Mastering Sagittal Plane Deformities: Orthopedic Principles of Procurvatum & Recurvatum Correction
Key Takeaway
Sagittal plane deformities, such as procurvatum and recurvatum, involve abnormal lower limb alignment. Orthopedic correction requires mastering biomechanics, compensatory kinematics, and applying precise geometric principles, like Paley's, to restore normal joint orientation and mechanical axis.
Introduction to Sagittal Plane Deformities
In the realm of orthopedic deformity correction, the frontal or coronal plane often commands the most attention. Varus and valgus deformities are visually striking, easily measured on standard anteroposterior radiographs, and intuitively linked to unilateral compartment osteoarthritis. However, sagittal plane deformities known as procurvatum and recurvatum present a uniquely complex biomechanical challenge that requires a fundamentally different analytical approach.
The core difference lies in joint kinematics. The knee does not possess a functional range of motion in the frontal plane. Therefore, there is absolutely no compensatory knee motion available to mask or accommodate a frontal plane Mechanical Axis Deviation. In stark contrast, the knee, hip, and ankle primarily move in the sagittal plane. This means that the sagittal plane alignment of the lower extremity changes dynamically with normal knee motion and the gait cycle.
While static radiographic considerations are usually sufficient for analyzing frontal plane alignment, dynamic factors must be considered when assessing sagittal plane alignment. Surgeons in training must master the interplay between bony deformity, joint contracture, and compensatory kinematics to successfully apply the principles of deformity correction pioneered by Dr Dror Paley. This comprehensive masterclass deconstructs the foundational principles of sagittal deformity correction, transforming academic concepts into an actionable, high yield framework for the operating room.
Biomechanics of Sagittal Plane Alignment
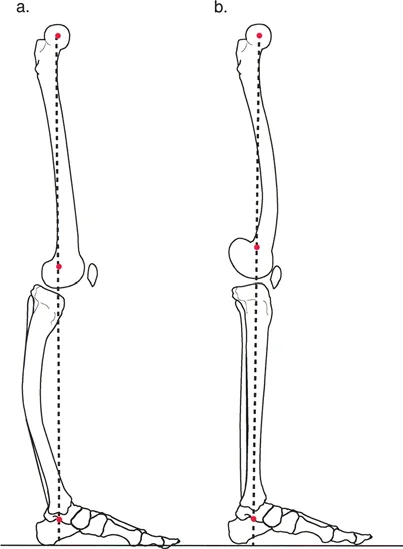
To understand sagittal plane deformities, we must first define the normal mechanical axis in this plane. The mechanical axis of the lower limb in the sagittal plane is defined by a line drawn from the center of rotation of the hip to the center of rotation of the ankle joint. On a lateral radiograph, the ankle center of rotation can be approximated as the tip of the lateral process of the talus.
The Knee Locking Mechanism
With the knee in full terminal extension, the mechanical axis of the lower limb normally passes anterior to the center of rotation of the knee joint. On a lateral radiograph, the knee center of rotation is approximated as the intersection of the posterior femoral cortex with Blumensaat line.
This anterior position of the mechanical axis is not an anatomical coincidence. It is a critical biomechanical necessity. Passing anterior to the knee center of rotation creates an extension moment, allowing the knee joint to be passively locked in full extension.
When the knee is locked in full extension, the massive quadriceps muscle group is allowed to relax during the stance phase of gait. If a sagittal plane deformity such as a severe flexion deformity prevents the mechanical axis from passing anterior to the knee, the quadriceps muscle must fire continuously to prevent the knee from buckling. This leads to profound and rapid quadriceps fatigue, resulting in an inefficient and energy draining gait pattern.
Clinical Application in Paralytic Gait
Moving the sagittal mechanical axis forward is a vital compensatory mechanism in gait for paralytic patients, such as those suffering from poliomyelitis or spina bifida. Because these patients lack the quadriceps strength to actively maintain knee extension, they rely entirely on manipulating their center of gravity to keep the mechanical axis anterior to the knee. By doing so, they use passive skeletal locking to remain upright and ambulate.
