Comprehensive Introduction and Patho-Epidemiology
Tarsal coalitions represent a fundamental failure of mesenchymal segmentation during embryonic development, rather than a de novo fusion of previously distinct osseous structures. During the fetal period, the primitive mesenchymal anlage of the foot normally undergoes a process of programmed apoptosis and cavitation to form distinct synovial joint spaces. When this process is arrested or incomplete, it results in abnormal fibrous (syndesmosis), cartilaginous (synchondrosis), or osseous (synostosis) connections between adjacent tarsal bones. The calcaneonavicular coalition is one of the two most prevalent forms of tarsal coalition, sharing epidemiological dominance with talocalcaneal (subtalar) coalitions, and together they account for approximately 90% of all such anomalies. The true incidence of tarsal coalitions in the general population is estimated to be between 1% and 13%, with a significant proportion remaining asymptomatic throughout the patient's life. Bilateral involvement is remarkably common, observed in 50% to 60% of cases, necessitating a high index of suspicion and bilateral radiographic evaluation even in unilaterally symptomatic patients.
The clinical presentation of a calcaneonavicular coalition is intimately tied to the physiological ossification timeline of the pediatric foot. Patients typically present between 8 and 14 years of age. Prior to this age, the coalition is primarily composed of flexible fibrous or cartilaginous tissue, which permits a sufficient degree of peritalar micro-motion to prevent significant mechanical stress or pain. However, as the cartilaginous bar begins to undergo endochondral ossification during early adolescence, the connection becomes increasingly rigid. This progressive ossification restricts the normal, complex coupled kinematics of the hindfoot and midfoot. As the mechanical tether solidifies, the subtalar joint is forced into a fixed valgus position, and the longitudinal arch collapses, leading to a rigid, painful flatfoot deformity.
Patients frequently present with vague, insidious-onset hindfoot or midfoot pain, exacerbated by weight-bearing activities, sports, or walking on uneven terrain. A hallmark of this condition is a history of recurrent ankle sprains, which occur because the rigid hindfoot is unable to accommodate uneven surfaces, transmitting excessive rotational forces directly to the ankle ligaments. Furthermore, the classic physical examination finding is "peroneal spasticity." It is imperative for the orthopedic surgeon to recognize that this is not a true upper motor neuron neurologic spasticity. Rather, it is a protective, reflex muscle spasm of the peroneal musculature (specifically the peroneus brevis) attempting to splint the painful, inflamed subtalar and transverse tarsal joints against irritating micromotion.
Clinical evaluation must always include a rigorous assessment of hindfoot flexibility. A rigid valgus hindfoot that fails to correct or invert during the Jack test (passive great toe extension invoking the windlass mechanism) or the double-leg heel-rise test is highly suspicious for a tarsal coalition. In a normal foot, heel rise locks the transverse tarsal joint and inverts the calcaneus; in the presence of a calcaneonavicular bar, the heel remains in fixed valgus, and the patient often experiences pain localized to the lateral aspect of the hindfoot, specifically over the sinus tarsi and the anterior process of the calcaneus.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the complex functional anatomy and biomechanics of the peritalar joint complex is essential for the successful surgical management of a calcaneonavicular coalition. The subtalar (talocalcaneal) and transverse tarsal (talonavicular and calcaneocuboid) joints do not function in isolation; rather, they operate as a highly coupled, interdependent kinematic unit often referred to in orthopedic literature as the coxa pedis or acetabulum pedis. This complex allows for the triplanar motions of pronation and supination, which are critical for shock absorption during the contact phase of gait and rigid lever arm propulsion during the terminal stance phase.
The anterior process of the calcaneus extends distally to articulate with the cuboid. The navicular lies medially and superiorly to the cuboid, articulating predominantly with the head of the talus. In a normal anatomical configuration, there is no direct articulation between the calcaneus and the navicular; they are connected only by the bifurcate ligament (specifically, its calcaneonavicular band). A calcaneonavicular bar represents an anomalous bridge spanning from the anterior process of the calcaneus (just lateral to the anterior facet of the subtalar joint) directed anteriorly, medially, and superiorly to attach to the lateral and dorsolateral margin of the navicular. This structural tether acts as a rigid osseous or cartilaginous block that obliterates the normal gliding and rotational mechanics of the transverse tarsal joint.
