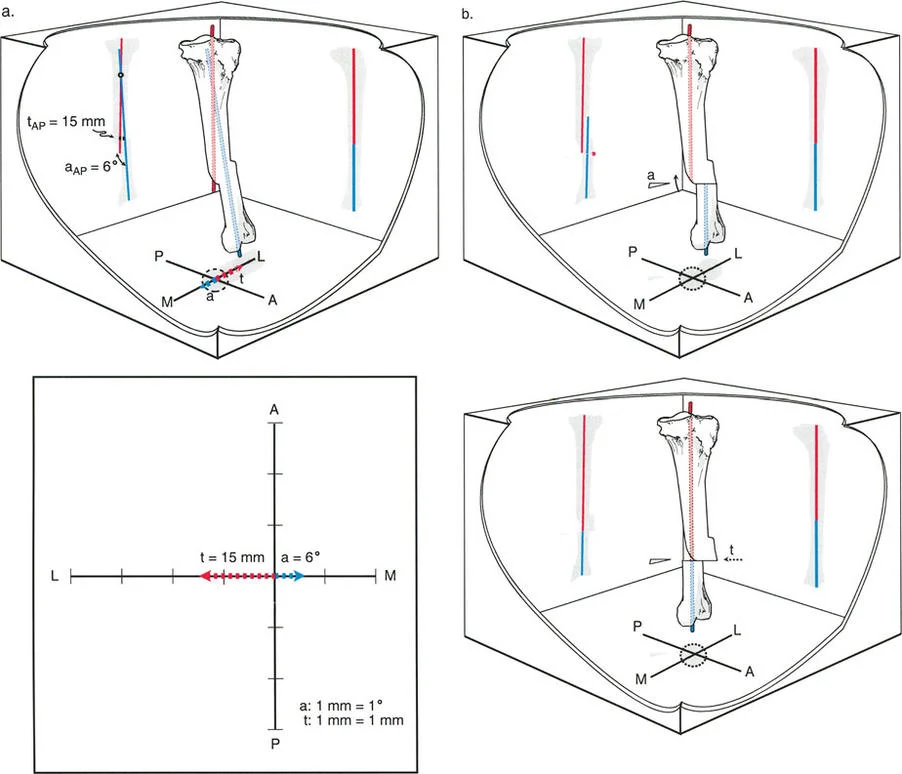
When the angulation and the translation occur entirely within the same anatomical plane, such as being visible and measurable purely on the anteroposterior radiograph or purely on the lateral radiograph, the surgeon has two distinct, competing strategies for osteotomy correction. Each strategy carries profound biological, biomechanical, and cosmetic implications.
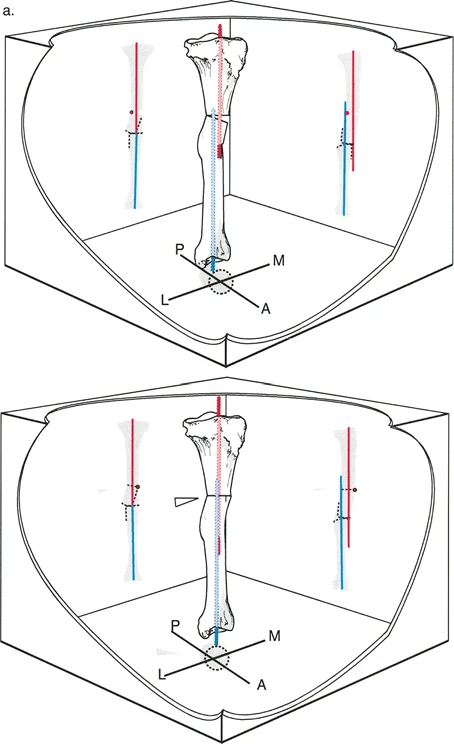
Strategy A Osteotomy at the Angulation Translation CORA
The first strategy involves ignoring the original malunion site and performing the osteotomy precisely at the a-t CORA.
Because the a-t CORA is the exact mathematical intersection of the displaced axes, performing a closing wedge, opening wedge, or neutral focal dome osteotomy at this level allows for the simultaneous correction of both the angular and translational components with a single bone cut. You simply hinge the bone around this point, relying on Osteotomy Rule One, and the mechanical axis is instantly restored.
The most significant advantage of this strategy is biological safety. The a-t CORA frequently falls in a region of the diaphysis or metaphysis that is completely separate from the original fracture site.
