Biomechanical Construct Complications in Orthopaedic Trauma

Key Takeaway
Biomechanical construct complications occur when the fatigue life of an orthopaedic implant is exceeded prior to achieving solid bony union. All internal and external fixation systems will eventually fail under cyclic loading if osteogenesis is delayed. Successful management requires early recognition of hardware failure, comprehensive biological optimization, and meticulous surgical revision utilizing techniques such as exchange nailing, plate augmentation, and autologous bone grafting to restore mechanical stability and stimulate fracture healing.
Comprehensive Introduction and Patho-Epidemiology
The fundamental tenet of osteosynthesis dictates that fracture fixation represents a physiological and mechanical race between bone healing and implant failure. All implants and external fixation systems will eventually fail if bone regeneration does not occur in a timely fashion. Orthopaedic hardware is designed to provide temporary mechanical stability, offloading physiological stresses from the fracture site until the biological envelope can bridge the defect with a mature, mineralized callus. When a nonunion or delayed union occurs, the implant is subjected to prolonged, repetitive cyclic loading that inevitably exceeds its fatigue life, culminating in catastrophic biomechanical construct complications.
Understanding the complex interplay between mechanical stability and biological vitality is paramount for the orthopaedic trauma surgeon. Construct failure is rarely an isolated mechanical event; it is almost universally the clinical manifestation of an underlying biological failure, whether that be an aseptic nonunion, an occult infection, or severe avascularity of the fracture fragments. The epidemiology of construct failure varies by anatomical location and patient demographic, but it remains a formidable challenge, complicating approximately 5% to 10% of all long bone fractures. High-risk anatomical zones, such as the subtrochanteric region of the femur and the distal third of the tibia, exhibit significantly higher rates of construct failure due to the massive bending moments and precarious vascular supply inherent to these regions.
The management of broken plates, fractured intramedullary nails, or failed external fixators must meticulously address both the mechanical instability and the compromised biological environment. Never revise a failed biomechanical construct without simultaneously addressing the biological etiology of the nonunion. Simply replacing a broken implant with a larger, stiffer one without optimizing the biological environment—through meticulous debridement, decortication, bone grafting, or infection eradication—will predictably lead to a second, often more devastating, failure. The economic and psychological burden of revision osteosynthesis is immense, necessitating a "get it right the second time" approach that leverages advanced principles of materials science, biomechanics, and orthobiologics.
Patient-specific risk factors profoundly influence the patho-epidemiology of construct failure. Smoking remains the single most detrimental modifiable risk factor, severely compromising microvascular circulation and inhibiting osteogenesis. Systemic conditions such as poorly controlled diabetes mellitus, profound metabolic bone disease, chronic corticosteroid use, and the indiscriminate use of non-steroidal anti-inflammatory drugs (NSAIDs) during the acute healing phase all contribute to a hostile biological environment. Furthermore, the initial injury characteristics, particularly high-energy open fractures with extensive periosteal stripping and soft tissue devitalization, exponentially increase the risk of delayed union and subsequent implant fatigue.
Detailed Surgical Anatomy and Biomechanics
Orthopaedic implants are subjected to complex multiaxial forces during the activities of daily living, including bending, torsion, shear, and axial compression. The failure of these constructs is governed by the rigorous principles of materials science, fatigue mechanics, and the specific modulus of elasticity of the chosen alloy. The fatigue life of an orthopaedic implant is graphically represented by the S-N (Stress-Number of cycles) curve. Every material utilized in orthopaedics, whether it be Titanium alloy (Ti-6Al-4V), 316L Stainless Steel, or Cobalt-Chromium, possesses an endurance limit. This limit defines a stress level below which the material can theoretically endure an infinite number of loading cycles without failing. However, in the presence of a nonunion, the physiological loads transmitted through the implant bypass the bone and are borne entirely by the hardware, frequently exceeding this endurance limit.