Joint Alignment During Dynamic Flexion
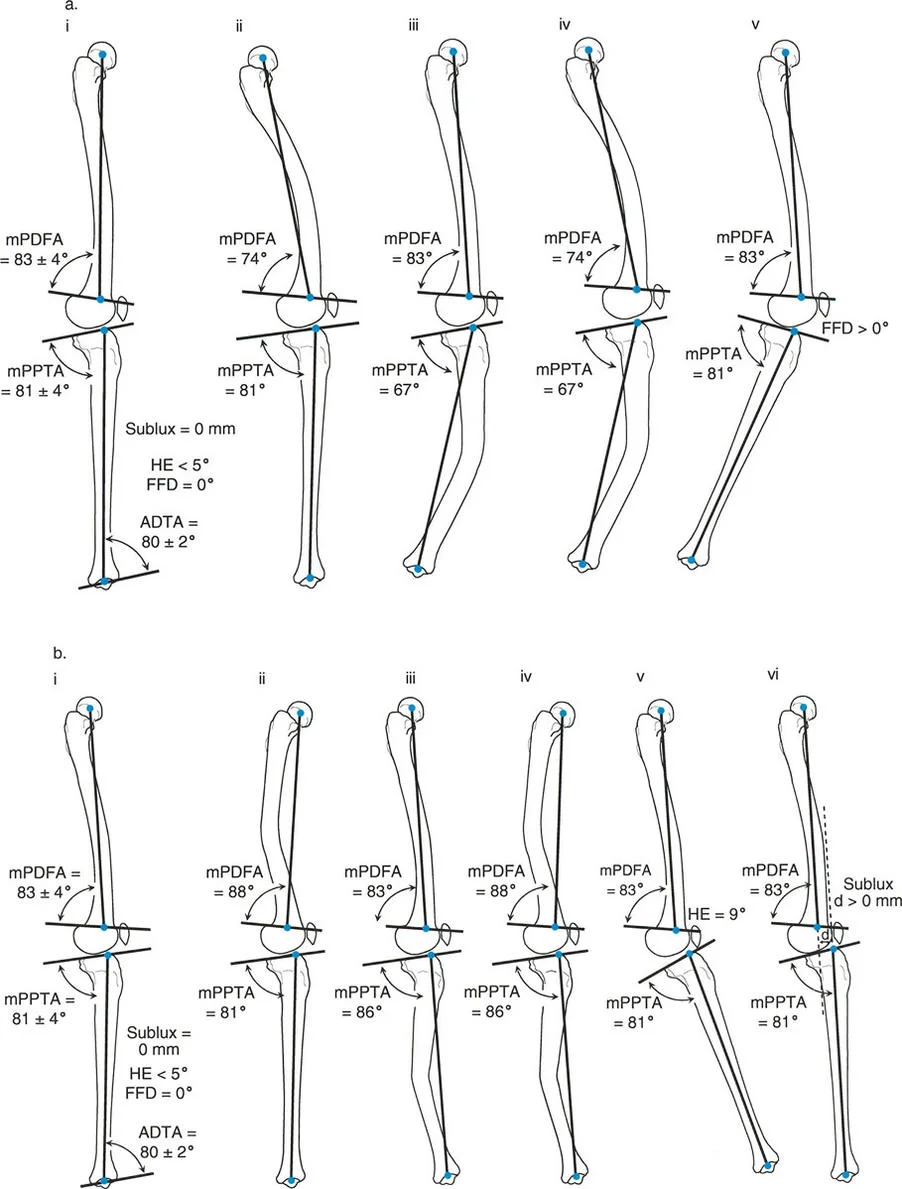
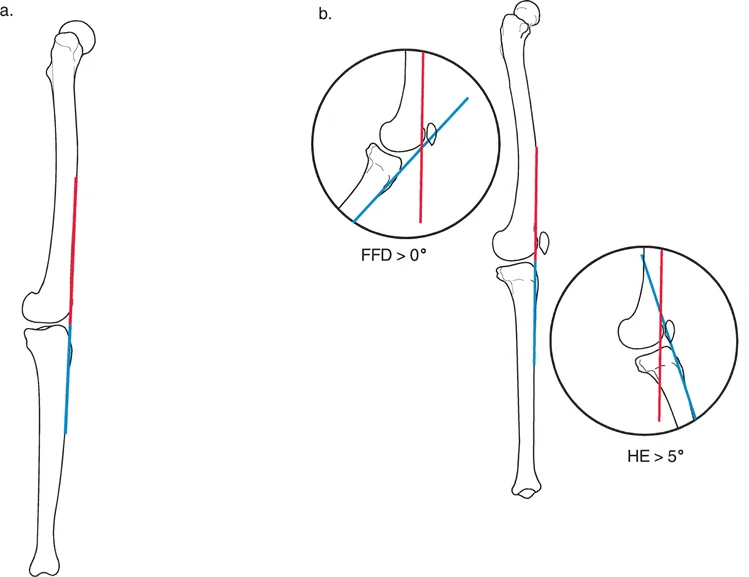
The sagittal plane joint centers of rotation for the hip, knee, and ankle normally become perfectly collinear when the knee reaches approximately five to ten degrees of flexion.