The bone at a previous fracture level is notoriously treacherous. It is often highly sclerotic, hypovascular, and may harbor dormant bacteria if the original injury was an open fracture. Furthermore, the soft tissues overlying a previous trauma site are frequently scarred, adherent to the bone, and compromised in their vascularity. By moving the osteotomy to the a-t CORA, the surgeon operates through pristine, uninjured skin and muscle, drastically reducing the risk of wound breakdown and deep infection.
Additionally, the a-t CORA level usually features a patent, normal medullary canal, facilitating robust endosteal healing and the generation of high-quality regenerate bone if gradual correction via distraction osteogenesis is employed.
Despite its biological safety, the a-t CORA strategy has two major drawbacks that often deter surgeons. First is the residual cosmetic bump. Because the original malunion site is left untouched, the physical step-off of the malunited bone remains. In areas with thick muscle coverage, this is irrelevant. However, on the subcutaneous medial border of the tibia, this residual bump can be highly symptomatic, aesthetically displeasing, and prone to irritation from footwear.
Second is the incompatibility with intramedullary nailing. An osteotomy at the a-t CORA creates a new angular bend in the bone to compensate for the old one. This results in a zig-zag deformity of the medullary canal. Passing a straight, rigid intramedullary nail through a zig-zag canal is mechanically impossible without excessive reaming that compromises cortical integrity. Therefore, Strategy A typically requires fixation with plates and screws or an external fixator.
Strategy B Osteotomy at the Original Malunion Site
The second strategy directly addresses the primary pathology by placing the osteotomy at the exact site of the original fracture malunion, which is the apex of the physical deformity.
Because the osteotomy is placed away from the a-t CORA, the surgeon must rely on Paley's Osteotomy Rule Two. To restore the mechanical axis, the hinge of correction must remain virtually located at the a-t CORA, while the bone cut is made at the malunion site. As the deformity is corrected around the a-t CORA hinge, the bone ends at the malunion site will undergo simultaneous angulation and translation.
The biomechanical brilliance of Strategy B is that it completely abolishes the zig-zag deformity of the bone. By correcting the angulation and translation directly at the site where they originated, the medullary canal is perfectly reconstituted into a straight tube. This straight canal allows for the immediate insertion of a rigid, locked intramedullary nail. Intramedullary nailing offers superior load-sharing biomechanics, allows for early weight-bearing, and avoids the soft tissue irritation associated with bulky external fixators or large plates.
Furthermore, Strategy B eliminates the cosmetic bump. The translation of the bone ends at the osteotomy site smooths out the cortical step-off, resulting in a cosmetically normal-appearing limb.
However, Strategy B carries substantial biological risks. The surgeon must operate directly through the zone of injury. Cutting through dense, avascular, sclerotic bone requires high-energy tools like oscillating saws or drill bits, which can cause thermal necrosis. Healing at this site is notoriously slow, and the risk of nonunion is significantly elevated compared to cutting through pristine metaphyseal bone. The soft tissue envelope is also at higher risk of dehiscence and infection due to prior scarring.
Preoperative Planning Steps for Angulation Translation Deformities
Meticulous preoperative planning is the hallmark of a successful deformity correction. The surgeon must transition from conceptual understanding to precise geometric mapping before stepping into the operating room.
Step One Obtaining Proper Radiographs
Accurate planning begins with high-quality, full-length, weight-bearing radiographs of the lower extremities. The patella must be facing perfectly forward to ensure a true anteroposterior view. A true lateral view spanning the hip, knee, and ankle is equally critical. Standard short-cassette radiographs are insufficient for deformity planning because they do not allow for the assessment of the mechanical axis or the standard joint orientation angles.
Step Two Drawing the Mechanical Axes
The surgeon draws the mechanical axis of the normal, contralateral limb to establish the baseline Mechanical Axis Deviation. On the deformed limb, the center of the femoral head, the center of the knee, and the center of the ankle are identified. The proximal and distal mechanical axes are drawn based on the normal joint orientation angles.
Step Three Locating the Angulation Translation CORA
By extending the proximal and distal anatomical axes, the surgeon identifies their intersection point. This is the a-t CORA. The magnitude of the angular deformity is measured at this intersection. The magnitude of the translational deformity is measured as the perpendicular distance between the parallel offset axes at the level of the malunion.