Construct complications predominantly initiate at stress risers. These are architectural features of the implant, or iatrogenic alterations created during the index procedure, that concentrate mechanical forces and exponentially increase the local stress profile. Common stress risers include empty screw holes in a plate positioned directly over a fracture gap, the junction between the solid and slotted portions of an intramedullary nail, and the thread-shaft junction of locking screws. Even microscopic scratches or gouges created by drill bits or reduction forceps can act as nucleation sites for microcracks. With each physiological loading cycle—such as each step the patient takes—these microcracks propagate through the crystalline structure of the metal, eventually leading to macroscopic, catastrophic failure.
Intramedullary Nail Biomechanics and Breakage
Intramedullary nails function primarily as load-sharing devices when the fracture ends are cortically opposed. However, in the setting of a comminuted fracture or a fracture with a critical-sized defect that fails to heal, the nail transitions into a load-bearing device. When a diaphyseal fracture fails to unite, the nail is subjected to massive bending moments. This is particularly evident in the subtrochanteric region of the femur, where the mechanical axis and anatomical axis diverge, creating immense varus-producing forces, or in the proximal third of the tibia. Nail breakage typically occurs directly at the level of the nonunion, precisely where the bending moment is maximized and the working length of the implant is localized.
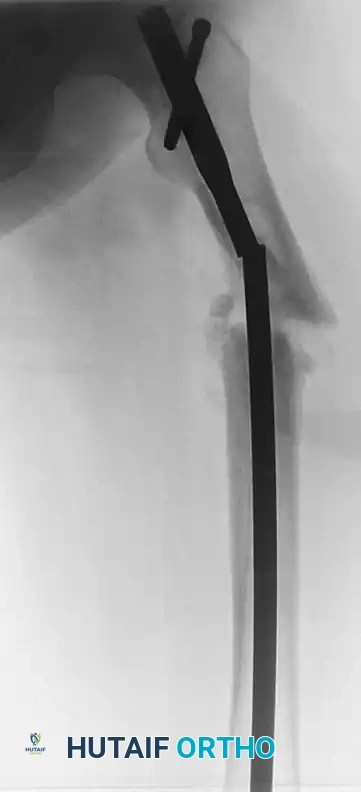
FIGURE 53-49 A: Broken femoral intramedullary nail resulted in nonunion that required bone grafting and plate fixation. The failure occurred at the zone of maximum bending stress, necessitating a comprehensive revision strategy.
Locking Screw Mechanics and "Auto-Dynamization"
Locking screws, which thread directly into the plate or nail to create a fixed-angle construct, are subjected to remarkably high shear forces at the implant-bone interface. In some specific clinical scenarios, the failure of locking screws can paradoxically benefit the healing process. If the static locking screws of an intramedullary nail break due to shear stress, the nail may be allowed to slide axially within the medullary canal. This allows physiological loads to compress the fracture site—a phenomenon known as "auto-dynamization."
FIGURE 53-49 B: Broken screws proximally and distally did not impede bony union. The shear failure of the screws allowed for axial compression, facilitating secondary bone healing.
While auto-dynamization can occasionally lead to spontaneous union by stimulating secondary bone healing via callus formation, it remains an uncontrolled and unpredictable process. It frequently results in undesirable outcomes such as loss of limb length, malrotation, or progressive angular deformity. Therefore, prophylactic, controlled dynamization—achieved by surgically removing static locking screws before implant failure occurs—is vastly preferred over waiting for the hardware to succumb to fatigue.
Exhaustive Indications and Contraindications
The decision to intervene surgically upon a failed biomechanical construct requires a nuanced understanding of the patient's physiological status, the mechanical stability of the limb, and the presence or absence of infection. Aseptic nonunion is strictly a diagnosis of exclusion; occult infection must be ruled out in every case of hardware failure.