During a normal gait cycle, knee extension usually does not exceed five degrees of flexion. This implies that the capsuloligamentous structures of the posterior knee do not normally restrict terminal knee extension during dynamic gait. Instead, the eccentric action of the hamstring muscles acts as a dynamic brake, preventing the knee from snapping into full hyperextension. Therefore, knee hyperextension due to a recurvatum deformity of the femur, tibia, or the knee joint itself usually does not manifest during the actual gait cycle, even if it is glaringly obvious during static physical examination or standing.
Compensatory Mechanisms in the Sagittal Plane
Knee malalignment in the sagittal plane is generally much better tolerated by patients than malalignment in the frontal plane. Because all three major lower extremity joints move in the sagittal plane, they can dynamically compensate for the bony deformity.
Recurvatum deformities are characterized by an apex posterior angulation. A recurvatum deformity of the tibia or femur can be easily compensated for by simply flexing the knee joint. The patient walks with a slightly flexed knee, returning the overall mechanical axis to a functional position relative to the center of gravity.
Procurvatum deformities are characterized by an apex anterior angulation. Procurvatum is slightly less well tolerated than recurvatum because compensating for it requires knee hyperextension. While the knee has a massive capacity for flexion, its capacity for hyperextension is anatomically limited by the posterior capsule and cruciate ligaments.
Sagittal Loading and Osteoarthritis
Malalignment in the frontal plane dramatically shifts load to either the medial or lateral compartment, rapidly accelerating unilateral osteoarthritis. In the sagittal plane, however, the femur is round in its sagittal profile. Overloading of one specific compartment does not occur in the same binary way.
Interestingly, early osteoarthritic lesions of the knee are predominantly found in the posterior aspect of the condyles rather than the anterior aspect. Because the posterior condyles bear the brunt of the load during deep flexion activities, and because compensatory mechanisms for sagittal deformities often force the knee into prolonged dynamic flexion, the posterior cartilage experiences accelerated wear and tear.
Paley Principles Applied to the Sagittal Plane
To master sagittal deformity correction, the surgeon must apply the foundational Paley principles. These principles rely on precise geometric analysis to restore normal joint orientation and mechanical alignment.
Center of Rotation of Angulation
The Center of Rotation of Angulation represents the exact point where the proximal and distal anatomical or mechanical axes of a deformed bone intersect. Identifying the Center of Rotation of Angulation is the most critical step in preoperative planning. In the sagittal plane, identifying this point can be more challenging than in the frontal plane because the femur and tibia possess natural sagittal bows. The femur has a normal anterior bow, and the tibia has a subtle multi-apical contour. Surgeons must use mid-diaphyseal lines rather than straight mechanical lines to accurately locate the apex of the deformity.
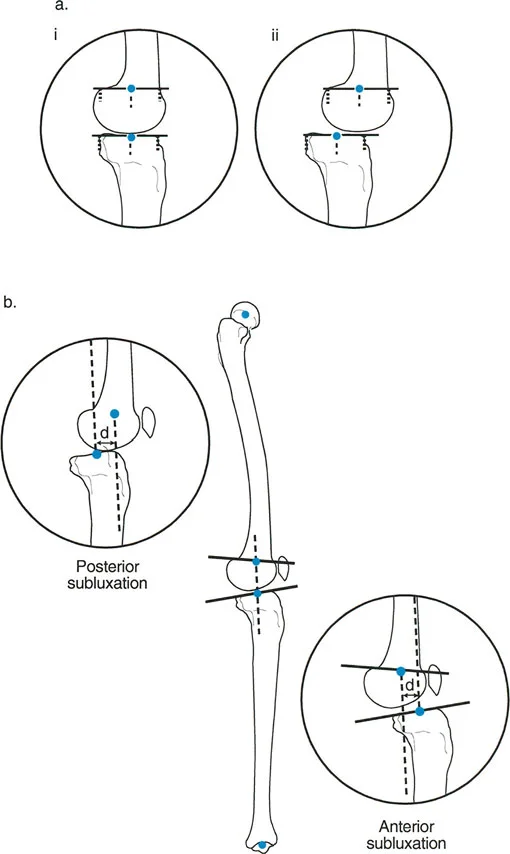
Mechanical Axis Deviation in the Sagittal Plane
Mechanical Axis Deviation in the sagittal plane is evaluated by drawing the mechanical axis from the center of the femoral head to the center of the talus on a full length lateral radiograph. Normally, this line passes slightly anterior to the center of the knee. If the line falls posterior to the knee center, the patient has a sagittal Mechanical Axis Deviation that promotes knee buckling. If it falls too far anteriorly, it promotes severe hyperextension thrusts.