Biomechanically, the subtalar joint acts as a directional torque converter, translating the internal and external rotation of the tibia into pronation and supination of the foot, respectively (often modeled as a mitered hinge). When a calcaneonavicular bar is present, it rigidly tethers the lateral column (calcaneus) to the medial column (navicular). Because the navicular is functionally locked to the calcaneus, the talar head is unable to internally rotate and plantarflex over the calcaneus during the normal gait cycle. This restriction completely abolishes the normal inversion and eversion of the hindfoot. Consequently, the ground reaction forces that are normally dissipated by the flexible peritalar complex are abnormally concentrated at the adjacent joints, particularly the ankle joint superiorly and the talonavicular joint medially, leading to capsular distension, synovitis, and eventually, premature degenerative osteoarthrosis.
Surgically, the anatomy of the lateral hindfoot dictates the operative approach. The Ollier incision is utilized to access the sinus tarsi and the bar. The surgeon must be acutely aware of the superficial soft tissue structures, primarily the intermediate dorsal cutaneous nerve (a terminal branch of the superficial peroneal nerve), which courses directly over the operative field. Deep to the subcutaneous tissue, the inferior extensor retinaculum forms the roof of the sinus tarsi. The extensor digitorum brevis (EDB) muscle originates from the superolateral surface of the calcaneus, the floor of the sinus tarsi, and the interosseous talocalcaneal ligament. The EDB serves as a critical anatomical landmark and a vital surgical asset; its mobilization exposes the calcaneonavicular bar, and its rich vascular muscle belly is subsequently utilized as an interpositional graft to obliterate the dead space following resection, thereby minimizing the risk of hematoma organization and recurrent heterotopic ossification.
Exhaustive Indications and Contraindications
The decision-making process regarding the surgical resection of a calcaneonavicular bar requires a meticulous evaluation of the patient's symptoms, age, skeletal maturity, and the presence of secondary adaptive changes within the foot. Surgical intervention is not indicated for incidentally discovered, asymptomatic coalitions. A trial of conservative management is mandatory for all symptomatic patients before considering operative intervention.
Conservative modalities typically include a period of rigid immobilization (e.g., a short-leg walking cast or a controlled ankle motion [CAM] boot for 4 to 6 weeks) to acutely reduce peritalar synovitis and peroneal muscle spasm. Following immobilization, custom-molded orthotics with a medial longitudinal arch support and a medial heel wedge may be utilized to unload the lateral column and reduce stress on the coalition. Nonsteroidal anti-inflammatory drugs (NSAIDs) and physical therapy focusing on peroneal stretching and proprioceptive training are also employed. Surgical resection is indicated only when these exhaustive conservative measures fail to provide durable symptomatic relief.
The ideal candidate for a primary calcaneonavicular bar resection is an older child or young adolescent (typically between 8 and 14 years of age) who presents with persistent pain and a rigid flatfoot, but who has not yet developed irreversible degenerative arthritic changes in the talonavicular, subtalar, or calcaneocuboid joints. In this demographic, isolated resection yields excellent clinical outcomes, restoring a functional degree of peritalar motion and preventing the long-term sequelae of altered hindfoot kinematics.
Contraindications must be strictly observed to prevent catastrophic surgical failures. Advanced patient age (older adolescents or adults) is a relative contraindication if accompanied by established degenerative arthritis. In the presence of significant peritalar arthrosis, restoring motion through bar resection will paradoxically exacerbate pain by mobilizing an already arthritic joint. In such scenarios, arthrodesis is the definitive treatment. Furthermore, the presence of a concomitant, large talocalcaneal coalition (particularly involving the middle facet) often dictates a primary fusion approach, as isolated resection of the calcaneonavicular bar will not restore motion if the subtalar joint remains tethered elsewhere.