The primary indication for revision is symptomatic hardware failure accompanied by clinical and radiographic evidence of nonunion. However, the timing and exact nature of the intervention depend heavily on the specific failure pattern. For instance, a bent but intact plate in a hypertrophic nonunion may only require stabilization to allow the robust biology to consolidate, whereas a broken nail in an atrophic nonunion demands comprehensive mechanical revision and aggressive biological augmentation.
Below is a detailed matrix outlining the indications and contraindications for various intervention strategies in the setting of construct complications.
| Clinical Scenario | Primary Indication for Intervention | Contraindications / Relative Contraindications | Preferred Revision Strategy |
|---|---|---|---|
| Hypertrophic Nonunion with Broken Plate | Mechanical instability, progressive deformity, pain. Excellent biological potential present. | Active infection (requires staged approach). Severe soft tissue compromise over the surgical site. | Hardware removal, correction of alignment, rigid re-fixation (often with an intramedullary nail or stiffer plate) to provide absolute stability. |
| Atrophic Nonunion with Broken IM Nail | Lack of biological activity, mechanical failure, pain. | Uncorrected metabolic abnormalities (e.g., severe Vitamin D deficiency, uncontrolled diabetes). | Nail extraction, over-reaming (biological stimulation), insertion of larger diameter nail, autologous bone grafting (e.g., RIA). |
| Infected Nonunion with Loose/Broken Hardware | Eradication of infection, removal of biofilm-laden implants, stabilization of dead space. | Immediate single-stage internal fixation is absolutely contraindicated. | Staged approach: Hardware removal, aggressive debridement, placement of antibiotic spacer (Masquelet technique) or external fixation. |
| Bent IM Nail (Impending Failure) | Prevention of catastrophic breakage, progressive deformity. | Asymptomatic patient with advanced, bridging callus on CT scan (observe closely). | Prophylactic exchange nailing before frank breakage occurs to avoid complex distal segment extraction. |
| Broken Locking Screws (Auto-dynamization) | Progressive shortening, malrotation, or angular deformity exceeding acceptable limits. | Asymptomatic patient, acceptable alignment, visible progression of healing callus. | Removal of broken screws if causing local irritation; otherwise, observe if alignment is maintained and union is progressing. |
Pre-Operative Planning, Templating, and Patient Positioning
The revision of a failed biomechanical construct is a highly complex, technically demanding procedure that demands meticulous preoperative planning. The surgeon must anticipate multiple failure points during the extraction process and ensure that specialized equipment is readily available in the operating theater. The diagnosis requires a high index of suspicion; patients typically report a sudden "pop" or a gradual return of pain at the fracture site after a period of postoperative comfort, often accompanied by swelling or a subjective feeling of instability.
High-quality, orthogonal radiographs are mandatory, but they are often insufficient for comprehensive planning. A fine-cut Computed Tomography (CT) scan with metal artifact reduction software is invaluable for assessing the exact location of hardware breakage, evaluating the remaining bone stock, identifying the presence of a fibrous nonunion gap, and determining the size of the medullary canal for subsequent reaming. Furthermore, a rigorous infectious workup is non-negotiable. Preoperative inflammatory markers, including C-Reactive Protein (CRP), Erythrocyte Sedimentation Rate (ESR), and a complete blood count, must be obtained. If these markers are elevated, or if there is any clinical suspicion of infection, preoperative joint or fracture site aspiration should be attempted, or the surgeon must be prepared for a staged procedure pending intraoperative tissue cultures.
Host optimization is the first step in preoperative planning. Strict smoking cessation must be enforced, ideally confirmed with cotinine levels. Nutritional deficiencies, particularly Vitamin D, Calcium, and Albumin, must be corrected to optimize the biological envelope. Endocrinological control of diabetes is essential to ensure adequate microvascular perfusion to the surgical site.