Sagittal Joint Orientation Angles
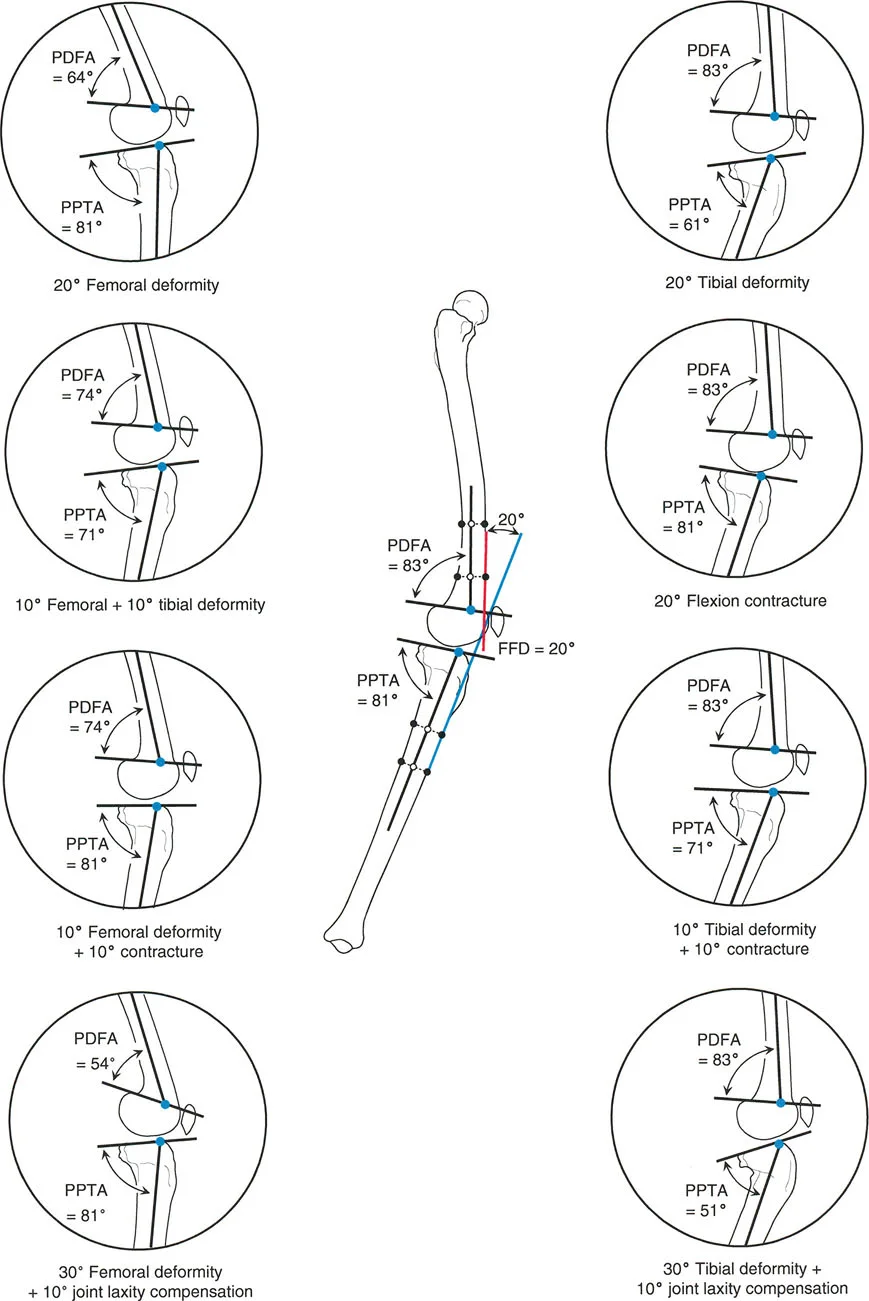
Accurate deformity correction requires restoring the normal orientation of the joints relative to the mechanical and anatomic axes of the bones. In the sagittal plane, we rely on specific posterior angles.
