Spinal Accessory Nerve Injury & Repair: Surgical Guide
Key Takeaway
The spinal accessory nerve is highly susceptible to iatrogenic and penetrating trauma within the posterior cervical triangle. Injury results in profound trapezius paralysis, shoulder sagging, and debilitating pain. This guide details the comprehensive management of spinal accessory nerve palsy, encompassing clinical evaluation, electrodiagnostic testing, and precise surgical interventions ranging from primary end-to-end neurorrhaphy to complex interfascicular nerve grafting for optimal functional restoration.
CERVICAL PLEXUS ANATOMY AND NEUROLOGY
The cervical plexus is a complex neural network formed by the union of the anterior primary rami of the first four cervical nerves (C1–C4). Situated deep in the neck, it lies anterolateral to the levator scapulae and middle scalene muscles, and deep to the internal jugular vein and sternocleidomastoid (SCM) muscle. The plexus provides critical sensory innervation to the neck, upper thorax, and scalp, as well as motor innervation to several anterior neck muscles and the diaphragm.
Sensory Branches
Sensory fibers originating from the upper two or three cervical segments emerge from the posterior border of the SCM (Erb’s point) and course through several distinct nerves:
* Lesser Occipital Nerve (C2): Ascends along the posterior border of the SCM to supply the skin of the scalp posterior and superior to the auricle.
* Greater Auricular Nerve (C2, C3): Ascends across the SCM to innervate the skin over the parotid gland, the posterior aspect of the auricle, and the lobule.
* Transverse Cervical Nerve (Anterior Cutaneous Nerve of the Neck) (C2, C3): Courses anteriorly across the SCM to supply the anterolateral skin of the neck.
* Supraclavicular Nerves (C3, C4): Emerge as a common trunk that divides into medial, intermediate, and lateral branches, providing sensory coverage to the skin over the clavicle, the anteromedial shoulder, and the upper thorax down to the level of the second rib.
Motor Branches
The motor distribution of the cervical plexus is equally vital, contributing to the stabilization and movement of the hyoid bone and larynx, as well as respiration:
* Ansa Cervicalis (Ansa Hypoglossi): Formed by a superior root (C1, briefly traveling with the hypoglossal nerve) and an inferior root (C2, C3). This loop innervates the infrahyoid "strap" muscles: the thyrohyoid, geniohyoid, omohyoid, sternothyroid, and sternohyoid.
* Phrenic Nerve (C3, C4, C5): The most critical motor branch of the cervical plexus. Branches from C3, C4, and C5 unite to form the phrenic nerve, which descends obliquely across the anterior scalene muscle to provide the sole motor innervation to the diaphragm.
Clinical Pearl: The classic anatomical mnemonic "C3, 4, and 5 keep the diaphragm alive" underscores the critical nature of these nerve roots. High cervical spine injuries above C3 typically result in complete respiratory paralysis.
THE SPINAL ACCESSORY NERVE (CRANIAL NERVE XI)
The spinal accessory nerve (SAN) is unique among cranial nerves due to its dual origin and complex anatomical course. It is a pure motor nerve responsible for the innervation of the sternocleidomastoid and the trapezius muscles, playing a paramount role in shoulder girdle biomechanics.
Anatomical Course
Fibers arising from the lateral aspect of the anterior horns of the upper five cervical segments (C1–C5) unite to form the spinal root of the accessory nerve. This root ascends into the cranial cavity through the foramen magnum. Within the posterior cranial fossa, it is joined by its cranial counterpart, which consists primarily of rootlets destined to pass with the vagus nerve (CN X).
These combined rootlets exit the skull via the jugular foramen. Immediately after exiting, the cranial rootlets diverge from the spinal accessory nerve to course with the vagus fibers, contributing to the innervation of the pharynx and larynx.
The spinal accessory nerve then descends into the neck, passing beneath the posterior belly of the digastric muscle. It receives communicating branches from the anterior primary rami of C2, C3, and C4. The nerve pierces and innervates the sternocleidomastoid muscle, emerging from its posterior border at the junction of the upper and middle thirds (Erb's point). It then traverses the posterior cervical triangle obliquely, descending further to enter the deep surface of the trapezius muscle, innervating its superior, middle, and inferior thirds.
Vulnerability in the Posterior Cervical Triangle
The SAN is highly susceptible to injury at any point along its course, but its superficial location within the posterior cervical triangle makes it exceptionally vulnerable. In this region, the nerve lies embedded in the investing layer of deep cervical fascia, covered only by skin, subcutaneous tissue, and platysma.
Common mechanisms of injury include:
* Iatrogenic Trauma: The most frequent cause of SAN palsy. Procedures such as posterior triangle lymph node biopsy, radical or modified neck dissections, excision of benign masses (e.g., lipomas, sebaceous cysts), and central venous catheter placement carry a high risk of inadvertent transection or traction injury.
