Mastering Complex Deformity Correction: Paley's Principles for Translation & Angulation
Key Takeaway
Translation deformities involve parallel but non-collinear bone axes, while angulation-translation combines both. Dr. Paley's method uses precise biomechanical principles, CORA, and specialized osteotomies (transverse or oblique) to restore mechanical axis alignment, ensuring optimal bone-to-bone contact and preventing iatrogenic deformities in limb reconstruction.
Introduction to Complex Deformity Correction
In the realm of orthopedic deformity correction, pure angular deformities often dominate the early learning curve of surgeons-in-training. However, real-world trauma, malunions, and nonunions rarely present in a single, simple plane. Long bone deformities are frequently a complex amalgamation of rotation, length discrepancies, and shifting axes. Among the most challenging of these geometric puzzles are pure translation deformities and combined angulation-translation deformities.
Mastering these deformities requires a rigorous understanding of biomechanics, spatial geometry, and the foundational principles established by Dr. Dror Paley. This comprehensive masterclass will dissect the nuances of translation, the rules governing osteotomy placement, the critical importance of bone-to-bone contact, and the standardized conventions required to accurately measure and correct these multi-planar challenges. Whether you are utilizing acute internal fixation or gradual distraction osteogenesis via a hexapod circular fixator, the principles outlined in this guide are the bedrock of successful limb reconstruction.
The Evolution of Limb Reconstruction
Historically, limb reconstruction relied heavily on visual estimation and rudimentary osteotomies that often failed to restore the true mechanical axis of the lower extremity. The advent of the Paley method revolutionized this field by introducing a strict mathematical and geometric approach to bone deformity. By treating the long bones as geometric line segments and the joints as precise angular orientations, orthopedic surgeons can now predict the exact biomechanical outcome of an osteotomy before the first incision is ever made.
Paley Principles as the Foundation
To navigate translation and angulation-translation deformities, the surgeon must be fluent in the language of Paley. The Center of Rotation of Angulation (CORA), Mechanical Axis Deviation (MAD), and Joint Orientation Angles are not merely academic concepts; they are the navigational beacons of surgical planning. A failure to respect these principles inevitably leads to iatrogenic deformities, joint malorientation, and early failure of the reconstructed limb.
Biomechanics of Pure Translation Deformities
A pure translation deformity occurs when the proximal and distal anatomical or mechanical axis lines of a bone are perfectly parallel but not collinear. Understanding the biomechanical implications of this displacement is the first step in formulating a corrective surgical plan.
Defining Translation in the Frontal and Sagittal Planes
Translation can occur in any plane, but it is most frequently analyzed in the frontal (coronal) and sagittal planes. In the frontal plane, medial or lateral translation shifts the mechanical axis away from the center of the knee joint. In the sagittal plane, anterior or posterior translation alters the lever arm of the extensor or flexor mechanisms, profoundly impacting gait kinematics.
Center of Rotation of Angulation at Infinity
In Paley's terminology, the Center of Rotation of Angulation (CORA) is the point at which the proximal and distal axes of a deformed bone intersect. However, in a pure translation deformity, the proximal and distal axes are parallel. In geometric terms, parallel lines never intersect, meaning the CORA for a pure translation deformity is mathematically located at infinity.
Because there is no angular deviation, the joint orientation angles remain completely normal relative to their respective local bone segments. The joint surfaces remain parallel to the ground during the stance phase of gait, provided there is no compensatory joint contracture.
Mechanical Axis Deviation and Clinical Consequences
Do not mistake a lack of angulation for a lack of clinical consequence. Pure translation shifts the overarching mechanical axis of the entire limb, resulting in Mechanical Axis Deviation (MAD).
When the femur or tibia translates medially or laterally, the mechanical axis line drawn from the center of the femoral head to the center of the ankle joint no longer passes through the center of the knee. This displacement alters the weight-bearing forces across the adjacent joints. A lateral translation of the distal tibial segment, for example, will shift the mechanical axis laterally, inducing a valgus thrust at the knee. Over time, this abnormal load distribution predisposes the patient to asymmetric cartilage wear, ligamentous strain, and early-onset osteoarthritis.