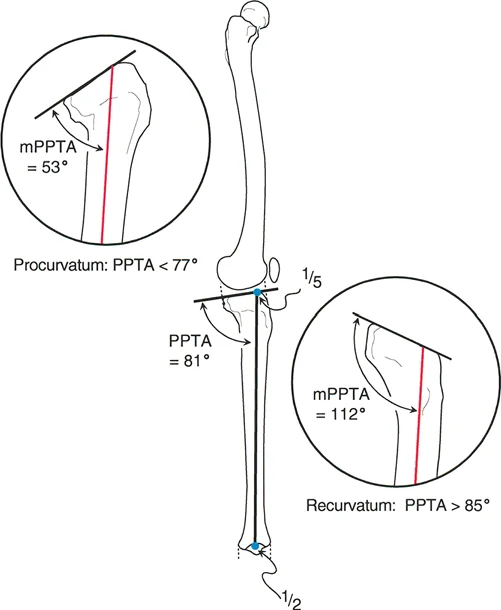
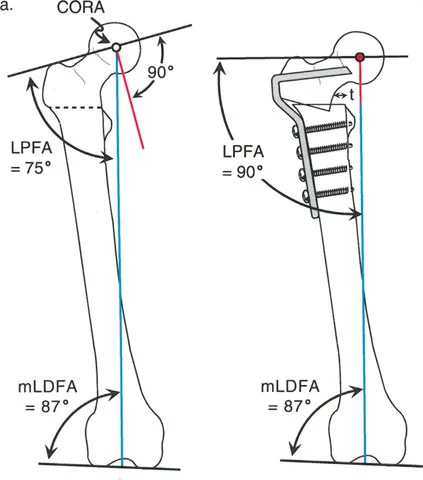
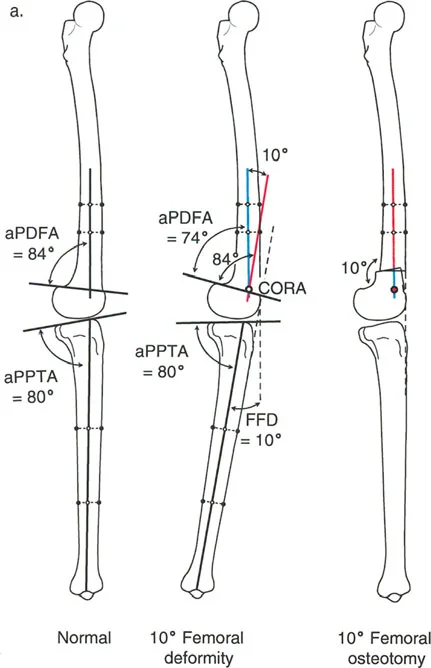
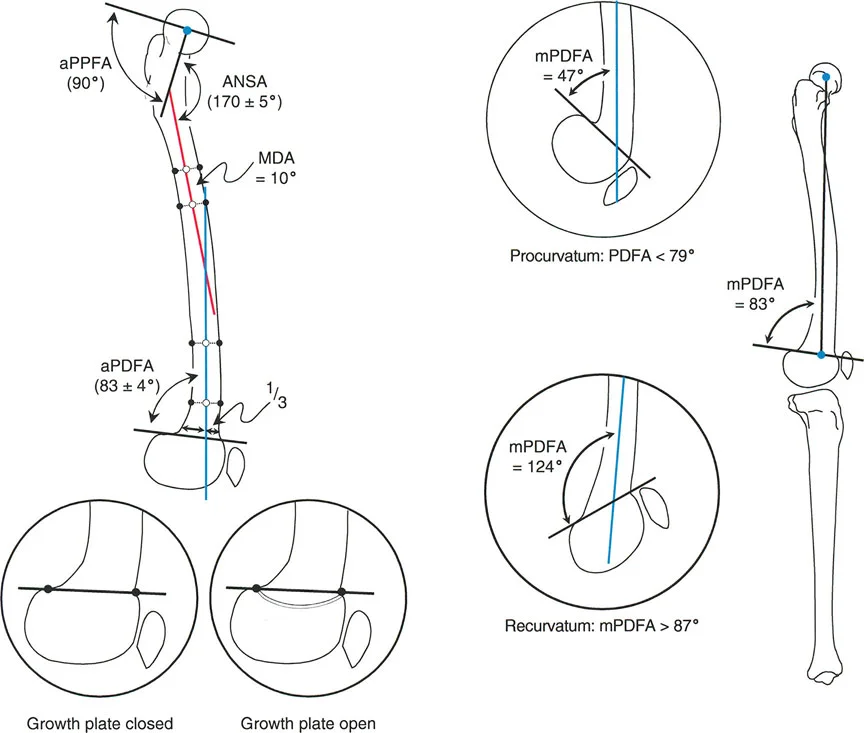
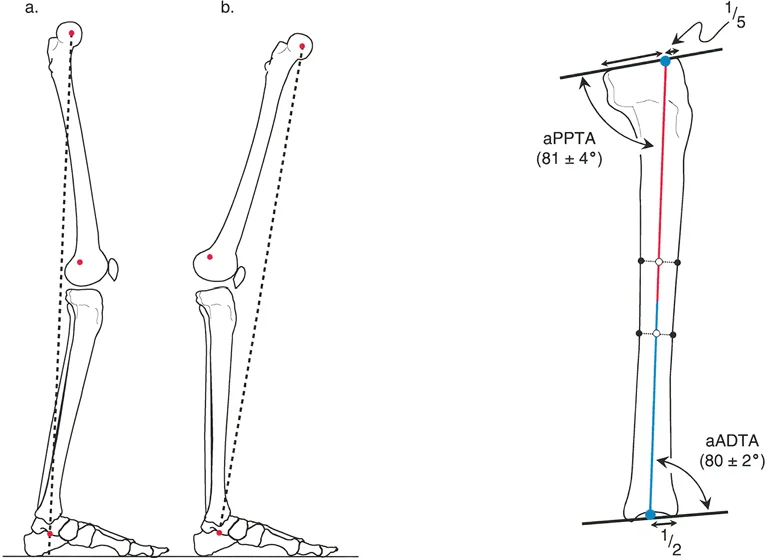
The mechanical Posterior Distal Femoral Angle is the posterior inner angle formed by the mechanical axis of the femur and the joint line of the distal femur. The mechanical Posterior Proximal Tibial Angle is the posterior inner angle formed by the mechanical axis of the tibia and the joint line of the proximal tibia.