* Penetrating Trauma: Lacerations from glass, knife wounds, or low-velocity missile injuries.
* Blunt Trauma: Severe traction injuries to the shoulder girdle (similar to upper brachial plexus injuries) or direct blows to the posterior neck.
CLINICAL PRESENTATION AND DIAGNOSIS
The clinical manifestation of a spinal accessory nerve injury is profound and debilitating, primarily due to the paralysis of the trapezius muscle. Woodhall provided the seminal description of the symptoms and findings that follow surgical injury to this nerve, often referred to as "Spinal Accessory Nerve Syndrome."
Symptomatology
Patients typically present with a triad of shoulder dysfunction, visible deformity, and severe pain:
1. Generalized Weakness: Profound weakness in the affected shoulder girdle and arm.
2. Loss of Abduction: Inability to actively abduct the shoulder beyond 90 degrees. The trapezius is essential for upward rotation of the scapula, which is a prerequisite for full glenohumeral abduction.
3. Sensory Disturbance and Pain: While the SAN is a motor nerve, its injury leads to a severe, aching pain. This pain may vary from a pulling sensation in the region of the surgical scar to a deep ache in the shoulder and arm. The aching frequently radiates to the medial margin of the scapula and down the arm to the fingers. This pain is secondary to the loss of trapezius support, causing the shoulder girdle to droop and placing chronic, debilitating traction on the brachial plexus.
Physical Examination Findings
Careful inspection and dynamic testing will reveal classic signs of trapezius paralysis:
* Atrophy: The superior one-third of the trapezius muscle on the affected side always atrophies, leading to a hollowed appearance of the supraclavicular fossa.
* Shoulder Ptosis: The affected shoulder sags visibly at rest.
* Scapular Dyskinesis (Winging): The scapula rotates distally and laterally, and flares slightly. Crucially, its inferior angle is closer to the midline than its superior angle.
* Dynamic Accentuation: This abnormal scapular position is accentuated when the arm is abducted. However, the flaring of the inferior angle disappears when the arm is raised anteriorly (forward flexion).
Diagnostic Pitfall: It is imperative to differentiate SAN palsy from long thoracic nerve palsy (serratus anterior paralysis). In serratus anterior paralysis, the scapula translates medially, the inferior angle rotates laterally, and the winging is accentuated by forward flexion against resistance (e.g., doing a wall push-up). In SAN palsy, the winging is lateral, the inferior angle rotates medially, and winging is accentuated by abduction.
Electrodiagnostic Evaluation
If the nerve has been injured by a low-velocity missile or blunt trauma, and if no vascular or visceral injuries require immediate surgical exploration, simple observation for 3 to 4 weeks is recommended.
If clinical evidence of return of function is absent after this period, Electromyography (EMG) and Nerve Conduction Studies (NCS) are mandatory. Electrodiagnostic examination revealing fibrillation potentials and positive sharp waves (denervation) in the trapezius, without voluntary motor unit action potentials, confirms a severe axonotmetic or neurotmetic injury, indicating the need for surgical exploration.
SURGICAL MANAGEMENT
The timing and type of surgical intervention depend heavily on the mechanism of injury and the time of diagnosis.
Indications and Timing
- Immediate Repair: When injury to the nerve is detected intraoperatively (e.g., during a lymph node biopsy), primary end-to-end repair should be attempted immediately if circumstances permit.
- Delayed Repair (2-3 Weeks): When the injury is not appreciated during the index operation, or when removal of a segment of the nerve is necessary as part of an oncological resection, reconstructive procedures should be delayed 2 to 3 weeks. This allows the initial wound to heal, decreases local inflammation, and allows the extent of nerve end neuroma formation to declare itself.
- Contraindications to Early Repair: When a segment of the nerve has been removed for malignancy, the patient’s overall prognosis or the need for adjuvant therapies (such as postoperative irradiation) may preclude immediate additional nerve procedures.
Surgical Alternatives
When the patient’s condition permits, symptoms warrant treatment, and the gap created by segmental resection or retraction is too great to close by tension-free end-to-end suture, the surgeon must employ advanced reconstructive techniques:
1. Interfascicular Nerve Grafting: The gold standard for bridging nerve gaps.
2. Tendon Transfer: A salvage procedure (e.g., the Eden-Lange procedure, transferring the levator scapulae, rhomboid minor, and rhomboid major) reserved for cases where nerve repair has failed or the injury is chronic (typically >12-18 months) and the motor endplates of the trapezius have irreversibly degenerated.
