Cervical Disc Disease: Comprehensive Pathophysiology and Surgical Management
Key Takeaway
Cervical disc disease encompasses a spectrum of degenerative changes leading to radiculopathy or myelopathy. Pathophysiology involves annular degeneration and nuclear extrusion, frequently complicated by uncovertebral joint hypertrophy. Surgical management, primarily Anterior Cervical Discectomy and Fusion (ACDF) or posterior foraminotomy, is indicated for progressive neurological deficits or refractory pain. This guide details the biomechanics, clinical evaluation, and step-by-step operative techniques for managing cervical disc herniations.
Introduction and Historical Context
Herniation of the cervical intervertebral disc with subsequent spinal cord or nerve root compression has been recognized as a distinct clinical entity since Key first detailed the pathological findings of two cases of cord compression by "intervertebral substance" in 1838. Almost a century later, Mixter and Barr’s landmark 1934 report on lumbar disc herniation also included four cases of cervical disc protrusions, cementing the understanding of discogenic neurological compromise.
In an extensive epidemiological study of acute cervical disc prolapse, Kelsey et al. demonstrated that cervical disc rupture exhibits a male predominance, with a ratio of 1.4:1. Key occupational and lifestyle factors positively associated with the injury include frequent heavy lifting on the job, cigarette smoking, and frequent diving from a board. Interestingly, the use of vibrating equipment and prolonged time spent in motor vehicles were not positively associated with this specific problem. The societal burden is significant; Horal reported that up to 40% of the population in Sweden experienced neck pain at some point in their lives. Furthermore, patients presenting with cervical disc disease have a statistically higher likelihood of concurrent lumbar disc disease, suggesting a systemic predisposition to disc degeneration. Magnetic Resonance Imaging (MRI) studies consistently demonstrate a direct correlation between advancing age and increasing cervical disc degeneration.
Pathophysiology and Biomechanics
The pathophysiology of cervical disc disease mirrors the degenerative cascade observed in other regions of the spine, albeit with unique anatomical considerations specific to the cervical region.
The Degenerative Cascade
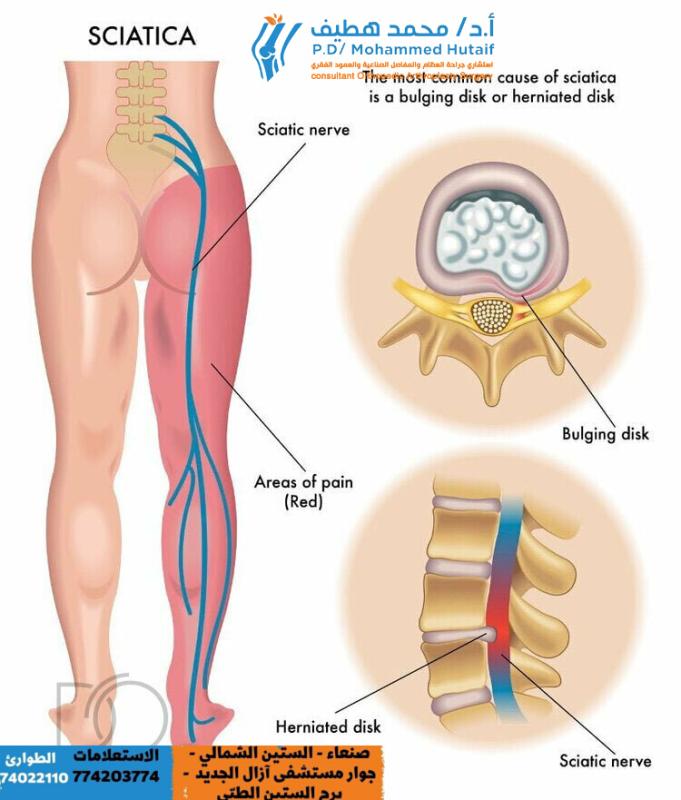
Physiological desiccation and biochemical alterations in the nucleus pulposus are followed by progressive annular degeneration. Frank extrusion of nuclear material can occur as an acute complication of this chronic degenerative process. Kramer postulated that hydraulic pressure exerted on the disc, rather than excessive physiological motion alone, is the primary mechanical driver producing traumatic disc herniation.
As disc degeneration proceeds, loss of disc height leads to hypermobility of the affected spinal segment. This micro-instability provokes a hypertrophic response, resulting in degenerative arthritic changes.