Joint Orientation Angles in Pure Translation
To confirm a pure translation deformity, the surgeon must measure the joint orientation angles. In a pure translation scenario, these angles will fall within normal population parameters.
| Joint Orientation Angle | Abbreviation | Normal Range | Average |
|---|---|---|---|
| Mechanical Lateral Distal Femoral Angle | mLDFA | 85 to 90 degrees | 88 degrees |
| Medial Proximal Tibial Angle | MPTA | 85 to 90 degrees | 87 degrees |
| Mechanical Lateral Proximal Femoral Angle | mLPFA | 85 to 90 degrees | 90 degrees |
| Lateral Distal Tibial Angle | LDTA | 86 to 92 degrees | 89 degrees |
| Joint Line Congruency Angle | JLCA | 0 to 2 degrees | 0 degrees |
Clinical Pearl: If the mLDFA or MPTA falls outside these normal ranges, you are no longer dealing with a pure translation deformity. You are facing a combined angulation-translation deformity, which requires a completely different set of osteotomy rules.
Preoperative Planning for Translation Deformities
Correcting translation without inducing an iatrogenic angular deformity requires precise osteotomy planning. The primary limiting factor in translating a bone back to its anatomic axis is the preservation of adequate bone-to-bone contact to ensure biomechanical stability and biological healing.
Step by Step Radiographic Evaluation
- Obtain full-length, standing, weight-bearing anteroposterior (AP) and lateral radiographs of the entire lower extremity.
- Draw the mechanical axis of the entire limb from the center of the femoral head to the center of the ankle plafond.
- Measure the Mechanical Axis Deviation (MAD) in millimeters from the center of the knee joint.
- Draw the proximal and distal anatomical axes of the deformed bone.
- Confirm that the axes are parallel.
- Measure the exact magnitude of translation in millimeters between the parallel axes.
Calculating the Required Translation
The magnitude of translation measured on the radiograph dictates the surgical correction required. However, the surgeon must account for radiographic magnification. Utilizing a calibration marker (such as a 25 mm sphere placed at the level of the bone during the X-ray) is mandatory to calculate the true translation distance.
Osteotomy Selection for Translation Deformities
When addressing a translation deformity without angulation, the surgeon must choose an osteotomy trajectory that allows the bone segments to slide back into alignment while respecting the biological envelope. The choice between a transverse and an oblique osteotomy is dictated by the patient's need for simultaneous limb lengthening and the anatomical level of the deformity.
The Transverse Osteotomy
The transverse osteotomy is the workhorse for pure translational correction when there is no need to add length to the limb. By cutting perpendicular to the bone axis, the surgeon creates two flat surfaces that can slide across one another.
Maximizing Bone Contact in Transverse Cuts
The level at which this cut is performed is of paramount importance. It is highly preferable to perform the transverse cut just proximal or distal to the region of the original bone overlap, which is the apex of the translation. By executing the cut at the metaphyseal flare or adjacent to the overlap, maximum bone contact can be maintained after the translation is completed.
If a translational osteotomy is performed at a normal-width diaphyseal level, the surgeon will face a severe geometric penalty. The diaphyseal tube is narrow; therefore, the amount of translation possible is strictly limited. As the bone ends are translated to correct the mechanical axis, the cross-sectional bone-to-bone contact decreases linearly. A 50 percent translation in a narrow diaphysis leaves only 50 percent cortical contact, severely compromising intrinsic stability and increasing the risk of nonunion or hardware failure.
Surgical Pearl: When performing a transverse osteotomy in the diaphysis, a minimum of 50 percent bone-to-bone contact must be maintained. If the required translation exceeds this limit, the surgeon must utilize an intercalary bone graft, a shortening osteotomy, or transition to a gradual correction method using distraction osteogenesis.
The Oblique Osteotomy
When a translation deformity is accompanied by limb shortening, the oblique osteotomy becomes an elegant, dual-purpose solution. An oblique cut allows the bone segments to lengthen as they translate along the inclined axis of the osteotomy line.