Equipment availability is a frequent pitfall in revision surgery. The surgeon must personally verify the presence of universal hardware extraction sets, broken screw removal kits (including hollow reamers and conical extraction screws), carbide drills capable of penetrating hardened alloys, metal-cutting burrs, and specialized extraction hooks for retained intramedullary nails.
Patient positioning must facilitate unimpeded fluoroscopic access in two orthogonal planes and allow for simultaneous access to bone graft harvest sites. For femoral revisions, the patient is typically positioned supine on a radiolucent flat Jackson table or a fracture table, depending on surgeon preference and the need for traction. The ipsilateral iliac crest should be prepped and draped for potential bone graft harvest. If the Reamer-Irrigator-Aspirator (RIA) system is to be used, the contralateral femur may also need to be prepped. For tibial revisions, a supine position with a radiolucent triangle under the knee is standard.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a construct revision requires patience, a systematic approach, and a deep understanding of extraction mechanics. The following details the step-by-step approach for the most challenging scenario: the extraction and revision of a broken intramedullary nail in an atrophic nonunion.
Step 1: Exposure and Proximal Hardware Removal
Utilize the previous surgical incisions, extending them proximally or distally as necessary to achieve adequate, tension-free exposure. Expose the proximal end of the nail and meticulously clear the surrounding heterotopic ossification or fibrous tissue. Remove any remaining proximal locking screws. Engage the proximal nail segment with the manufacturer-specific extraction device. This step is usually straightforward unless the internal threads of the nail are stripped or damaged by tissue ingrowth. If the threads are stripped, a conical extraction threaded device or a specialized internal expansion bolt must be utilized to gain purchase on the proximal segment.
Step 2: Distal Segment Extraction
The extraction of a retained distal segment is arguably the most technically demanding aspect of the procedure. The distal segment is often firmly incarcerated within the diaphyseal bone by endosteal overgrowth. Several techniques can be employed, escalating in invasiveness:
* Extraction Hook Technique: Pass a specialized, long extraction hook past the broken distal segment through the medullary canal. Engage the distal tip of the nail with the hook, and utilize a slotted mallet to back-slap the segment out. This requires adequate space between the nail and the endosteum.
* Ball-Tipped Guide Wire Technique: Pass a standard ball-tipped guide wire through the cannulation of the broken distal segment. Impact a small reamer, a specialized interference device, or multiple smooth wires over the ball-tipped wire to deliberately jam it within the cannulation of the nail. Once an interference fit is achieved, extract the entire unit.
* Over-Reaming Technique: If the nail is solidly ingrown, a hollow trephine reamer can be passed over the broken nail segment to cut the endosteal attachments, freeing the nail for subsequent hook extraction.
* Open Extraction: If closed methods fail, the fracture site must be opened directly. A high-speed metal-cutting burr may be used to create a small, strategic cortical window. The distal segment is then grasped directly with heavy vice grips or a bone tamp is used to retrograde the nail out of the canal.
Step 3: Canal Preparation and Biological Stimulation
Once all hardware is successfully removed, the nonunion site must be biologically revitalized. Over-ream the medullary canal by 1.5 to 2.0 mm larger than the diameter of the previous nail. This aggressive reaming serves two critical purposes: it mechanically debrides the avascular, fibrous membrane lining the canal, and it generates a rich slurry of autologous bone graft (reamings) that is inherently deposited at the fracture site to stimulate osteogenesis.
Step 4: Definitive Fixation
Insert a new, significantly larger diameter intramedullary nail to provide enhanced mechanical stability and increased fatigue resistance. Ensure the new nail engages the isthmus securely. If rotational stability remains a concern, or if the nonunion is profoundly atrophic, augment the intramedullary construct with an extramedullary compression plate. This "plate-nail construct" dramatically increases torsional and bending stiffness, creating an exceptionally rigid mechanical environment that protects the healing bone.