Uncovertebral Joint Hypertrophy
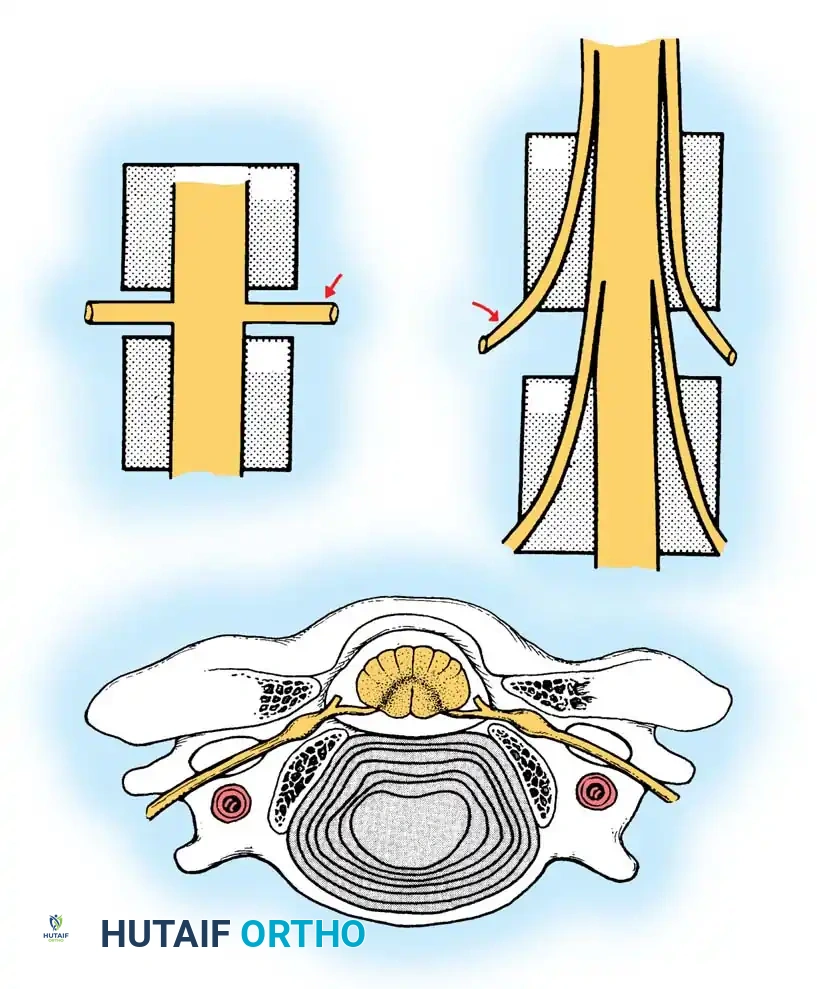
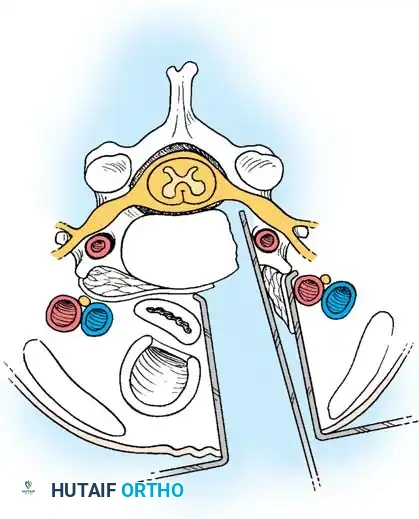
In stark contrast to the lumbar spine, hypertrophic changes in the cervical spine predominantly affect the uncovertebral joints (joints of Luschka or uncinate processes).
The uncinate process forms the ventral wall of the intervertebral foramen. As hypertrophic osteophytes develop around the uncovertebral joints, facet joints, and vertebral bodies, they encroach upon the neuroforamen, leading to lateral root pressure. In end-stage disease, progressive stiffening of the cervical spine and global loss of motion are the usual results. Occasionally, massive anterior hypertrophic spurring can mechanically compress the esophagus, resulting in dysphagia.
Biochemical and Vascular Factors
Modern research has elucidated the biochemical mediators of discogenic pain. Kang et al. identified increased production of matrix metalloproteinases (MMPs), nitric oxide (NO), prostaglandin E2 (PGE2), and interleukin-6 (IL-6) in disc material excised from cervical disc herniations. These inflammatory cytokines and enzymes are intimately involved in the biochemistry of disc degeneration and are primary culprits in nociception and radicular pain production.
Additionally, Kauppila and Penttila reported the presence of atherosclerotic and degenerative changes in the common arteries supplying the cervicobrachial area, suggesting that impaired regional blood flow and subsequent ischemia may play a contributory role in the pathogenesis of cervicobrachial disorders.
Clinical Evaluation: Signs and Symptoms
The clinical presentation of cervical intervertebral disc disease is best categorized into three distinct symptom complexes: axial spinal pain, radiculopathy (nerve root compression), and myelopathy (spinal cord compression).