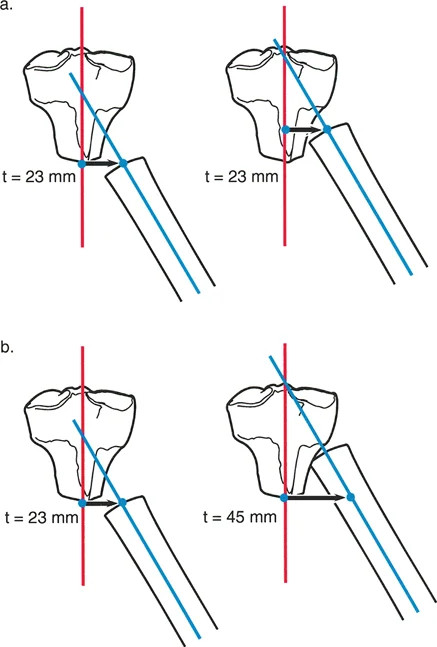
Mathematical Geometry of the Oblique Cut
The geometry of the oblique cut must be meticulously calculated. The angle of the bone cut is directly determined by two variables: the amount of length required and the amount of translation required.
For example, if a surgeon needs 20 mm of translation and 20 mm of lengthening, a 45-degree oblique cut is required. As the distal segment slides along the 45-degree plane, it moves distally (lengthening) and laterally or medially (translating) at an equal rate. If more length is needed than translation, the osteotomy angle must be more vertical (closer to the anatomical axis). If more translation is needed than length, the osteotomy angle must be more horizontal.
The limiting factors for an oblique osteotomy are twofold. First, just like the transverse cut, the surgeon must ensure adequate bone contact remains at the end of the sliding correction. Second, the soft tissue envelope dictates the amount of acute lengthening possible. Stretching neurovascular structures acutely beyond 15 to 20 millimeters can lead to neurapraxia, compartment syndrome, or vascular compromise.
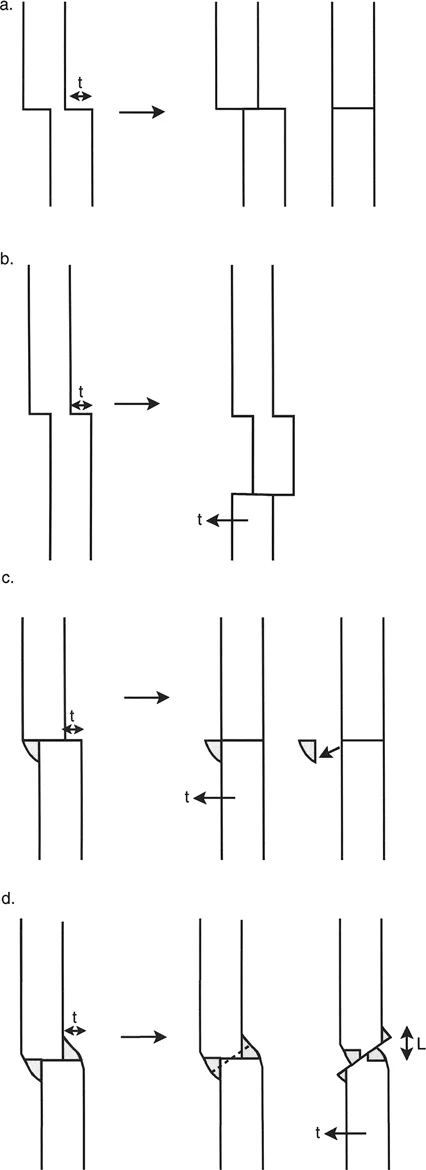
Translation osteotomies. Part of the decision regarding the level of osteotomy depends on the configuration of the bone ends and callus. L, length. (a) Transverse cut at the level of the previous fracture, no callus. (b) Transverse cut at a level different from that of the previous fracture, no callus. (c) Transverse cut at the level of the previous fracture, callus trimmed off to allow sliding. (d) Oblique cut to simultaneously regain length and translation.
Managing Callus in Mature Malunions
As illustrated in the diagram above, the presence of fracture callus complicates the osteotomy. In cases of mature malunions, a prominent callus may physically block the bone ends from sliding back into their anatomic alignment.
Biological and Mechanical Challenges of Fracture Callus
Fracture callus represents nature's attempt to bridge a biomechanically unstable environment. In a malunion, this callus becomes dense, sclerotic woven bone. While this provides structural stability to the deformed limb, it presents a significant mechanical barrier to acute translation. The callus essentially acts as a bony wedge that prevents the proximal and distal segments from achieving collinearity.