Surgical Approach and Technique
The following approach allows satisfactory exposure for neurolysis, primary suture, or nerve grafting.
1. Positioning and Incision
The patient is placed in the supine position with a sandbag under the ipsilateral scapula. The head is turned to the contralateral side, and the neck is slightly extended.
When the initial wound has healed well, a transverse incision is made across the middle of the posterior triangle, meticulously following the natural skin folds (Langer's lines) of the neck to ensure an optimal cosmetic result.
2. Nerve Identification
The terminal part of the spinal accessory nerve must be located at two constant anatomical landmarks:
* Proximal Landmark: The nerve emerges at the junction of the proximal and middle thirds of the sternocleidomastoid muscle (Erb's point).
* Distal Landmark: It courses diagonally, distally, and posteriorly to enter the lateral border of the trapezius muscle at the junction of its middle and distal thirds.
The incision should be long enough to permit exact identification of both the distal and proximal stumps of the nerve.
Surgical Warning: Extreme care must be taken not to confuse the lesser occipital and greater auricular nerves with the spinal accessory nerve. The sensory nerves course superiorly and anteriorly, whereas the SAN courses inferiorly and posteriorly.
3. Intraoperative Stimulation and Neurolysis
Once identified, the proximal part of the nerve should be stimulated using a handheld nerve stimulator. Contraction of the trapezius muscle indicates that the nerve has not been completely severed (e.g., a neurapraxia or axonotmesis in continuity).
The entire nerve is exposed within the posterior triangle. If the nerve is in continuity but extensive scarring is present within or around the epineurium, a meticulous external and internal neurolysis is performed under loupe or microscopic magnification.
4. Preparation of Nerve Ends
If the nerve has been divided, its ends will likely have formed neuromas (proximal neuroma and distal glioma). The ends must be mobilized gently. Using a fresh scalpel blade or nerve scissors, the scarred ends are sectioned back serially (in "bread-loaf" fashion) until healthy, pouting funiculi (fascicles) are visualized.
5. Primary End-to-End Neurorrhaphy
An end-to-end suture is performed only if it can be achieved under little or no tension. Awkward positioning of the head, neck, and shoulders in a cast to allow suturing of the nerve without tension should be strictly avoided, as postoperative mobilization will inevitably stretch and rupture the repair. Repair is typically performed using 8-0 or 9-0 non-absorbable monofilament sutures placed through the epineurium.
Interfascicular Nerve Grafting
If a tension-free primary repair is impossible, interfascicular nerve grafting is the most satisfactory alternative. The sural nerve or the great auricular nerve (if expendable) are common donor sites.
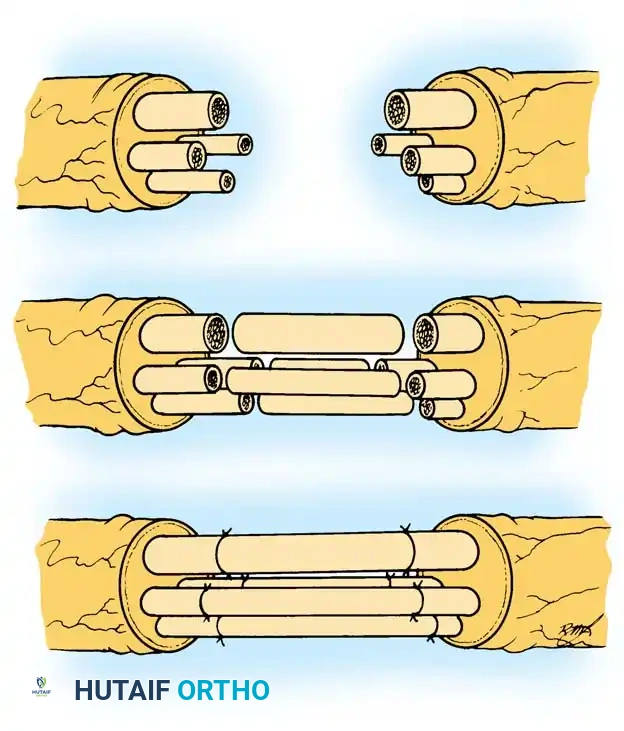
Fig. 59-16 Interfascicular nerve grafting. The scarred nerve ends are resected to healthy fascicles. Cable grafts (typically harvested from the sural nerve) are interposed between the proximal and distal stumps to bridge the gap without tension. Fine epineurial sutures secure the grafts in place, allowing regenerating axons to cross the surgical sites.
Grafting Technique:
1. Measure the defect accurately with the neck in a neutral position.
2. Harvest a nerve graft 10-15% longer than the measured defect to account for graft shrinkage and ensure absolute tension-free coaptation.