Axial Spine Symptoms
When the cervical disc is punctured anteriorly (e.g., during discography), concordant pain is often noted in the neck, medial scapula, and shoulder. Anatomical studies confirm that the cervical disc and surrounding longitudinal ligaments are richly innervated, analogous to the sinu-vertebral nerve in the lumbar spine. Tamura also noted that cranial symptoms—such as headache, vertigo, tinnitus, and ocular problems—can be associated with C3-C4 root sleeve defects.
Clinical Pearl: Cervical disc disease, particularly at the C5-C6 or C6-C7 levels, can present with severe anterior chest and left arm pain, closely mimicking acute cardiac angina (pseudo-angina). A thorough cardiac workup is mandatory to rule out myocardial ischemia before attributing these symptoms solely to cervical spondylosis.
Cervical Radiculopathy
Symptoms of root compression are typically characterized by sharp, lancinating pain radiating into the arm or chest, accompanied by paresthesias, numbness in specific dermatomes, and motor weakness. Radicular symptoms are often intermittent but are usually superimposed on a background of chronic, aching neck and shoulder pain.
By meticulously evaluating specific motor groups, deep tendon reflexes, and sensory dermatomes, the exact level of the lesion can be localized with high clinical accuracy. However, the dual innervation of certain muscle groups can occasionally confound the clinical picture, making MRI confirmation essential.
Neurological Level Localization
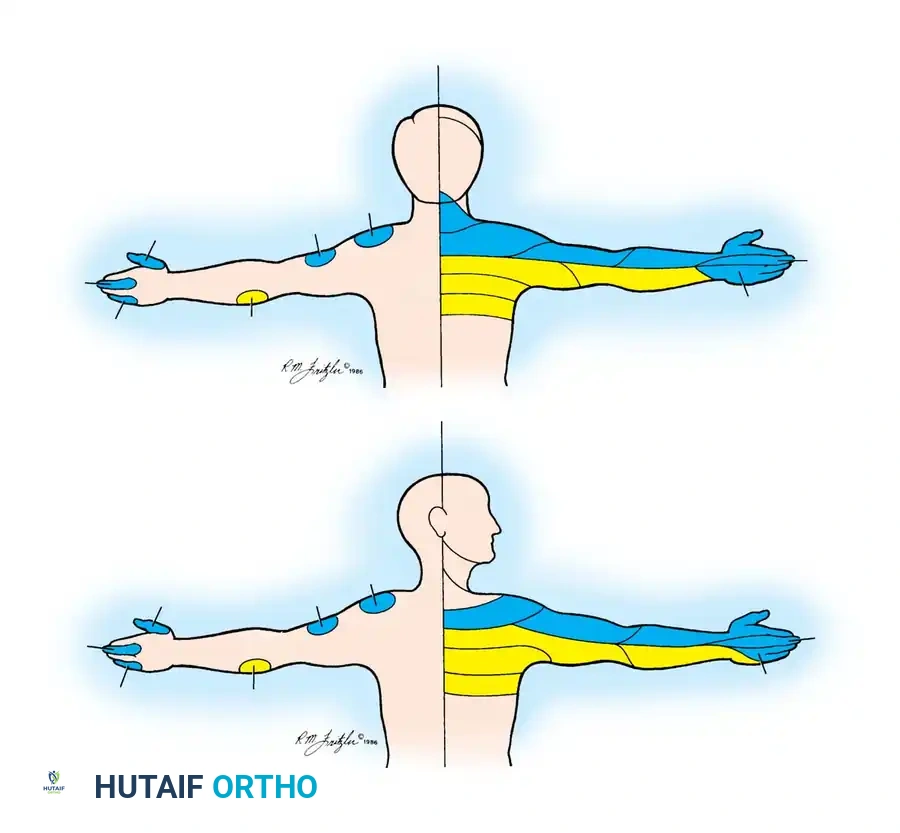
- C5 Nerve Root Compression (C4-C5 Disc):
- Sensory Deficit: Upper lateral arm and elbow.
- Motor Weakness: Deltoid (almost entirely C5) and Biceps (variable, dual C5/C6).
- Reflex Change: Biceps reflex (variable).
- C6 Nerve Root Compression (C5-C6 Disc):
- Sensory Deficit: Lateral forearm, thumb, and index finger.
- Motor Weakness: Biceps, Extensor Carpi Radialis Longus and Brevis.
- Reflex Change: Biceps and Brachioradialis reflexes diminished.
- C7 Nerve Root Compression (C6-C7 Disc):
- Sensory Deficit: Middle finger (variable due to dermatomal overlap).
- Motor Weakness: Triceps, Wrist flexors (Flexor Carpi Radialis), Finger extensors (Extensor Digitorum Communis).
- Reflex Change: Triceps reflex diminished.
- C8 Nerve Root Compression (C7-T1 Disc):
- Sensory Deficit: Ring finger, little finger, and ulnar border of the palm.