Furthermore, the biological envelope surrounding a mature malunion is often compromised. The periosteum may be thickened and scarred, and the local vascularity may be altered. Aggressive resection of the callus can strip the bone of its remaining blood supply, increasing the risk of an atrophic nonunion following the corrective osteotomy.
Techniques for Callus Resection and Sliding
To facilitate translation, the surgeon must carefully plan the management of the malunion callus. There are several techniques available depending on the morphology of the bone:
- Callus Trimming: If the osteotomy is performed exactly at the level of the old fracture, the protruding callus must be trimmed using an osteotome or high-speed burr. This creates a flat, sliding surface. Care must be taken to preserve as much vascularized periosteum as possible.
- Osteotomy Away from the Callus: As shown in the previous figures, performing a transverse osteotomy adjacent to the callus (rather than through it) can preserve the biological integrity of the old fracture site while allowing the diaphyseal segments to translate.
- Dome Osteotomy: In cases where translation and angulation coexist near the metaphysis, a dome or focal dome osteotomy can be utilized. This allows rotation around a central axis without the need to resect massive amounts of callus.
Mastering Combined Angulation Translation Deformities
While pure translation deformities present unique challenges, they are relatively rare compared to combined angulation-translation deformities. In these complex scenarios, the bone is not only shifted off its axis but is also bent. Mastering these deformities requires the strict application of Paley's Osteotomy Rules.
Defining the Angulation Translation Deformity
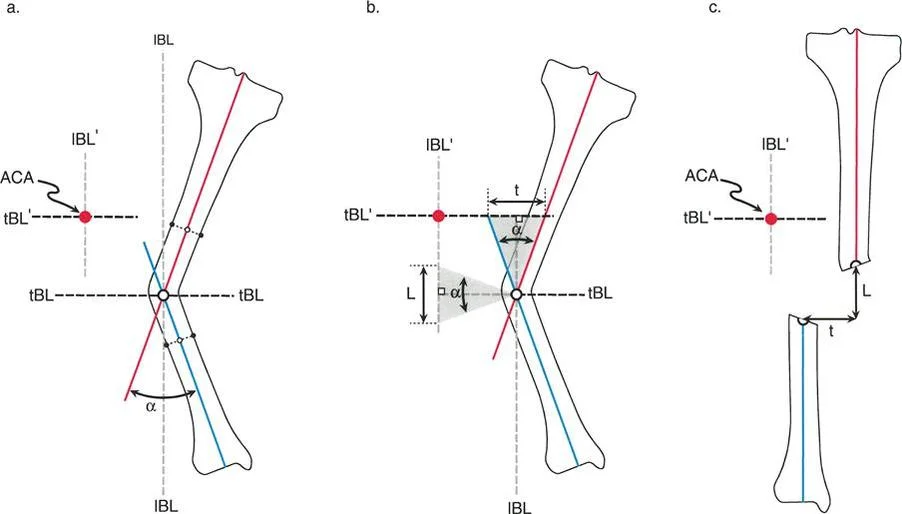
An angulation-translation deformity occurs when the proximal and distal anatomical axes intersect at a specific angle, but a pure angular correction at the apex of the deformity fails to restore the overall mechanical axis of the limb. This indicates that a translational component is "hidden" within the deformity.
The Role of the Center of Rotation of Angulation
In a combined deformity, identifying the CORA is the critical first step. The CORA is found by drawing the proximal anatomical axis and the distal anatomical axis and marking their exact point of intersection.
However, in a combined deformity, simply hinging the bone at the CORA is not enough. The surgeon must evaluate the Mechanical Axis Deviation. If a simulated angular correction at the CORA restores the joint orientation angles but leaves the limb with a residual MAD, a translational component exists and must be addressed simultaneously.
