Benign Tumors of the Hand: Diagnosis, Staging, and Surgical Management

Key Takeaway
Benign tumors of the hand require meticulous clinical evaluation, appropriate imaging, and precise surgical execution to minimize recurrence and preserve hand function. While history and plain radiographs often suffice for diagnosis, aggressive lesions necessitate advanced MRI or CT staging. Treatment predominantly involves marginal or intralesional excision, with careful adherence to oncologic principles and preservation of critical neurovascular structures.
INTRODUCTION TO HAND ONCOLOGY
The evaluation and management of tumors in the hand and wrist demand a profound understanding of complex regional anatomy, biomechanics, and oncologic principles. Because the hand is composed of tightly packed, functionally critical structures within small anatomical compartments, even histologically benign lesions can cause significant morbidity through mechanical compression, structural weakening, or neurovascular compromise.
Usually, a thorough history, meticulous physical examination, and high-quality plain radiographs are sufficient to adequately determine the diagnosis and formulate an appropriate treatment plan for benign-appearing tumors. However, if a more aggressive process is suspected—evidenced by intractable pain, rapid growth, severe inflammation, a mass >5 cm, or radiographic bony destruction—further diagnostic and staging studies are strictly warranted before any biopsy or definitive surgical intervention.
DIAGNOSTIC PATHWAY AND STAGING
Imaging Modalities
Local imaging studies are paramount for surgical planning, defining the anatomical extent of the lesion, and assessing compartmental boundaries.
* Plain Radiographs: The mandatory first step. Evaluates for osseous involvement, cortical scalloping, matrix calcification (e.g., stippled calcification in cartilaginous tumors), and pathologic fractures.
* Magnetic Resonance Imaging (MRI): The gold standard for soft tissue tumors. It delineates the tumor's relationship to tendons, neurovascular bundles, and joint capsules. MRI is highly sensitive for identifying the fluid-filled levels of an aneurysmal bone cyst (ABC) or the specific signal characteristics of a lipoma (isointense to subcutaneous fat).
* Computed Tomography (CT): Superior for evaluating cortical integrity, subtle matrix mineralization, and the central nidus of an osteoid osteoma.
* Systemic Staging: A metastatic workup, including a chest CT, is indicated for most malignant lesions or aggressive benign tumors (e.g., Giant Cell Tumor of Bone) with a known propensity for pulmonary metastasis.
Principles of Biopsy in the Hand
Generally, hand tumors are treated surgically with primary excision. Biopsy is rarely indicated for classic benign lesions because complete marginal excision serves as both an excisional biopsy and definitive treatment, providing the entire specimen for histopathologic analysis.
Surgical Warning: Incisional biopsy is strictly advised if a malignant sarcoma is suspected, or if the morbidity of surgical excision outweighs the morbidity caused by the tumor itself (e.g., complex intraneural tumors). Biopsy incisions must be made longitudinally and placed directly over the tumor mass so that the entire biopsy tract can be excised en bloc during definitive surgery.
Oncologic Staging Systems
Orthopedic oncology relies heavily on the Enneking staging systems to guide surgical margins.
Enneking Classification of Benign Tumors:
* Stage 1 (Latent): Static or healing; well-marginated (e.g., non-ossifying fibroma).
* Stage 2 (Active): Growing, symptomatic, bounded by natural barriers (e.g., aneurysmal bone cyst).
* Stage 3 (Aggressive): Rapidly growing, breaching natural barriers, high recurrence rate (e.g., Giant Cell Tumor of Bone).
Enneking Classification of Surgical Margins:
* Intracapsular: Piecemeal debulking or curettage within the tumor capsule. Leaves macroscopic disease.
* Marginal: "Shelling out" the tumor en bloc through the pseudocapsule or reactive zone. Leaves microscopic disease (satellite nodules).
* Wide: Intracompartmental en bloc excision with a continuous cuff of normal healthy tissue.
* Radical: Extracompartmental en bloc excision, removing the entire anatomical compartment.
SOFT TISSUE TUMORS OF THE HAND
Adipocytic Tumors
Lipomas
Lipomas are the most common solid cellular tumors of the hand. They typically present as painless, slow-growing masses. Because lipomas project through spaces of least resistance, deep palmar space lesions tend to present distally between the fingers and thumb, driven by the unyielding overlying palmar aponeurosis. Radiographically, they may exhibit the Bufalini sign (radiolucency in the soft tissues). MRI shows a well-marginated mass isointense to fat. Treatment is marginal excision.
Infiltrating Lipomas
Occurring mostly in adults, infiltrating lipomas grow between large muscles (intermuscular) or arise between muscle fibers (intramuscular). Despite tissue infiltration, there is no malignant transformation. However, the local recurrence rate is high (up to 60%) following marginal excision.
Lipoblastomas
These are rare, benign tumors composed of immature, spindle-shaped cells occurring almost exclusively in children under 7 years of age. Absence of cellular atypia and mitosis is necessary to differentiate them from congenital liposarcomas. Surgical excision after MRI assessment yields a 14% recurrence rate.
Peripheral Nerve Sheath Tumors
Neurilemoma (Schwannoma)
The most common benign nerve tumor in the hand, typically presenting in the 4th to 6th decades. They arise from Schwann cells and grow eccentrically, pushing nerve fascicles to the periphery.
* Histology: Exhibits biphasic architecture: Antoni A pattern (hypercellular, storiform tumor cells with Verocay bodies) and Antoni B pattern (hypocellular, disorganized myxoid matrix).