- Motor Weakness: Interossei, Finger flexors (variable), Flexor Carpi Ulnaris.
- Reflex Change: None.
- T1 Nerve Root Compression (T1-T2 Disc):
- Sensory Deficit: Medial aspect of the elbow.
- Motor Weakness: Interossei.
- Reflex Change: None.
In the classic clinical series by Odom, Finney, and Woodhall, considerable variability was noted. A diminished triceps reflex was the predominant reflex change in both C6 (56%) and C7 (64%) root compressions. Similarly, the index finger was the most common digit exhibiting hypalgesia in both C6 (68%) and C7 (70%) lesions.
Diagnostic Pitfall: Always examine the upper extremity to rule out distal peripheral nerve entrapment syndromes, such as Thoracic Outlet Syndrome (TOS), Carpal Tunnel Syndrome (CTS), and Cubital Tunnel Syndrome (CuTS), which can present with overlapping symptoms (Double Crush Syndrome).
The Shoulder Abduction Relief Sign: Described by Davidson, Dunn, and Metzmaker, this highly specific sign involves the patient actively abducting the shoulder and flexing the elbow to place the hand on top of the head. Relief of radicular pain strongly suggests cervical extradural compression, as this maneuver decreases tension on the affected nerve root.
Cervical Spondylotic Myelopathy
The signs of midline cervical spinal cord compression are unique, insidious, and varied. Pain is often poorly localized and aching; in many cases, pain is a minor complaint compared to neurological dysfunction. Patients may describe occasional sharp pain or generalized tingling radiating down the spine with neck extension (Lhermitte sign). Symptoms often include a generalized feeling of weakness, stiffness, and spasticity in the lower extremities, leading to a broad-based, unstable gait.
In patients with predominant cervical spondylosis, symptoms of vertebral artery compression may also manifest, including dizziness, drop attacks, tinnitus, intermittent visual blurring, and retro-ocular pain.
Diagnostic Imaging and Discography
While MRI is the gold standard for non-invasive evaluation of cervical disc disease, cervical discography remains a valuable adjunct for identifying the specific symptomatic disc in patients with multilevel degenerative changes being considered for surgical fusion.

🔪 Surgical Technique 39-14: Cervical Discography
- Positioning: Place the patient supine on the radiolucent procedure table.
- Preparation: Insert an angiocatheter into the upper extremity and begin intravenous antibiotic infusion (e.g., Cefazolin). Alternatively, intradiscal antibiotics can be administered during the procedure. Sedate the patient lightly (patient must remain responsive to report pain concordance). Prepare and drape the anterolateral neck sterilely.
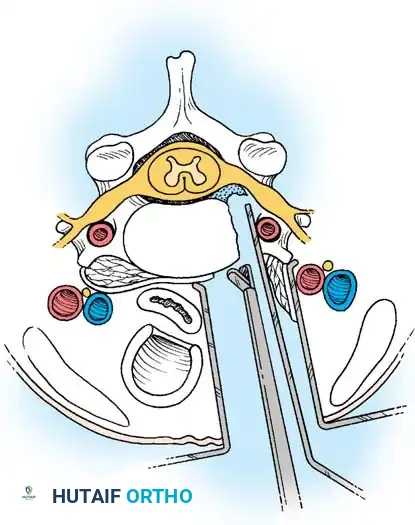
- Anterolateral Approach: Under continuous fluoroscopic imaging, identify the target intervertebral discs, ensuring aligned end plates and sharp margins. Approach the paralaryngeal area from the right. Use the index and middle fingers to gently displace the esophagus and trachea medially (to the left) and the carotid sheath laterally (to the right).
- Needle Insertion: With the opposite hand, insert a 2- or 3.5-inch spinal needle over the retracting fingers, through the skin, and into the outer anulus of the disc. Advance the needle into the center of the nucleus pulposus using orthogonal (anteroposterior and lateral) fluoroscopic guidance.