Normal Reference Values
Understanding the normal baseline values is essential for identifying the magnitude of the deformity and calculating the required correction.
| Angle Designation | Full Name | Normal Value Range | Average Value |
|---|---|---|---|
| mPDFA | Mechanical Posterior Distal Femoral Angle | 79° to 87° | 83° |
| aPDFA | Anatomic Posterior Distal Femoral Angle | 79° to 87° | 83° |
| mPPTA | Mechanical Posterior Proximal Tibial Angle | 77° to 84° | 81° |
| aPPTA | Anatomic Posterior Proximal Tibial Angle | 77° to 84° | 81° |
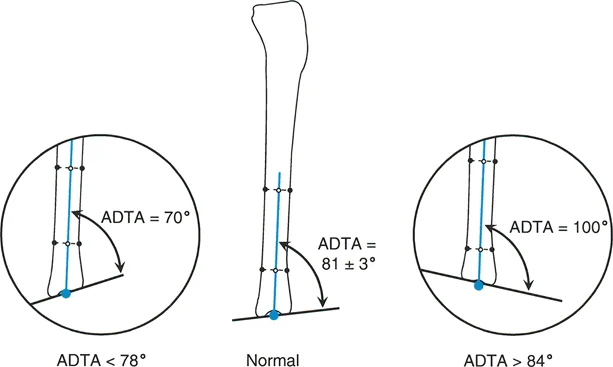
| aADTA | Anatomic Anterior Distal Tibial Angle | 78° to 82° | 80° |
Surgical Pearl
Always measure the contralateral normal limb if available. Patient specific anatomy often deviates from population averages, and the uninjured side serves as the ultimate template for perfect restoration of the sagittal joint orientation angles.
Deconstructing Procurvatum Deformities
Procurvatum is an apex anterior deformity. It can occur in the femur or the tibia and drastically alters the biomechanics of the lower extremity.
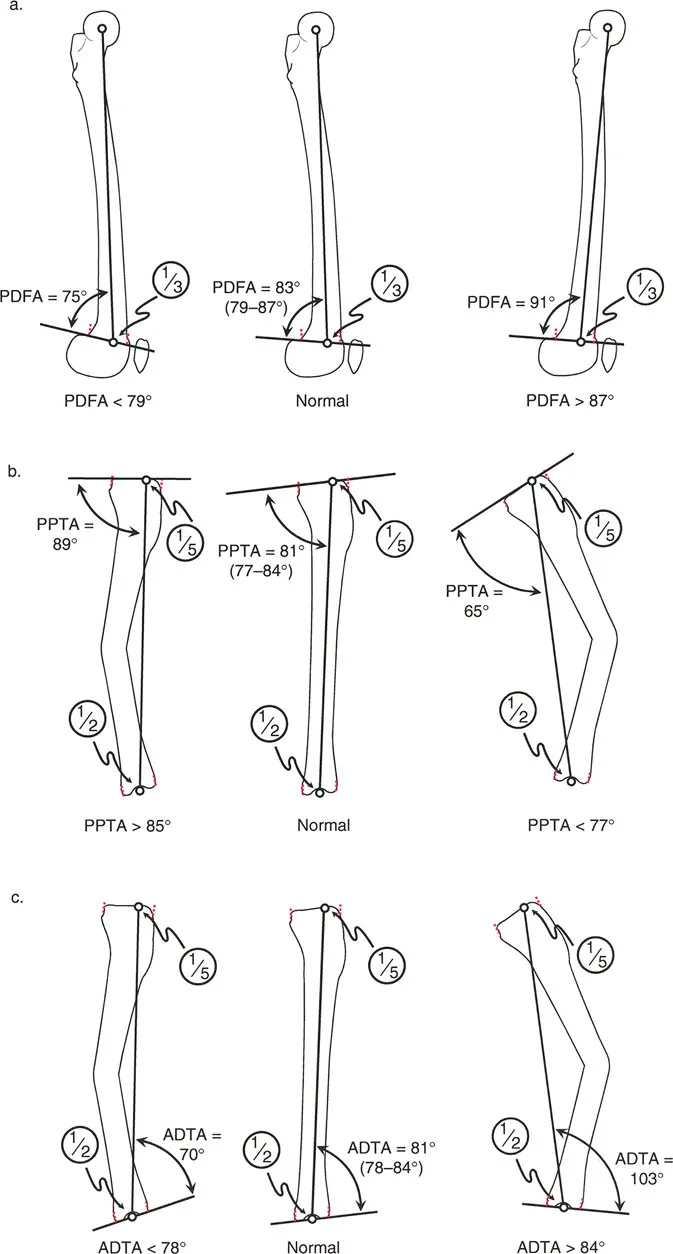
When a procurvatum deformity occurs in the distal femur, it increases the mechanical Posterior Distal Femoral Angle beyond the normal eighty three degrees. When it occurs in the proximal tibia, it increases the mechanical Posterior Proximal Tibial Angle beyond the normal eighty one degrees.