Step 5: Biological Augmentation
The "Diamond Concept" of fracture healing must be respected. Pack the nonunion site with autologous bone graft harvested via the RIA system or from the iliac crest. Ensure the presence of osteogenic cells, an osteoconductive scaffold, and osteoinductive growth factors. In cases of severe biological compromise, the judicious use of recombinant human bone morphogenetic protein (rhBMP-2 or rhBMP-7) may be indicated to aggressively stimulate local osteogenesis.
Complications, Incidence Rates, and Salvage Management
Despite meticulous planning and execution, the revision of a failed biomechanical construct carries a significant risk of intraoperative and postoperative complications. The altered anatomy, compromised soft tissue envelope, and the presence of avascular bone all contribute to a hostile surgical environment.
Intraoperatively, the most feared complication is iatrogenic fracture propagation or the creation of a new fracture during the aggressive extraction of retained hardware. This occurs in approximately 3% to 5% of complex extractions and requires immediate recognition and extension of the fixation construct to bypass the new fracture. Inability to remove the hardware entirely is another significant risk; stripped screw heads or cold-welded locking mechanisms may necessitate the use of metal-cutting burrs, which generate immense heat and can cause thermal necrosis of the surrounding bone if not copiously irrigated.
Postoperatively, recurrent nonunion and deep surgical site infection are the most devastating complications. Aseptic nonunion is frequently misdiagnosed; occult infections, particularly with low-virulence organisms such as Cutibacterium acnes or coagulase-negative staphylococci, are present in up to 15% of presumed "aseptic" failures. If revision osteosynthesis fails, the surgeon must pivot to salvage procedures, which may include bone transport via circular external fixation (Ilizarov method), vascularized fibular grafting, or, in extreme cases of recalcitrant infection and massive bone loss, amputation.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management Strategy |
|---|---|---|---|
| Iatrogenic Fracture during Extraction | 3% - 5% | Avoid excessive force; use trephines to clear endosteal bone; ensure adequate exposure. | Immediate extension of fixation construct (longer nail or spanning plate) to stabilize the new fracture. |
| Thermal Necrosis of Bone | 2% - 4% | Copious, continuous cold saline irrigation when using metal-cutting burrs or high-speed drills. | Resection of necrotic bone; aggressive autologous bone grafting; potential shortening of the limb. |
| Deep Surgical Site Infection | 5% - 10% | Preoperative optimization; prophylactic antibiotics; meticulous dead space management; ruling out occult infection prior to single-stage revision. | Serial debridement; removal of hardware; placement of antibiotic spacer (Masquelet); definitive fixation once infection is eradicated. |
| Recurrent Construct Failure | 5% - 15% | Respect the Diamond Concept; ensure absolute mechanical stability; address patient modifiable risk factors (smoking). | Re-evaluation of mechanics and biology; consider Ilizarov bone transport or vascularized bone grafting; evaluate for metabolic abnormalities. |
| Retained Broken Hardware | 1% - 3% | Ensure availability of comprehensive broken hardware removal sets; utilize fluoroscopy to confirm engagement. | If deeply embedded and not in the path of the new implant, it may be left in situ; otherwise, create a cortical window for direct extraction. |
Phased Post-Operative Rehabilitation Protocols
The postoperative management following the revision of a failed biomechanical construct must be highly individualized, carefully tailored to the mechanical stability of the new fixation, the anatomical location, and the biological quality of the host bone. Unlike primary fracture fixation, where standard protocols often apply, revision surgery demands a more conservative and closely monitored rehabilitation pathway.
Phase 1: Protection and Soft Tissue Healing (0-6 Weeks)
The primary focus during the initial six weeks is the protection of the new mechanical construct, the healing of the compromised soft tissue envelope, and the prevention of joint contractures. Weight-bearing is typically restricted to toe-touch (TTWB) or partial weight-bearing (PWB), utilizing assistive devices. This protects the hardware from immediate cyclic overloading while the initial, fragile cartilaginous callus begins to form. Aggressive joint mobilization of the adjacent joints (hip, knee, ankle) is instituted immediately to prevent arthrofibrosis. Both chemical (e.g., Low Molecular Weight Heparin or direct oral anticoagulants) and mechanical (intermittent pneumatic compression) deep vein thrombosis (DVT) prophylaxis are mandatory, given the prolonged immobility and the inflammatory cascade triggered by revision surgery.