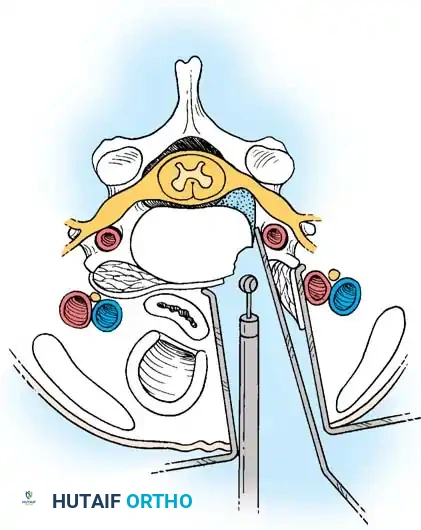
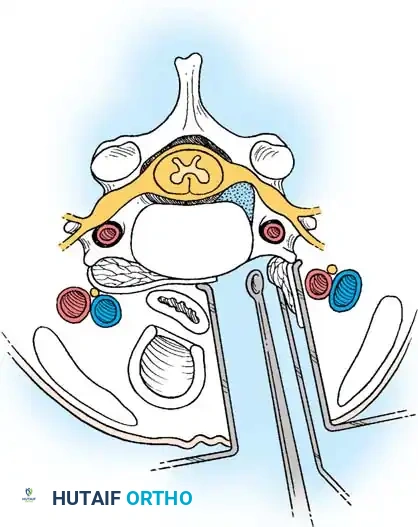
- Alternative Lateral Approach: This approach passes the needle posterior to the trachea and esophagus, potentially reducing infection risk. Position the C-arm to place the cervical spine in an oblique position for optimal foraminal exposure (adjust until end plates, disc space, and uncovertebral process are in sharp focus). Insert the needle until the tip contacts the subjacent uncovertebral process, then "walk off" anteriorly into the disc center.
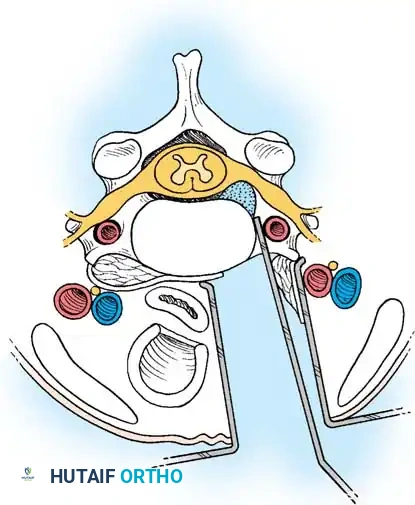
- Injection and Concordance: Inject nonionic contrast dye mixed with saline into each disc. Carefully record the patient's pain response. A positive test requires the reproduction of the patient's exact concordant clinical pain.
- Post-Procedure Imaging: Obtain immediate post-discography radiographs and a CT scan of the cervical spine to evaluate annular tears and contrast extravasation.
Surgical Management: Approaches and Indications
The classic historical approach to cervical discs was posterior via laminectomy, originally utilized as a standard exposure for extradural tumors. In 1943, Semmes and Murphey introduced the concept that cervical disc disease usually manifests as root symptoms rather than cord compression, shifting the surgical focus.
In the 1950s, pioneers like Bailey, Badgley, Cloward, Smith, and Robinson popularized the anterior approach coupled with interbody fusion. While Robertson and Hirsch demonstrated that simple anterior discectomy without fusion could yield acceptable early results, long-term data by Yamamoto et al. revealed significant drawbacks. Yamamoto noted that while 81% of soft disc hernia patients improved, only 47% of spondylosis patients improved without fusion. Furthermore, 49% developed new postoperative neck and scapular pain due to micro-instability and disc space collapse.
Current Standard of Care: Anterior Cervical Discectomy and Fusion (ACDF) is the procedure of choice when the disc is approached anteriorly. Fusion prevents disc space collapse, maintains foraminal height, prevents painful abnormal motion, and restores cervical lordosis. Conversely, posterior cervical foraminotomy is the procedure of choice for isolated, laterally located soft disc fragments where central decompression is not required.
Anterior Cervical Discectomy and Fusion (ACDF)
The anterior approach utilizes the avascular plane between the visceral neuraxis (trachea/esophagus) and the vascular neuraxis (carotid sheath).
Step 1: Exposure and Retraction
Following a transverse incision within a natural skin crease (usually left-sided to protect the recurrent laryngeal nerve, which has a more predictable course on the left), the platysma is divided. The deep cervical fascia is incised anterior to the sternocleidomastoid. Blunt dissection separates the carotid sheath laterally from the trachea and esophagus medially. The prevertebral fascia is incised to expose the longus colli muscles.