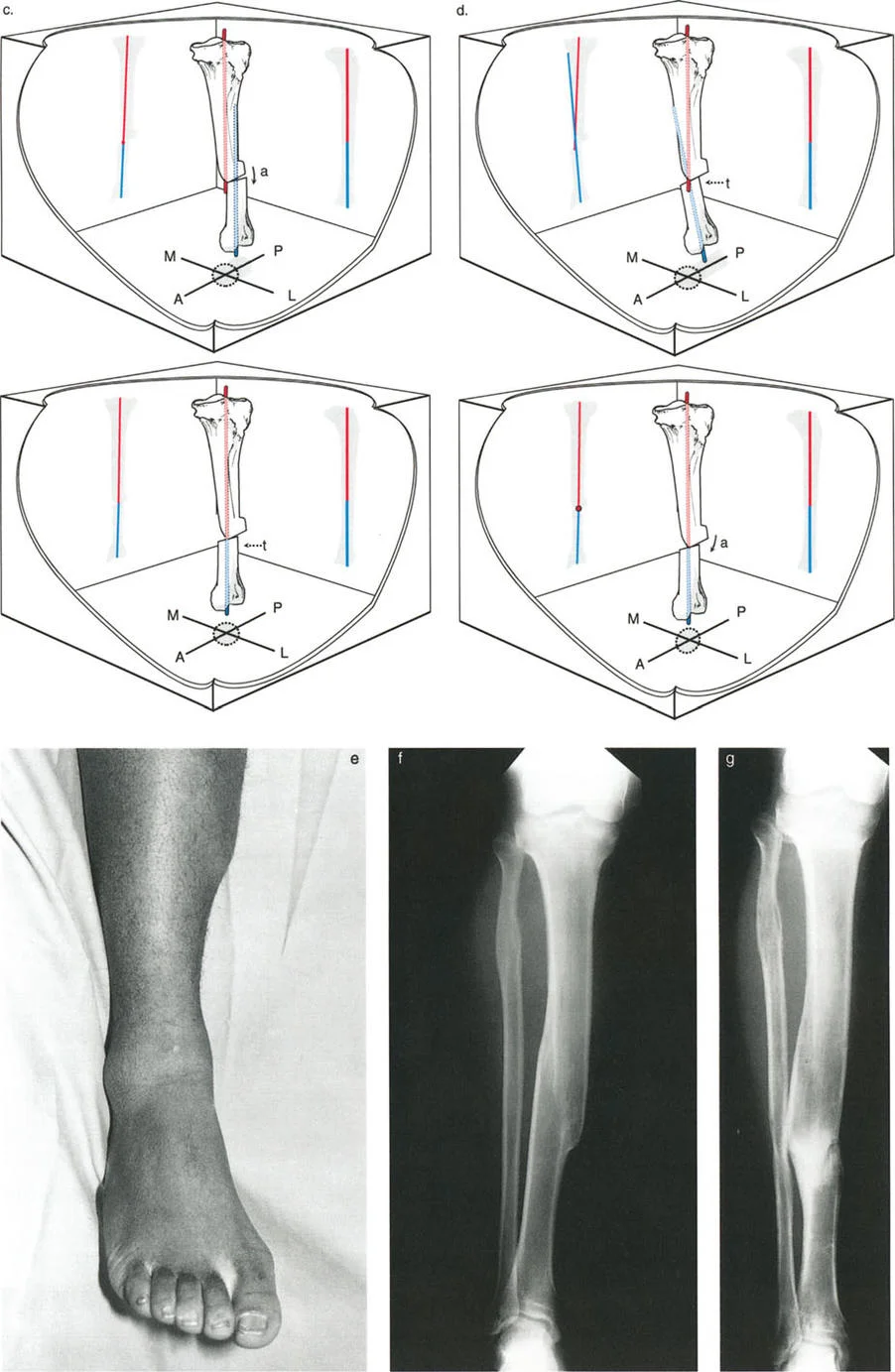
Step Four Simulating the Osteotomy
Using digital templating software or traditional paper cut-outs, the surgeon simulates both Strategy A and Strategy B.
If simulating Strategy A, the cut is made at the a-t CORA, and the distal segment is rotated until the mechanical axes align. The surgeon evaluates the resulting zig-zag deformity and plans for plate or external fixator placement.