Clinical Decision Matrix: Indications and Contraindications
| Category | Specific Criteria | Clinical Rationale |
|---|---|---|
| Primary Indications | Symptomatic pain failing >3 months of conservative care (casting, orthotics, NSAIDs). | Mechanical tether causes persistent synovitis and pain that cannot be managed non-operatively. |
| Patient age 8–14 years (skeletally immature or recently mature). | Cartilaginous/early osseous bar is amenable to resection before adaptive joint remodeling occurs. | |
| Absence of advanced peritalar degenerative joint disease (DJD). | Resection restores motion; moving a healthy joint relieves pain. | |
| Absolute Contraindications | Active local or systemic infection. | Risk of deep space infection and osteomyelitis in the resected bone bed. |
| Severe peripheral vascular disease or compromised soft tissue envelope. | High risk of wound dehiscence, flap necrosis, and failure of the EDB interposition. | |
| Relative Contraindications | Advanced patient age (Adults) with established subtalar or talonavicular arthritis. | Mobilizing an arthritic joint will exacerbate pain; primary triple or subtalar arthrodesis is preferred. |
| Concomitant massive talocalcaneal (middle facet) coalition. | Resecting only the anterior tether will not restore motion; global hindfoot mechanics remain locked. | |
| Severe, rigid, uncorrectable hindfoot valgus deformity. | Bar resection alone will not correct the structural malalignment; osteotomies or fusions are required. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough and meticulous radiographic evaluation is the cornerstone of preoperative planning before proceeding with a calcaneonavicular bar resection. The standard radiographic series must include weight-bearing anteroposterior (AP), lateral, and oblique radiographs of the foot. On the lateral radiograph, the classic "anteater nose" sign may be visible, representing a tubular elongation of the anterior process of the calcaneus extending toward the navicular. However, the 45-degree internal oblique view is universally considered the gold standard plain radiograph for visualizing a calcaneonavicular bar. On this view, the coalition will appear as a solid bony bridge (synostosis) or an irregular, sclerotic pseudoarticulation with narrow, irregular radiolucent lines (synchondrosis or syndesmosis) directly between the anterior process of the calcaneus and the navicular.
Advanced cross-sectional imaging, particularly Computed Tomography (CT), has become an indispensable tool and is highly recommended for all patients undergoing surgical planning. A fine-cut CT scan with multiplanar reconstructions (axial, coronal, and sagittal) allows the surgeon to delineate the exact three-dimensional morphology, width, and depth of the coalition. Crucially, the CT scan is utilized to assess for multiple coalitions—such as a concomitant middle facet talocalcaneal coalition, which occurs in a small but significant percentage of patients and would drastically alter the surgical plan. Furthermore, CT imaging is highly sensitive for evaluating the presence of subtle degenerative arthritic changes in the talonavicular or subtalar joints, such as subchondral sclerosis, joint space narrowing, or marginal osteophytosis.
Magnetic Resonance Imaging (MRI) is generally reserved for specific clinical scenarios where plain radiographs and CT scans are equivocal, particularly in younger patients where the coalition is entirely fibrous or cartilaginous and has not yet ossified. MRI can vividly demonstrate the non-osseous tether, as well as the associated bone marrow edema adjacent to the coalition, which correlates strongly with the patient's pain generator.

FIGURE 82-79 A: Harris-Beath axial calcaneal (coalition) view utilized to identify middle facet tarsal coalitions. Note the normal middle facet on the right and an incomplete middle facet coalition on the left. This view is critical during pre-operative planning to rule out concomitant subtalar tethers.
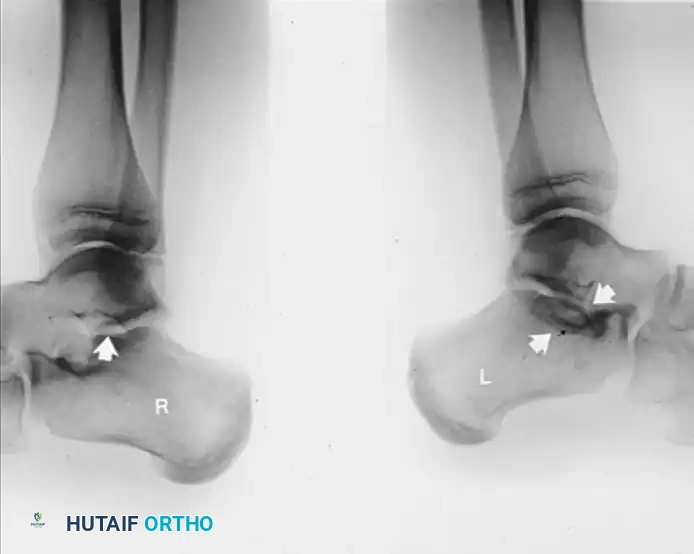
FIGURE 82-79 B: Lateral radiograph of the hindfeet of the same patient. Note the normal middle and posterior facets on the right. On the left, observe the loss of normal “space” at the middle facet, rounding of the lateral process of the talus, and a sclerotic semicircle in the calcaneus inferior to the middle facet, representing the overlap of the cortical margins of the sustentaculum and the bony bar.