Biomechanical Consequences of Procurvatum
A procurvatum deformity essentially mimics a joint flexion contracture. Because the apex is anterior, the distal articular surface tilts posteriorly. To keep the foot flat on the ground and the torso upright, the patient must hyperextend the knee.
However, because the posterior capsule restricts hyperextension, the patient often cannot fully compensate. This results in a functional limb length discrepancy. The limb acts shorter than it anatomically is, leading to a vaulting gait or a drop pelvic gait on the affected side. Over time, the constant strain on the posterior capsular structures can lead to chronic pain and instability.
Deconstructing Recurvatum Deformities
Recurvatum is an apex posterior deformity. This is the exact opposite of procurvatum and presents its own unique set of clinical challenges.
A recurvatum deformity in the distal femur decreases the mechanical Posterior Distal Femoral Angle below the normal eighty three degrees. In the proximal tibia, it decreases the mechanical Posterior Proximal Tibial Angle below the normal eighty one degrees.
Biomechanical Consequences of Recurvatum
Recurvatum tilts the distal articular surface anteriorly. To maintain an upright posture and keep the foot plantigrade, the patient must flex the knee. As discussed earlier, the knee has a massive capacity for flexion, making recurvatum much easier to compensate for than procurvatum.
However, this compensation comes at a cost. Walking with a constantly flexed knee eliminates the passive knee locking mechanism. The quadriceps must fire continuously during the stance phase of gait. This leads to profound anterior knee pain, patellofemoral overloading, and rapid muscular fatigue. Severe recurvatum deformities can also stretch the anterior cruciate ligament over time, leading to secondary sagittal plane instability.
Step by Step Radiographic Evaluation
Accurate measurement of sagittal plane deformities is impossible without pristine, standardized radiographs. A poorly positioned lateral radiograph will distort the joint orientation angles and lead to catastrophic errors in surgical planning.
Acquiring the Perfect Lateral Radiograph
To obtain a true lateral radiograph of the lower extremity, the x-ray beam must be directed strictly perpendicular to the sagittal plane of the knee.
- Positioning the Patella The patella must be pointing straight forward relative to the x-ray cassette.
- Overlapping Condyles The posterior borders of the medial and lateral femoral condyles must perfectly overlap. If one condyle projects significantly posterior to the other, the film is rotated and the posterior distal femoral angle cannot be accurately measured.
- Full Length View A full length lateral view from the hip to the ankle is ideal, though technically difficult to obtain due to the density of the contralateral limb. Often, stitched lateral views or carefully calibrated segmental views are required.
Surgical Pearl
When evaluating the proximal tibia on a lateral radiograph, ensure the fibular head is properly positioned. The anterior half of the fibular head should overlap the posterior half of the tibia. If the fibula is completely completely separated from the tibia or completely hidden behind it, the rotation is incorrect.
Paley Osteotomy Rules for Sagittal Deformities
The genius of Paley principles lies in the Osteotomy Rules. These rules dictate exactly where the bone should be cut and where the hinge or axis of correction should be placed to achieve perfect realignment without creating secondary translational deformities.
Executing the Osteotomy Rules
Rule One
When the osteotomy and the axis of correction are both located at the Center of Rotation of Angulation, the deformity is corrected by pure angulation. The mechanical axis is fully restored, and the bone ends remain perfectly aligned without any translation. This is the ideal scenario for most procurvatum and recurvatum corrections.