If simulating Strategy B, the cut is made at the malunion site. The distal segment is rotated and translated until the medullary canal is straight and the mechanical axes align. The surgeon measures the exact amount of translation required in millimeters to ensure the chosen hardware can accommodate the shift.
Biological and Biomechanical Considerations in Osteotomy Placement
The decision between cutting at the a-t CORA or the malunion site is rarely purely geometric. The orthopedic surgeon must balance the biomechanical desire for a straight medullary canal against the biological reality of bone healing and soft tissue viability.
Managing the Soft Tissue Envelope and Zone of Injury
The soft tissue envelope dictates the surgical approach. In patients with severe post-traumatic scarring, skin grafting, or prior flap coverage over the malunion site, Strategy B may be contraindicated. Incising through compromised tissue to perform a complex osteotomy with translation severely increases the risk of deep infection and hardware exposure. In these scenarios, Strategy A is preferred, utilizing an Ilizarov or Taylor Spatial Frame applied percutaneously away from the zone of injury.
Conversely, if the soft tissue envelope is robust and pliable, Strategy B becomes much more attractive. The surgeon can utilize an extensile approach, excise the sclerotic bone, perform the necessary angulation and translation, and achieve stable internal fixation.
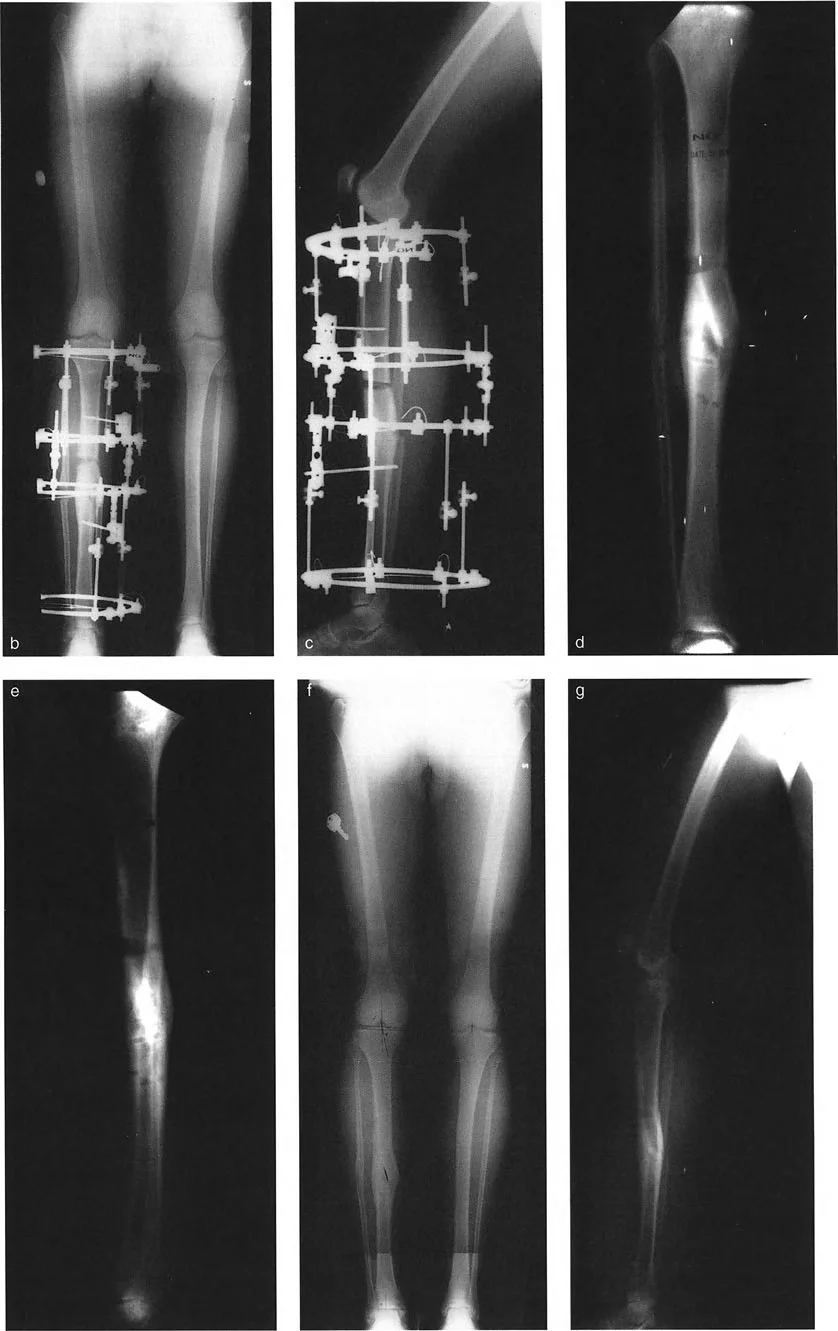
Intramedullary Nailing Versus External Fixation
The choice of osteotomy strategy heavily influences the choice of fixation hardware.