Paley Osteotomy Rules for Combined Deformities
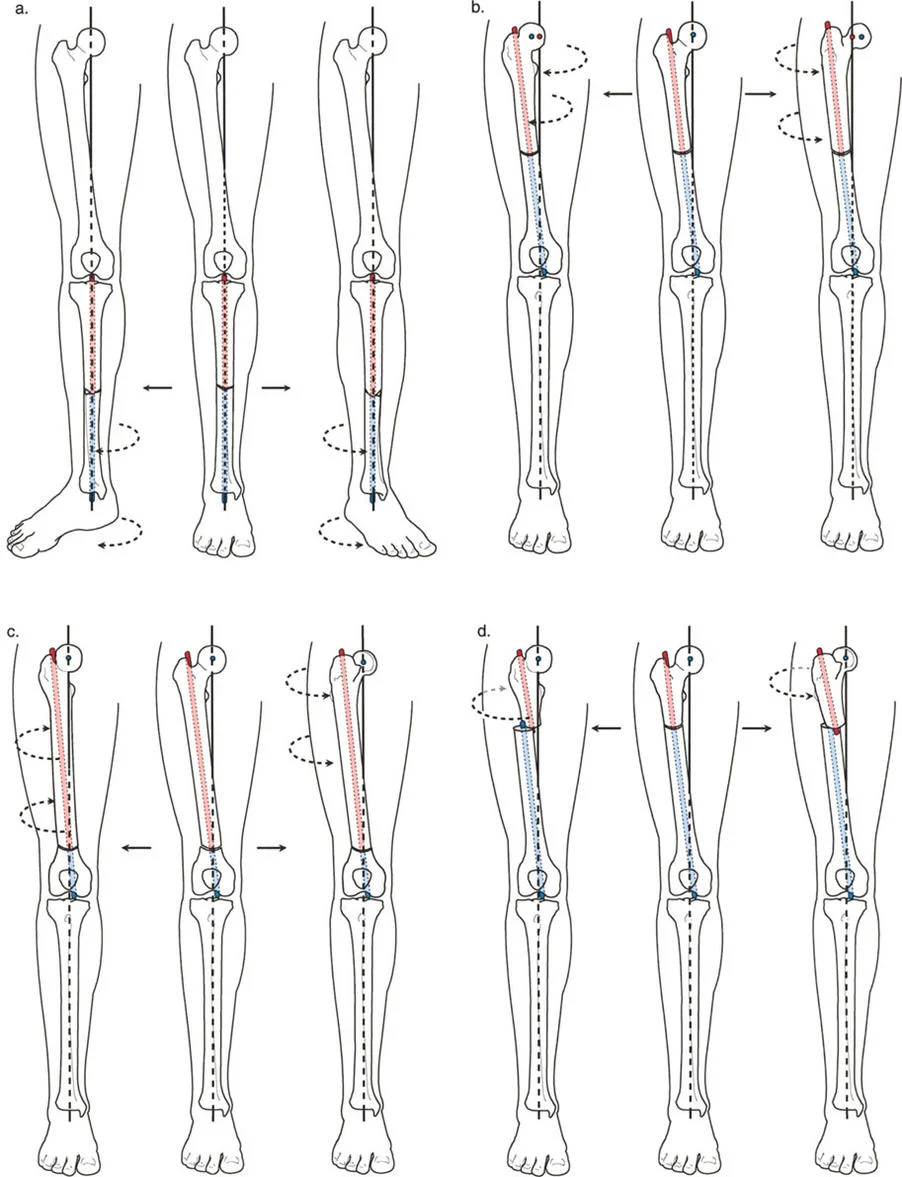
Dr. Dror Paley established three fundamental rules for osteotomy placement and correction. These rules dictate whether a bone will translate, angulate, or do both, based on the relationship between the osteotomy line, the CORA, and the hinge axis.
Rule One Osteotomy at the CORA
Paley's First Rule states that if the osteotomy and the hinge axis are both placed exactly at the CORA, the deformity will correct by pure angulation without any translation. The proximal and distal anatomical axes will become perfectly collinear.
While this is the ideal scenario for a pure angular deformity, it is insufficient for a combined angulation-translation deformity. If you apply Rule One to a combined deformity, you will correct the angulation, but the pre-existing translation will remain, leaving the patient with a residual Mechanical Axis Deviation.
Rule Two Osteotomy Outside the CORA
Paley's Second Rule states that if the osteotomy is placed at a different level than the CORA, but the hinge axis remains at the CORA, the bone will undergo both angulation and translation.