3. Divide the donor nerve into appropriate lengths to create "cables" that match the cross-sectional area of the SAN.
4. Suture the grafts in place using microsurgical techniques, aligning the fascicles as accurately as possible.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Postoperative care is dictated by the security of the repair and the presence of tension.
- Immobilization: If the line of suture is completely free of tension (either via primary repair or grafting), the shoulder should be immobilized in a Velpeau bandage or a broad arm sling for 3 to 4 weeks. This prevents the weight of the arm from pulling on the trapezius and stressing the repair site.
- Early Phase (0-4 Weeks): Strict avoidance of active shoulder elevation or neck stretching. Passive range of motion of the elbow, wrist, and hand is encouraged to prevent stiffness.
- Intermediate Phase (4-8 Weeks): The sling is gradually weaned. Gentle active-assisted exercises for the shoulder are initiated. Scapular stabilization exercises (focusing on the rhomboids and levator scapulae) are begun to provide compensatory support.
- Late Phase (8+ Weeks): Normal daily activities are progressively resumed 6 to 8 weeks after surgery. Progressive resistance exercises for the trapezius are delayed until clinical or electromyographic evidence of reinnervation is present (often 3 to 6 months postoperatively, depending on the distance from the repair to the motor endplates).
OUTCOMES AND PROGNOSIS
While large-scale, randomized controlled trials on the results of suturing the spinal accessory nerve are scarce, the existing literature provides a highly optimistic consensus.
Because the spinal accessory nerve is a purely motor nerve, regenerating axons do not suffer from the "sensory-motor mismatch" that plagues mixed nerve repairs. As emphasized by Seddon, excellent functional results can be expected following meticulous microsurgical repair.
Historical and contemporary reports by Woodhall, Dunn, Wright, Vastamäki, and Solonen consistently suggest that neurolysis, primary repair, or interfascicular grafting—when performed with appropriate indications and microsurgical technique—reliably relieve the debilitating traction pain and restore functional shoulder abduction and elevation. The key to success remains early recognition of the iatrogenic injury and prompt, tension-free surgical reconstruction.
📚 Medical References
- spinal accessory nerve, burners/stingers, thoracic outlet syndrome, Am J Sports Med 32:1063, 2004.
- Saha AK: The classic: mechanism of shoulder movements and a plea for the recognition of “zero position” of glenohumeral joint, Clin Orthop Relat Res 173:3, 1983.
- Sanders TG, Miller MD: A systematic approach to magnetic resonance imaging interpretation of sports medicine injuries of the shoulder, Am J Sports Med 33:1088, 2005.
- Sarkar K, Uhthoff HK: Ultrastructure of the subacromial bursa in painful shoulder syndromes, Virchows Arch 400:107, 1983.
- Schaefer O, Winterer J, Lohrmann C, et al: Magnetic resonance imaging for supraspinatus muscle atrophy after cuff repair, Clin Orthop Relat Res 403:93, 2002.
- Scheibel M, Magosch P, Pritsch M, et al: The belly-off sign: a new clinical diagnostic sign for subscapularis lesions, Arthroscopy 21:1229, 2005.
- Schneider K, Kasparyan NG, Altchek DW, et al: An aneurysm involving the axillary artery and its branch vessels in a major league baseball pitcher: a case report and review of the literature, Am J Sports Med 27:370, 1999.
- Sclamberg SG, Tibone JE, Itamura JM, et al: Six-month magnetic resonance imaging follow-up of large and massive rotator cuff repairs reinforced with porcine small intestinal submucosa, J Sboulder Elbow Surg 13:538, 2004.
- Seeger LL, Gold RH, Bassett LW, et al: Shoulder impingement syndrome: MR fi ndings in 53 shoulders, AJR Am J Roentgenol 150:343, 1988.
- Segmuller HE, Taylor DE, Hogan CS, et al: Arthroscopic treatment of adhesive capsulitis, J Shoulder Elbow Surg 4:403, 1995.
- Sengar DPS, McKendry RJ, Uhthoff HK: Increased frequency of HLA-A1 in calcifying tendinitis, Tissue Antigens 29:173, 1987.
- Severud EL, Routolo C, Abbott DD, et al: All-arthroscopic versus mini-open rotator cuff repair: a long-term retrospective outcome comparison, Arthroscopy 19:234, 2003.
- Sher JS, Uribe JW, Posada A, et al: Abnormal fi ndings on magnetic resonance images of asymptomatic shoulders, J Bone Joint Surg 77A:10, 1995.
- Snyder SJ, Foos GR: Arthroscopic treatment of bursal side and full thickness rotator cuff tears, Ann Chirg Gynaecol 85:117, 1996.
- Stephens SR, Warren RF, Payne LZ, et al:
You Might Also Like