Intramedullary nailing is the gold standard for diaphyseal fractures and osteotomies due to its load-sharing properties and minimal disruption of the periosteal blood supply. However, as established, nailing requires a straight medullary canal, necessitating Strategy B. When performing Strategy B with an intramedullary nail, the surgeon often uses blocking screws, also known as Poller screws, to guide the nail and maintain the corrected translation and angulation during insertion.
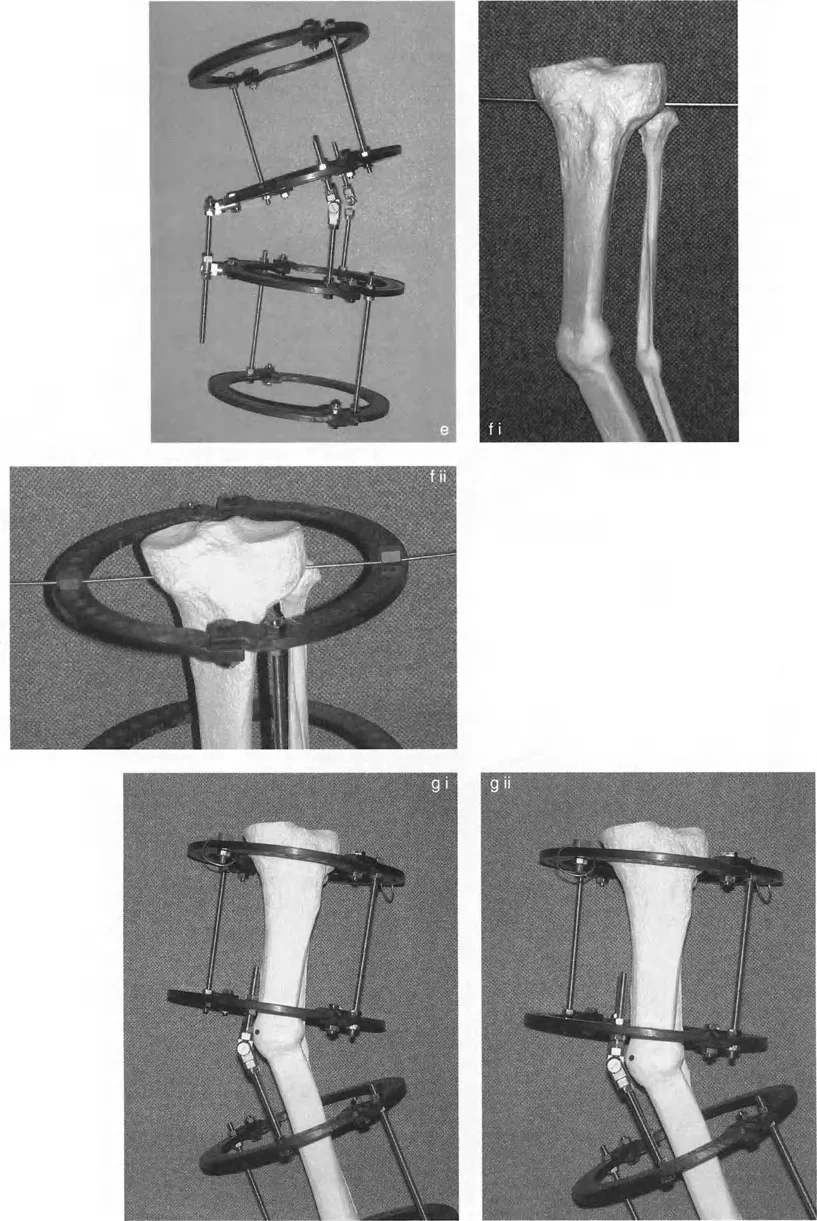
External fixation, particularly hexapod circular frames like the Taylor Spatial Frame, excels in complex, multi-planar angulation translation deformities. Hexapod frames do not require a straight medullary canal. They allow the surgeon to perform the osteotomy at the biologically optimal a-t CORA (Strategy A) and gradually correct the deformity over weeks using a computer-generated schedule. Gradual correction via distraction osteogenesis minimizes the risk of acute neurovascular stretch injuries, which is a significant concern when acutely translating bone ends in Strategy B.