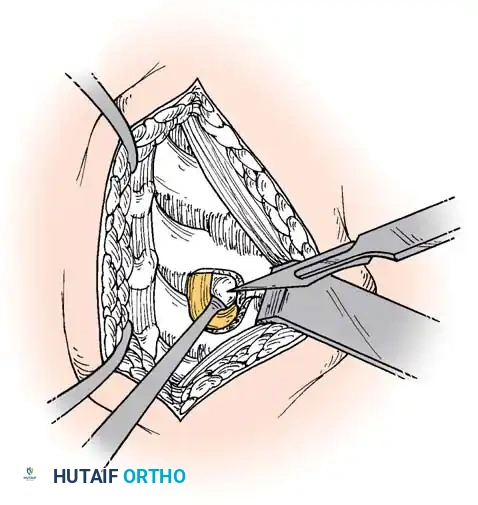
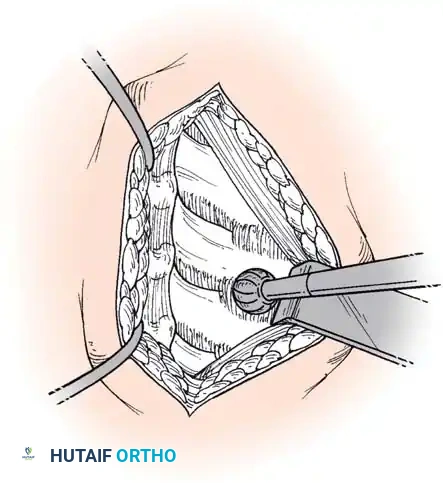
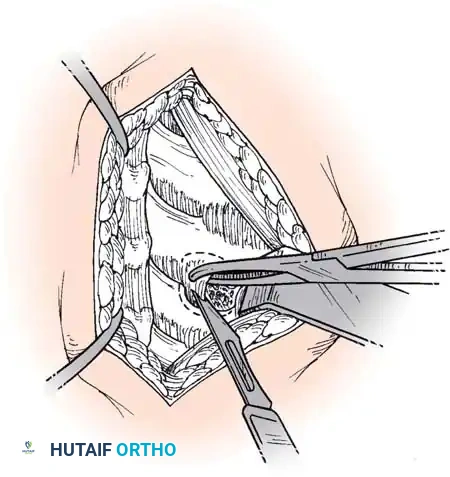
Step 2: Annulotomy and Discectomy
Self-retaining retractors are placed beneath the elevated medial borders of the longus colli. A rectangular annulotomy is performed using a #11 blade. The disc material is systematically removed using pituitary rongeurs and curettes.
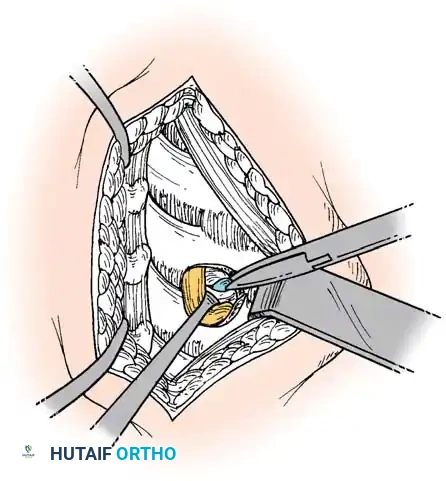
Step 3: Decompression
The posterior longitudinal ligament (PLL) is carefully identified and often resected to ensure no extruded disc fragments remain in the epidural space. High-speed burrs and Kerrison rongeurs are utilized to resect posterior osteophytes and decompress the uncinate processes bilaterally, ensuring the exiting nerve roots are entirely free.
Step 4: Endplate Preparation and Fusion
The cartilaginous endplates are meticulously decorticated using a curette or burr to expose bleeding subchondral bone, which is critical for arthrodesis. Care must be taken not to breach the structural integrity of the endplate to prevent graft subsidence.
An appropriately sized structural allograft, autograft, or synthetic cage packed with osteoinductive material is impacted into the disc space under gentle cervical traction. An anterior cervical plate is then secured with screws into the adjacent vertebral bodies to provide immediate biomechanical stability.
Posterior Cervical Foraminotomy
Foraminotomy is highly effective for unilateral radiculopathy caused by a lateral soft disc herniation or isolated foraminal stenosis, avoiding the morbidity of an anterior fusion.
Step 1: Posterior Exposure
The patient is positioned prone, often using a Mayfield head holder. A midline posterior incision is made, and the paraspinal musculature is subperiosteally elevated off the spinous processes and laminae on the symptomatic side.

📚 Medical References
- cervical disc disease, II: treatment of cervical spondylotic myelopathy in 32 cases, J Neurosurg 53:12, 1980.
- Maeda T, Saito T, Harimaya K, et al: Atlantoaxial instability in neck retraction and protrusion positions in patients with rheumatoid arthritis, Spine 29:757, 2004.
- Martel W, Page JW: Cervical vertebral erosions and subluxations in rheumatoid arthritis and ankylosing spondylitis, Arthritis Rheum 3:546, 1960.
- Matsunaga S, Ijiri K, Koga H: Results of a longer than 10-year follow-up of patients with rheumatoid arthritis treated by occipitocervical fusion, Spine 25:1749, 2000.
- Matsunaga S, Sakou T, Onishi T, et al: Prognosis of patients with upper cervical lesions caused by rheumatoid arthritis: comparison of occipitocervical fusion between C1 laminectomy and nonsurgical management, Spine 28:1581, 2003.
- Matthews JA: Atlanto-axial subluxation in rheumatoid arthritis: a fi ve-year follow-up study, Ann Rheum Dis 33:526, 1974.