Patient Positioning and Anesthesia Setup
Optimal patient positioning is critical for adequate exposure of the lateral hindfoot. The patient is typically placed in the lateral decubitus position, or alternatively, in a supine position with a large, firm bump placed under the ipsilateral hip. This hip bump internally rotates the operative leg, bringing the lateral aspect of the foot directly superior and parallel to the floor, providing excellent, unhindered access to the sinus tarsi and the calcaneocuboid joint.
A well-padded thigh or calf pneumatic tourniquet is applied to ensure a bloodless surgical field, which is absolutely necessary for precise identification of the articular margins and the neural structures. Regarding anesthesia, a regional approach is highly favored. A continuous popliteal sciatic nerve block, often combined with a saphenous nerve block, provides profound intraoperative muscle relaxation and exceptional postoperative pain control. This regional technique is typically supplemented with general anesthesia or deep intravenous sedation, depending on the patient's age, anxiety level, and the anesthesiologist's preference.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a calcaneonavicular bar resection demands meticulous soft tissue handling, precise osteotomies, and a robust interpositional strategy to prevent recurrence. The procedure is traditionally performed via the Ollier approach, which provides direct, expansile access to the lateral peritalar structures.
Exposure of the Bar (Ollier Approach)
- Incision and Superficial Dissection: The surgeon marks an Ollier incision over the lateral aspect of the hindfoot. The incision begins at the dorsolateral margin of the talonavicular joint and extends obliquely and plantarward toward the inferior tip of the lateral malleolus, typically measuring 4 to 6 centimeters in length.
- Nerve Protection: As the incision is deepened through the subcutaneous tissues, extreme caution must be exercised. It is critical to identify, mobilize, and protect the branches of the intermediate dorsal cutaneous nerve (a branch of the superficial peroneal nerve) that cross the superior aspect of the incision. Retraction of this nerve should be gentle using vessel loops to prevent traction neuritis.
- Tendon Sheath Preservation: The deep fascia is incised. The surgeon must meticulously preserve the extensor retinaculum and the sheaths of the extensor digitorum longus and peroneus tertius tendons anteriorly, as well as the peroneal tendons posteriorly. The peroneal tendons are retracted inferiorly and plantarward, while the extensor tendons are retracted superiorly and dorsally, creating a distinct surgical window over the sinus tarsi.
- Muscle Elevation (EDB Mobilization): The muscle belly of the extensor digitorum brevis (EDB) is identified at its origin. Using sharp dissection and a periosteal elevator, the EDB is raised from the confines of the sinus tarsi in a proximal-to-distal direction. The muscle is reflected distally, taking care not to devascularize it. This elevation is continued until the entire sinus tarsi, the anterior process of the calcaneus, and the lateral aspect of the navicular are fully exposed.
Identification and Resection of the Bar
- Joint Identification and Capsulotomy: The surgeon identifies the talonavicular and calcaneocuboid joints by manually rocking the forefoot-midfoot segment on the hindfoot. The calcaneonavicular bar will be visualized as a rigid structural bridge running from the anterior process of the calcaneus anteriorly and medially to the dorsolateral margin of the navicular. If the exact location of the articular margins of the calcaneocuboid or talonavicular joints is visually obscured by capsular tissue or osteophytes, the surgeon should perform conservative capsulotomies of these joints. Opening the capsules just enough to definitively identify the gleaming white articular cartilage is crucial to avoid iatrogenic joint violation during the osteotomy.

FIGURE 82-77 A: Diagrammatic representation of the calcaneonavicular tarsal coalition prior to surgical resection. Note the bridging osseous tether obliterating the normal interval between the anterior calcaneal process and the navicular.