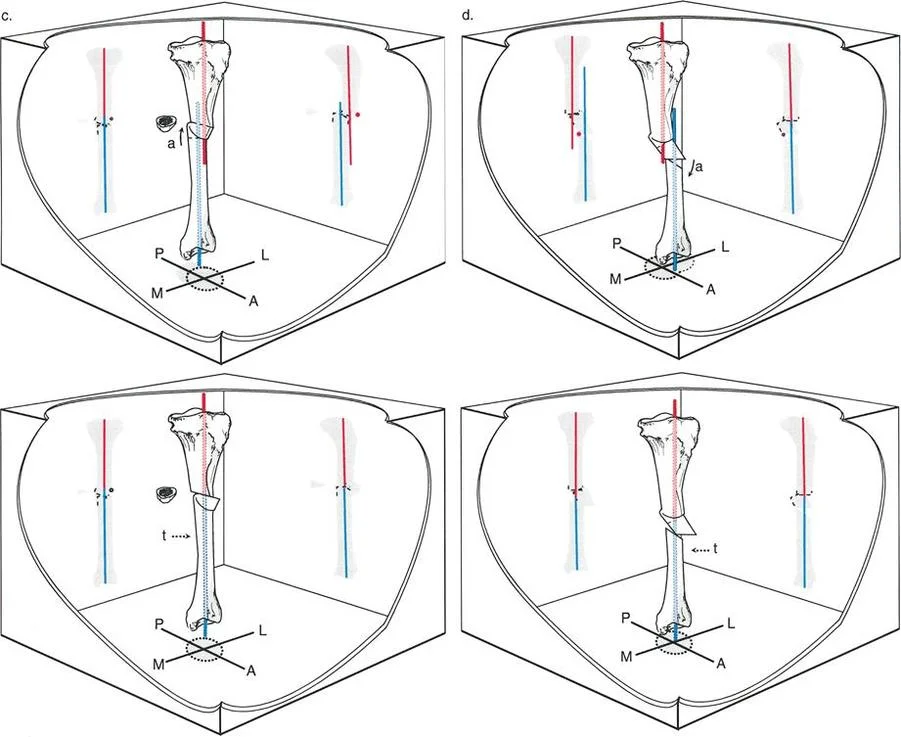
Multi Planar Deformities and the Oblique Plane
While the preceding sections focused on deformities in a single plane, true angulation translation malunions often exist in both the coronal and sagittal planes simultaneously.
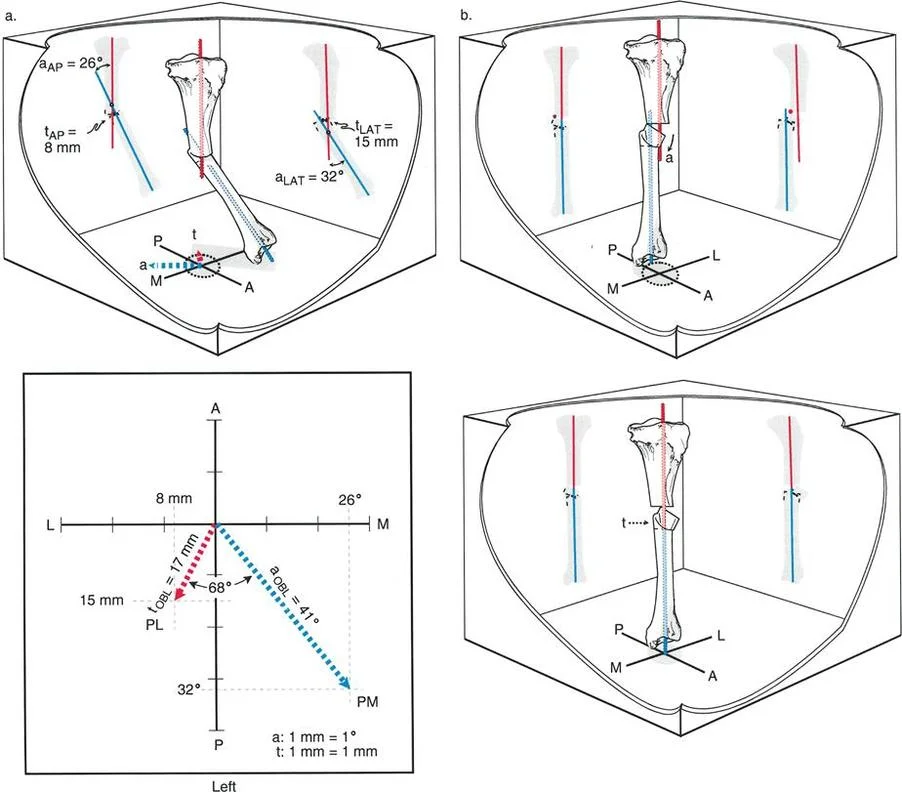
When a bone is angulated and translated in both the anteroposterior and lateral views, the deformity actually exists in a single, distinct oblique plane. The surgeon must calculate the true magnitude of the deformity and the orientation of this oblique plane using trigonometric principles or specialized software.