- Mayfi eld FH: Cervical spondylosis: a comparison of the anterior and posterior approaches, Clin Neurosurg 13:181, 1966.
- McCarron RF, Robertson WW: Brooks fusion for atlantoaxial instability in rheumatoid arthritis, South Med J 81:474, 1988.
- McKenzie MK, Bartal E, Pay NT: A hyperextension injury of the thoracic spine in association with diffuse idiopathic skeletal hyperostosis, Orthopedics 14:895, 1991.
- McLaren AC, Bailey SI: Cauda equina syndrome: a complication of lumbar discectomy, Clin Orthop Relat Res 204:143, 1986.
- McMaster MJ: Osteotomy of the cervical spine in ankylosing spondylitis, J Bone Joint Surg 79B:197, 1997.
- McMaster PE: Osteotomy of the spine for fi xed fl exion deformity, J Bone Joint Surg 44A:1207, 1962.
- Menezes AH, Van Gilder JC, Graf CJ, et al: Craniocervical abnormalities: a comprehensive surgical approach, J Neurosurg 53:444, 1980.
- Moskovich R, Crockard HA, Shott S, et al: Occipitocervical stabilization for myelopathy in patients with rheumatoid arthritis: implications of not bone-grafting, J Bone Joint Surg 82A:349, 2000.
- Moskowitz RW, Ziv I, Denko CW, et al: Spondylosis in sand rats: a model of intervertebral disc degeneration and hyperostosis, J Orthop Res 8:401, 1990.
- Neva MN, Kaarela K, Kauppi M: Prevalence of radiological changes in the cervical spine—a cross-sectional study after 20 years from presentation of rheumatoid arthritis, J Rheumatol 27:90, 2000.
- O’Brien MF, Casey AT, Crockard A, et al: Histology of the craniocervical junction in chronic rheumatoid arthritis: a clinicopathologic analysis of 33 operative cases, Spine 27:2245, 2002.
- Oda T, Fujiwara K, Yonenobu K, et al: Natural course of cervical spine lesions in rheumatoid arthritis, Spine 20:1128, 1995.
- Olerud C, Larsson BE, Rodriguez M: Subaxial cervical spine subluxation in rheumatoid arthritis: a retrospective analysis of 16 operated patients after 1-5 years, Acta Orthop Scand 68:109, 1997.
- Ono K, Ota H, Tada K, et al: Cervical myelopathy secondary to multiple spondylotic protrusions: a clinicopathologic study, Spine 2:109, 1977.
- Oostveen JC, Roozeboom AR, van de Laar MA, et al: Functional turbo spin echo magnetic resonance imaging versus tomography for evaluating cervical spine involvement in rheumatoid arthritis, Spine 23:1237, 1998.
- Paley D, Schwartz M, Cooper P, et al: Fractures of the spine in diffuse idiopathic skeletal hyperostosis, Clin Orthop Relat Res 267, 1991.
- Peppelman WC, Kraus DR, Donaldson WF III, et al: Cervical spine surgery in rheumatoid arthritis: improvement of neurologic defi cit after cervical spine fusion, Spine 18:2375, 1993.
- Puttlitz CM, Goel VK, Clark CR, et al: Biomechanical rationale for the pathology of rheumatoid arthritis in the craniovertebral junction, Spine 25:1607, 2000.
- Ranawat CS, O’Leary P, Pellicci P, et al: Cervical spine fusion in rheumatoid arthritis, J Bone Joint Surg 61A:1003, 1979.
- Rawlins BA, Girardi FP, Boachie-Adjei O: Rheumatoid arthritis of the cervical spine, Rheum Dis Clin North Am 24:55, 1998.
- Redlund-Johnell I, Pettersson H: Radiographic measurements of the cranio-vertebral region, designed for evaluation of abnormalities in rheumatoid arthritis, Acta Radiol Diagn Stockh 25:23, 1984.
- Reijnierse M, Breedveld FC, Kroon HM, et al: Are magnetic resonance fl exion views useful in evaluating the cervical spine of patients with rheumatoid arthritis? Skeletal Radiol 29:85, 2000.
- Reiter MF, Boden SD: Infl ammatory disorders of the cervical spine, Spine 23:2755, 1998.
- Robinson RA, Afeiche N, Dunn EJ, et al: Cervical spondylotic myelopathy: etiology and treatment concepts, Spine 2:89, 1977.
- Sachs B, Fraenkel J: Progressive ankylotic rigidity of the spine (spondylose rhizomélique), J Nerv Ment Dis 27:1, 1900.
- Sandhu FA, Pait TG, Benzel E, et al: Occipitocervical fusion for rheumatoid arthritis using the inside-outside stabilization technique, Spine 28:414, 2003.
- Santavirta S, Sandelin J, Slatis P: Posterior atlanto-axial subluxation in rheumatoid arthritis, Acta Orthop Scand 56:298, 1985.