Rule Two
When the osteotomy is made at a different level than the Center of Rotation of Angulation, but the axis of correction remains at the Center of Rotation of Angulation, the deformity is corrected by a combination of angulation and translation. The mechanical axis is restored, but the bone ends will be offset. This is often required when the Center of Rotation of Angulation is located too close to the joint line, making a Rule One osteotomy impossible due to lack of adequate bone stock for hardware fixation.
Rule Three
When the osteotomy and the axis of correction are both located outside the Center of Rotation of Angulation, a secondary translation deformity is created. The mechanical axis will not be restored, and the overall alignment will remain pathological. This is a common pitfall for inexperienced surgeons and must be strictly avoided.
Surgical Planning and Correction Strategies
Surgical correction of sagittal deformities requires meticulous preoperative planning. Whether using an intramedullary nail, a locking plate, or a circular external fixator, the geometric principles remain identical.
Preoperative Planning Workflow
- Draw the Joint Lines Establish the distal femoral and proximal tibial joint lines on the lateral radiograph.
- Draw the Normal Axes Draw the normal mechanical axes projecting from the joint lines using the standard reference angles.
- Draw the Diaphyseal Axes Draw the mid-diaphyseal lines of the proximal and distal bone segments.
- Identify the Intersection Mark the point where the proximal and distal diaphyseal lines intersect. This is the Center of Rotation of Angulation.
- Measure the Magnitude Measure the angle between the intersecting lines to determine the exact degree of procurvatum or recurvatum.
- Plan the Osteotomy Select the osteotomy site based on Paley Osteotomy Rules, prioritizing Rule One whenever anatomically possible.
- Simulate the Correction Use digital templating software or traditional paper cutouts to simulate the osteotomy and verify that the mechanical axis is restored.
Advanced Concepts in Sagittal Deformity Correction
Correcting sagittal plane deformities often requires managing complex soft tissue envelopes and understanding the difference between pure angulation and translation.
Translation Versus Angulation
In the sagittal plane, isolated translation deformities can occur, typically following trauma or malunion of a diaphyseal fracture. A pure translation deformity means the proximal and distal axes are parallel but not collinear.
Correcting translation requires a different approach than correcting angulation. If a surgeon attempts to correct a pure translation deformity by angulating the bone, they will inadvertently create a new joint orientation angle deformity. Translation must be corrected with translation, and angulation must be corrected with angulation.
When using circular external fixation, such as the Taylor Spatial Frame or Ilizarov apparatus, the software can easily calculate simultaneous correction of angulation and translation. However, when using internal fixation, the surgeon must manually execute these corrections, often requiring specialized blocking screws or reduction clamps to control the sagittal translation during nail insertion.
Managing Soft Tissue Contractures
Bony correction is only half the battle. Sagittal deformities are frequently accompanied by severe soft tissue contractures.
In long standing procurvatum deformities, the posterior structures including the gastrocnemius, hamstrings, and posterior joint capsule become severely contracted. Correcting the bony deformity acutely may stretch the posterior neurovascular bundle, leading to catastrophic sciatic or tibial nerve palsy.
Surgical Pearl
If the required correction exceeds twenty degrees in the sagittal plane, strongly consider gradual correction using a circular external fixator rather than acute correction with internal hardware. Gradual correction allows the soft tissues to undergo distraction histogenesis, safely stretching the nerves and vessels at a rate of one millimeter per day.
Postoperative Rehabilitation and Dynamic Assessment
The ultimate success of a sagittal plane deformity correction is not judged on a static postoperative radiograph, but rather in the gait lab and the physical therapy clinic.
Because the sagittal plane is the primary plane of motion for ambulation, rehabilitation must focus heavily on restoring dynamic kinematics. Patients who have lived with a recurvatum deformity for years will have deeply ingrained compensatory gait patterns, such as a habitual knee flexion thrust. Even after the bone is perfectly straightened, the brain will continue to command the muscles to walk with a flexed knee.
Intensive physical therapy focusing on quadriceps re-education, hamstring stretching, and proprioceptive gait training is mandatory. The surgeon must actively monitor the patient for resolution of the quadriceps fatigue and the return of the passive knee locking mechanism during the stance phase of gait. Only when the patient can ambulate efficiently without active quadriceps firing during stance can the sagittal plane deformity correction be considered a true success.
!!! info "Academic Resource & Medical Review"
This academic resource was prepared and medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is formulated specifically for medical students, orthopedic residents, and surgeons preparing for high-stakes board examinations (AAOS, FRCS Tr & Orth, Arab Board).
!!! warning "Disclaimer"
The surgical techniques, classifications, and clinical guidelines presented herein are for educational and academic review purposes only. They are not intended to replace institutional protocols or independent clinical judgment.
You Might Also Like