This rule is a powerful tool for correcting combined deformities. By intentionally placing the osteotomy away from the CORA, the surgeon forces the bone ends to translate as they angulate.
- Clinical Application: If a patient has a diaphyseal malunion with both varus angulation and medial translation, the CORA might be located in the metaphysis. By placing the osteotomy in the diaphysis (at the site of the malunion) and placing the fixator hinge at the metaphyseal CORA, the bone will automatically translate laterally as the varus is corrected, restoring the mechanical axis perfectly.
Rule Three Osteotomy Outside the CORA with Translation
Paley's Third Rule states that if the osteotomy and the hinge axis are both placed away from the CORA, the deformity will correct by angulation, but it will induce an iatrogenic translation. The proximal and distal axes will end up parallel but not collinear.
In the context of combined deformities, Rule Three is generally considered a pitfall to be avoided. If a surgeon inadvertently places the hinge away from the true CORA, they will create a new translation deformity. This is a common error among inexperienced surgeons utilizing external fixation, where the hinges are placed based on the soft tissue envelope rather than the geometric center of the deformity.
Key Takeaway: The hinge axis must always be aligned with the CORA to ensure the anatomical axes become collinear. If the hinge is off-axis, translation will inevitably occur.
Fixation Strategies and Postoperative Management
Once the osteotomy geometry is calculated and executed, the surgeon must choose the appropriate fixation method to stabilize the correction. The choice between acute internal fixation and gradual external fixation depends on the magnitude of the deformity, the quality of the soft tissue envelope, and the need for simultaneous limb lengthening.
Acute Correction with Internal Fixation
Acute correction followed by rigid internal fixation (using plates and screws or intramedullary nails) is highly desirable for patient comfort and early rehabilitation.
Indications for Acute Correction:
* Pure translation deformities requiring less than 15 to 20 mm of shift.
* Combined deformities where the angular correction does not severely stretch the neurovascular bundle.
* Patients with excellent skin and soft tissue compliance.
* Deformities where no limb lengthening is required.
When utilizing plates for a translation osteotomy, the surgeon must often contour the plate to accommodate the new step-off created by the metaphyseal or diaphyseal shift. Locking plates are heavily favored in these scenarios, as they function as internal external fixators and do not rely on friction between the plate and the periosteum, preserving the local blood supply.
Gradual Correction with Circular External Fixation
For severe translation deformities, or combined deformities requiring massive shifts and lengthening, gradual correction via distraction osteogenesis is the gold standard.
Indications for Gradual Correction:
* Translations exceeding 20 mm.
* Deformities accompanied by significant limb shortening requiring callotasis.
* Poor soft tissue envelopes, previous skin grafting, or active infection.
* Complex multi-planar deformities requiring six-axis spatial correction.
Modern limb reconstruction relies heavily on hexapod circular fixators, such as the Taylor Spatial Frame or OrthoSUV. These devices utilize a web-based software program to calculate the exact strut adjustments required to correct angulation, translation, rotation, and length simultaneously.
The surgeon inputs the mounting parameters (the relationship of the reference ring to the bone) and the deformity parameters (the exact magnitude of translation and angulation measured on radiographs). The software then generates a daily prescription for the patient. As the struts are adjusted, the bone segments slowly translate and angulate through the soft tissue envelope at a rate of 1 mm per day, allowing nerves and blood vessels to safely accommodate the new geometry.
Monitoring Bone Healing and Mechanical Axis
Regardless of the fixation method chosen, postoperative monitoring is critical. For acute corrections, orthogonal radiographs should be obtained at two, six, and twelve weeks to monitor for hardware failure or loss of reduction.
For gradual corrections, patients must be seen every ten to fourteen days during the distraction phase. Standing, full-length alignment radiographs are mandatory to confirm that the mechanical axis is shifting as planned. If the translation is occurring too slowly, or if an iatrogenic angulation is developing, the software parameters can be updated mid-treatment to refine the trajectory of the bone segments.
The ultimate goal of any translation or angulation-translation correction is the complete restoration of the Mechanical Axis Deviation to zero, ensuring the joints are perfectly loaded and the patient is protected from the devastating long-term consequences of malalignment. Mastering these Paley principles transforms deformity correction from a game of visual estimation into an exact, reproducible science.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like