- Santavirta S, Slatis P, Kankaanpaa U, et al: Treatment of the cervical spine in rheumatoid arthritis, J Bone Joint Surg 70A:658, 1988.
- Slatis P, Santavirta S, Sandelin J, et al: Cranial subluxation of the odontoid process in rheumatoid arthritis, J Bone Joint Surg 71A:189, 1989.
- Smith HP, Challa VR, Alexander E Jr: Odontoid compression of the brain stem in a patient with rheumatoid arthritis: case report, J Neurosurg 53:841, 1980.
- Smith-Petersen MN, Larson CB, Aufranc OE: Osteotomy of the spine for correction of fl exion deformity in rheumatoid spondylitis, J Bone Joint Surg 27:1, 1945.
- Styblo K, Bossers GT, Slot GH: Osteotomy for kyphosis in ankylosing spondylitis, Acta Orthop Scand 56:294, 1985.
- Suda Y, Saitou M, Shioda M, et al: Cervical laminoplasty for subaxial lesion in rheumatoid arthritis, J Spinal Disord Tech 17:94, 2004.
- Sunahara N, Matsunaga S, Mori T, et al: Clinical course of conservatively managed rheumatoid arthritis patients with myelopathy, Spine 22:2603, 1997.
- Thomas WH: Surgical management of the rheumatoid cervical spine, Orthop Clin North Am 6:793, 1975.
- Thomasen E: Vertebral osteotomy for correction of kyphosis in ankylosing spondylitis, Clin Orthop Relat Res 194:142, 1985.
- Tsuji H: Laminoplasty for patients with compressive myelopathy due to so-called spinal canal stenosis in cervical and thoracic regions, Spine 7:28, 1982.
- Veidlinger OF, Colwill JC, Smyth HS, et al: Cervical myelopathy and its relationship to cervical stenosis, Spine 6:550, 1981.
- Weinstein PR, Karpman RR, Gall EP, et al: Spinal cord injury, spinal fracture, and spinal stenosis in ankylosing spondylitis, J Neurosurg 57:609, 1982.
- Wilson MJ, Turkell JH: Multiple spinal wedge osteotomy: its use in a case of Marie-Strumpell spondylitis, Am J Surg 77:777, 1949.
- Wilson PD: Surgical reconstruction of the arthritic cripple, Med Clin North Am 21:1623, 1937.
- Wilson PD, Osgood RB: Reconstructive surgery in chronic arthritis, N Engl J Med 209:117, 1933.
- Winfi eld J, Cooke D, Brook AS, et al: A prospective study of the radiological changes in the cervical spine in early rheumatoid disease, Ann Rheum Dis 40:109, 1981.
- Yonezawa T, Tsuji H, Matsui H, et al: Subaxial lesions in rheumatoid arthritis: radiographic factors suggestive of lower cervical myelopathy, Spine 20:208, 1995.
- Zanasi R, Fioretta G, Rotolo F, et al: “Open door” operation to raise the vertebral arch in myelopathy due to cervical spondylosis, Ital J Orthop Traumatol 10:21, 1984.
- Zhang Z, Yin H, Yang K, et al: Anterior intervertebral disc excision and bone grafting in cervical spondylotic myelopathy, Spine 8:16, 1983.
- Zeidman SM, Ducker TB, Raycroft J: Trends and complications in cervical spine surgery: 1989-1993, J Spinal Disord 10:523, 1997.
- Zigler JE, Capen DA, Rothman SL: Spinal disease in the aged, Clin Orthop Relat Res 316:70, 1995.
- Ankylosing Spondylitis Ahn NU, Ahn UM, Nallamshetty L, et al: Cauda equina syndrome in ankylosing spondylitis (the CES-AS syndrome): meta-analysis of outcomes after medical and surgical treatments, J Spinal Disord 14:427, 2001.
- Biasi D, Carletto A, Caramaschi P, et al: Effi cacy of methotrexate in the treatment of ankylosing spondylitis: a three-year open study, Clin Rheumatol 19:114, 2000.
- Bradford DS, Tribus CB: Vertebral column resection for the treatment of rigid coronal decompensation, Spine 22:1590, 1997.
- Brigham CD: Ankylosing spondylitis and seronegative spondyloarthropathies. In The Cervical Spine Research Society, Editorial Committee: The cervical spine, 3rd ed, Philadelphia, 1998, Lippincott-Raven. Broom MJ, Raycroft JF: Complications of fractures of the cervical spine in ankylosing spondylitis, Spine 13:763, 1988.
- Calabro JJ, Maltz BA: Current concepts: ankylosing spondylitis, N Engl J Med 282:606, 1970.
- Chang KW, Chen YY, Lin CC, et al:
You Might Also Like