- Retraction and Osteotomy Preparation: Small, right-angled Hohmann retractors or Chandler retractors are placed carefully around the dorsal and plantar waist of the bar. This step is vital to protect the surrounding deep soft tissues, including the underlying talar head and the medial neurovascular structures, and to improve direct visualization of the coalition.
- Execution of the Calcaneal Cut: At the calcaneal origin of the bar (proximal aspect), a 1/2-inch or 3/4-inch straight osteotome is placed parallel to the floor of the sinus tarsi. The surgeon impacts the osteotome, cutting up to, but not completely through, the medial cortex of the bar to maintain stability for the subsequent cuts.

FIGURE 82-78 A: Initial positioning of the osteotome for resection of the calcaneonavicular tarsal coalition. The blade is positioned at the calcaneal origin, parallel to the sinus tarsi floor.
- Direction of the Navicular Cut: The second osteotomy is directed at the upper, navicular insertion of the bar. The osteotome is placed at the dorsolateral aspect of the navicular and directed medially, plantarward, and obliquely at an angle of approximately 30 degrees from the vertical plane. This specific trajectory is paramount; it ensures the cut safely excises the bar without violating the adjacent articular surfaces of the talonavicular joint medially or the calcaneocuboid joint distally.

FIGURE 82-78 B: Direction of the osteotome. Note the oblique, plantarward trajectory designed to safely excise the bar without violating the adjacent articular surfaces.
- Fracture and Excision of the Bar: Once the dorsal and proximal cuts are made, the osteotome is placed back into the inferior/calcaneal cut. The surgeon gently levers the instrument to fracture the bar through its remaining intact medial cortex. The resulting rectangular or trapezoidal piece of bone is removed en bloc with a rongeur or Kocher clamp.
- Debridement and Contouring: The remaining medial cortical margins and any sharp osseous spikes are meticulously smoothed using a Luer rongeur or a high-speed motorized burr. The surgical rationale for this specific geometric block resection is to maximize the volume of bone removed while minimizing the chance of iatrogenic damage to the anterior facet of the subtalar joint or the inferior aspect of the head and neck of the talus.
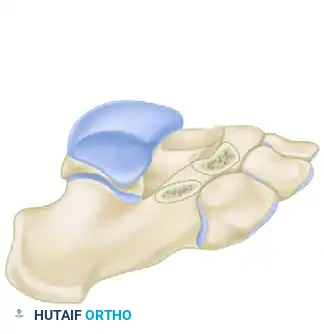
FIGURE 82-78 C: The surgical site after complete resection of the bony bar, demonstrating the resulting rectangular defect and the exposed underlying structures.
Verification of Resection and Interposition Technique
Generous resection of the bar is absolutely mandatory to prevent recurrence. The most common surgical error leading to clinical failure is removing an inadequate amount of bone. We strongly recommend obtaining a lateral oblique radiographic examination on the operating table (using fluoroscopy) immediately after resection to objectively confirm adequate removal. Typically, a 1.5- to 2.5-cm segment of the bar must be removed to create a sufficient gap. An excellent anatomic landmark confirming adequate excision is the visualization of the lateral fourth of the articular surface of the talar head, which should be left uncovered by the navicular once the bar is fully excised.
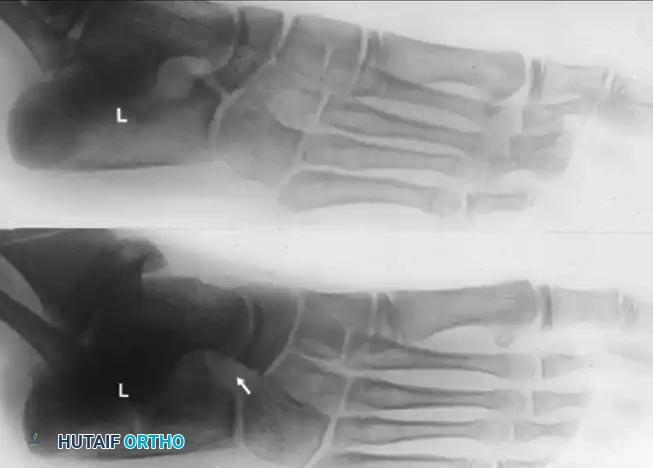
FIGURE 82-77 B: Diagrammatic representation of the surgical site after adequate resection of the calcaneonavicular bar. Note the significant gap created to prevent re-ossification.