The a-t CORA in a multi-planar deformity is found by analyzing the intersection of the axes in this oblique plane. Correcting the deformity requires rotating the bone around a hinge that is perpendicular to the oblique plane. Hexapod external fixators have revolutionized the management of oblique plane deformities, as the software matrix automatically calculates the simultaneous multi-planar correction, simplifying a mathematically overwhelming task for the surgeon.
Clinical Pearls for the Orthopedic Surgeon
To synthesize the complexities of angulation translation deformity correction, surgeons should integrate the following high-yield pearls into their clinical practice.
- Never Trust a Short Cassette: Always demand full-length, weight-bearing standing radiographs. You cannot accurately assess the Mechanical Axis Deviation or locate the true a-t CORA without visualizing the hip, knee, and ankle joints simultaneously.
- Respect the Biology of the Malunion: Sclerotic bone at a previous fracture site has a high rate of nonunion. If you choose Strategy B, consider decorticating the bone ends, using a high-speed burr with copious irrigation to prevent thermal necrosis, and adding autologous bone graft to stimulate osteogenesis.
- Master the Poller Screw: When utilizing Strategy B with an intramedullary nail, blocking screws are essential. Place the blocking screws in the concavity of the deformity to narrow the medullary canal and force the nail to translate the bone ends into the correct anatomical alignment.
- Beware the Neurovascular Bundle: Acute translation of bone ends, as required in Strategy B, can tether or stretch adjacent nerves and vessels. For example, acute valgus and translational correction of a proximal tibia deformity can easily cause a common peroneal nerve palsy. If significant translation is required, consider gradual correction with a circular frame or a prophylactic nerve release.
- Understand the Limits of Acute Correction: As a general rule, acute translation greater than one centimeter or acute angulation greater than fifteen degrees carries a higher risk of soft tissue complications. Gradual distraction osteogenesis is preferred for massive deformities.
- The Rule of Thumb for Hinge Placement: Remember Paley's Rule Two. If you want the bone ends to slide and translate, put your osteotomy away from the a-t CORA, but keep your conceptual hinge exactly on the a-t CORA.
Conclusion to Angulation Translation Deformity Correction
Mastering the angulation translation paradigm elevates the orthopedic surgeon from a mere bone-setter to a true architect of limb reconstruction. Deformities are rarely simple, and the interplay between angular deviation and translational shift requires a rigorous, mathematical approach to preoperative planning.
By deeply understanding Dr. Dror Paley's principles, specifically the identification of the a-t CORA and the application of the three Osteotomy Rules, surgeons can predictably restore the mechanical axis of the lower extremity. The choice between cutting at the a-t CORA to prioritize biology, or cutting at the malunion site to prioritize biomechanics and intramedullary nailing, remains one of the most intellectually stimulating challenges in orthopedic surgery.
Ultimately, successful deformity correction relies on a delicate balance. The surgeon must harmonize the geometric perfection of the anatomical axes with the biological realities of bone healing and soft tissue viability. Through meticulous planning, respect for joint orientation angles, and precise surgical execution, even the most complex angulation translation malunions can be corrected, restoring function, alleviating pain, and preserving the long-term health of the patient's joints.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like