Phase 2: Callus Maturation and Progressive Loading (6-12 Weeks)
At the six-week mark, a critical clinical and radiographic evaluation is performed. The surgeon must scrutinize orthogonal radiographs for the presence of early bridging callus. Clinically, the patient should exhibit diminishing pain at the fracture site upon palpation and gentle stressing. If these biological milestones are met, weight-bearing can be progressively advanced. This controlled increase in mechanical loading leverages Wolff's Law, stimulating the maturation and mineralization of the bridging callus. Physical therapy focuses on restoring muscle strength, proprioception, and normalized gait mechanics. If radiographic progression is sluggish, the surgeon may consider the application of a low-intensity pulsed ultrasound (LIPUS) bone stimulator or pulsed electromagnetic field (PEMF) therapy.
Phase 3: Consolidation and Return to Function (3-6 Months and Beyond)
Full, unrestricted weight-bearing is only permitted once solid radiographic union is unequivocally achieved, defined as bridging callus visible on at least three out of four cortices on orthogonal radiographic views, coupled with an absence of pain at the fracture site during full weight-bearing. Long-term monitoring is required, often extending up to one to two years postoperatively, to ensure the biological envelope has fully consolidated, the medullary canal has recanalized, and the new implant does not succumb to late fatigue failure. A critical surgical pitfall is permitting premature weight-bearing in an atrophic nonunion revision; even with a robust plate-nail construct, premature loading risks early catastrophic failure of the revision hardware. The mechanical construct is merely a temporary bridge; the bone must ultimately bear the physiological load.
Summary of Landmark Literature and Clinical Guidelines
The contemporary management of biomechanical construct complications is heavily informed by decades of rigorous clinical research and biomechanical studies. Evidence-based guidelines emphasize the necessity of addressing both the mechanical and biological components of construct failure.
The paradigm of biological augmentation in revision osteosynthesis was fundamentally shaped by Giannoudis et al., who introduced the "Diamond Concept" of fracture healing. This landmark framework established that successful bone regeneration requires the simultaneous presence of osteogenic cells, an osteoconductive scaffold, osteoinductive growth factors, and a stable mechanical environment. This concept remains the cornerstone of preoperative planning for any nonunion revision, dictating the use of autograft, BMAC, and rigid fixation.
In the realm of mechanical revision, the seminal work by Brinker and O'Connor highlighted the efficacy of exchange nailing for aseptic diaphyseal nonunions. Their research demonstrated that over-reaming the canal by at least 1.5 mm and inserting a larger diameter nail yields union rates exceeding 85% in aseptic femoral and tibial nonunions, provided the nonunion is not profoundly atrophic. However, for atrophic nonunions or those with significant bone loss, the literature strongly supports the addition of extramedullary plate augmentation. Studies by Attum et al. and others have shown that a plate-nail construct provides superior biomechanical stiffness compared to isolated exchange nailing, significantly reducing the risk of re-failure in mechanically hostile environments such as the subtrochanteric femur.
Furthermore, the stringent requirement to rule out infection prior to revision is supported by numerous studies demonstrating the high prevalence of occult infections in presumed aseptic nonunions. Guidelines from the Musculoskeletal Infection Society (MSIS) and the Orthopaedic Trauma Association (OTA) mandate the intraoperative collection of at least three to five distinct tissue samples for aerobic, anaerobic, and fungal cultures during any revision procedure. The integration of these landmark principles ensures that the orthopaedic surgeon approaches construct complications with a comprehensive, evidence-based strategy, maximizing the probability of successful salvage and functional restoration.