To prevent postoperative hematoma organization and subsequent re-ossification (recurrence of the synostosis), the newly created dead space must be completely filled with vascularized tissue.
1. Suture Placement in EDB: Using a heavy absorbable suture (e.g., #1 or #0 Vicryl), the surgeon weaves a Krackow or figure-of-eight locking stitch through the proximal, tendinous margin of the mobilized extensor digitorum brevis muscle belly.
2. Muscle Transposition: The muscle is then interposed deep into the depths of the bony defect. A small, straight Keith needle is threaded with the suture ends and passed medially directly through the center of the resected space, exiting the medial skin of the midfoot (plantar to the navicular tuberosity). Pulling the suture draws the EDB muscle belly directly into the defect, acting as a biological spacer.
3. Securing the Muscle: The ends of the suture exiting the medial skin are passed through a broad felt pad or a sterile plastic button and tied firmly over the medial aspect of the foot. This tension holds the muscle securely in the defect during the initial healing phase.
4. Alternative Techniques: If the EDB is hypoplastic, insufficient, or inadvertently damaged during exposure, the use of bone wax firmly packed into the cancellous bone surfaces, often combined with Gelfoam or a free autologous fat graft harvested from the thigh or gluteal fold, is an acceptable and well-documented alternative to muscle interposition.
Hemostasis and Closure
Prior to closure, the pneumatic tourniquet is deflated. Meticulous hemostasis is secured using electrocautery. Hematoma prevention is critical, as pooled blood in the defect is the primary scaffold for heterotopic ossification. The subcutaneous tissues are approximated, and the skin is closed with absorbable subcuticular sutures or nylon, depending on surgeon preference. A well-padded, sterile dressing is applied, followed immediately by a short-leg cast in the operating room while the foot is held in a neutral, plantigrade position.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following calcaneonavicular bar resection can occur. The orthopedic surgeon must be prepared to identify and manage these issues promptly. The most significant complication is the recurrence of the coalition, which occurs in approximately 10% to 15% of cases. Recurrence is almost universally due to inadequate primary resection (failing to remove the requisite 1.5 to 2.5 cm of bone) or failure to adequately interpose vascularized tissue or bone wax, leading to hematoma ossification.
Nerve injury is another recognized complication. The intermediate dorsal cutaneous nerve is highly vulnerable during the Ollier approach. Neuropraxia due to vigorous retraction, or transection leading to a painful stump neuroma, can cause significant postoperative morbidity. Careful dissection and the use of vessel loops for gentle retraction mitigate this risk.
Continued pain despite adequate resection is typically indicative of unrecognized, pre-existing degenerative arthritis in the subtalar or talonavicular joints. In these cases, the altered kinematics caused by the longstanding coalition have already permanently damaged the articular cartilage, and restoring motion merely exacerbates the pain of the arthritic joints.
Complication Profile and Salvage Strategies
| Complication | Estimated Incidence | Etiology / Risk Factors | Prevention and Salvage Management |
|---|---|---|---|
| Recurrence of Coalition | 10% - 15% | Inadequate bone resection (<1.5 cm); Failure of EDB interposition; Hematoma organization. | Prevention: Radical resection, fluoroscopic confirmation, meticulous EDB interposition, strict hemostasis. Salvage: Revision resection (if joints are healthy) or Triple Arthrodesis. |
| Nerve Injury (Neuritis/Neuroma) | 5% - 8% | Iatrogenic traction or transection of the intermediate dorsal cutaneous nerve. | Prevention: Careful superficial dissection, gentle retraction. Salvage: Gabapentinoids, local steroid injections; surgical neuroma excision and deep muscular implantation if conservative measures fail. |
| Persistent Pain / Progressive Arthritis | 15% - 20% | Unrecognized pre-operative DJD; Older patient age at time of surgery; Concomitant coalitions. | Prevention: Rigorous pre-op CT scanning to rule |