* Treatment: Marginal excision (shelling out) under magnification. Recurrence is rare.
Neurofibroma
Unlike schwannomas, neurofibromas arise centrally within the nerve, infiltrating the epineurium and separating the fascicles. They can be solitary or multiple (associated with Neurofibromatosis Type 1).
* Treatment: Excision is only recommended for expendable nerves, as removal inevitably causes neurologic deficit. In NF1, there is a 15% risk of malignant peripheral nerve sheath tumor (MPNST) degeneration.
Intraneural Lipofibromas
Typically presenting in patients under 30 years old, these lesions often affect the median nerve at the wrist or palm. They infiltrate the epineurium, compressing fascicles.
Clinical Pearl: A conservative approach is paramount. If extrinsic neural compression exists, surgical decompression (e.g., carpal tunnel release) is indicated. Intraneural excision to debulk the tumor is strongly discouraged, as intraneural fibrosis will predictably increase the neural deficit. En bloc excision with nerve grafting is reserved for severely affected, non-critical digital nerves or cases of intractable pain.
Synovial and Vascular Tumors
Giant Cell Tumor of Tendon Sheath (GCTTS)
Also known as localized nodular tenosynovitis, this is the most common primary solid hand tumor. It presents as a firm, slow-growing mass on the flexor surface of the fingers. Histologically identical to pigmented villonodular synovitis (PVNS), it contains multinucleated giant cells and hemosiderin-laden macrophages. Treatment is meticulous marginal excision, though recurrence is approximately 13% due to microscopic satellite lesions.
Glomus Tumor
A hamartoma of the neuromyoarterial glomus body, responsible for thermoregulation. It classically presents as a subungual mass with a triad of symptoms: severe localized pain, point tenderness (Love's pin test), and cold intolerance. Radiographs may show scalloping of the distal phalanx. Treatment is complete excision, yielding a 1-18% recurrence rate.
BENIGN BONE TUMORS OF THE HAND
Cartilage-Forming Tumors
Enchondroma
The most common primary bone tumor of the hand, typically presenting in the 1st or 2nd decade. They arise in the medullary canal of the phalanges or metacarpals and frequently present as a pathologic fracture. Radiographs reveal a central, well-circumscribed radiolucent lesion with or without stippled calcification.
* Treatment: Following fracture healing, treatment consists of intralesional curettage. The cavity can be filled with autologous bone graft, allograft, or calcium phosphate (CaPhos) bone cement. Malignant degeneration is rare (<1%) but higher in multiple enchondromatosis (Ollier disease or Maffucci syndrome).
Osteochondroma
Rare in the hand, these cartilage-capped bony projections arise from the metaphysis. Treatment is excision at the base of the stalk. Hereditary multiple exostoses (autosomal dominant) carry a 1-25% risk of malignant degeneration to chondrosarcoma.
Bone-Forming and Cystic Lesions
Osteoid Osteoma
Presents in patients under 30 years old, often in the proximal phalanx or carpus. Classically characterized by severe night pain that is dramatically relieved by NSAIDs (due to high prostaglandin E2 levels in the nidus). Radiographs show a sclerotic lesion with a central radiolucent nidus (<1.5 cm). Treatment is precise surgical excision or radiofrequency ablation of the nidus.
Aneurysmal Bone Cyst (ABC)
A locally aggressive, blood-filled cystic lesion presenting in the 2nd decade, typically in the metacarpal metaphysis. Radiographs show an expansile, eccentric lesion. MRI confirms fluid-fluid levels. Treatment requires aggressive curettage, high-speed burring, and bone grafting.
Giant Cell Tumor of Bone (GCT)
Occurring in the 3rd to 4th decades, GCTs in the upper extremity often affect the distal radius or carpus. They are benign but locally aggressive and possess a rare tendency for benign pulmonary metastasis.
* Staging: Campanacci grading (I: well-marginated, II: thinned cortex, III: soft tissue extension).
* Treatment: Aggressive intralesional curettage with high-speed burring, chemical adjuvants (phenol, liquid nitrogen, or hydrogen peroxide), and cementation. En bloc resection is required for massive cortical destruction. A chest CT is mandatory to rule out pulmonary metastases.
SURGICAL TECHNIQUE: EXCISION OF COMPLEX PALMAR LIPOMA
The following section details the step-by-step surgical extirpation of a complex, deep palmar lipoma that has tracked distally along the path of least resistance, presenting with significant dorsal prominence.
Step 1: Preoperative Assessment and Positioning
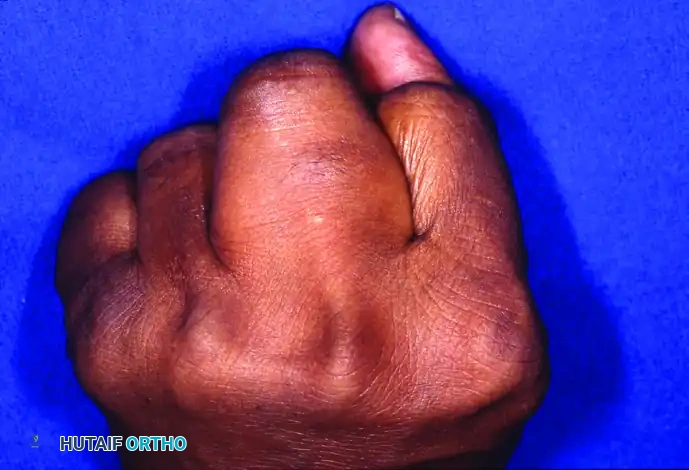
The patient presents with a substantial mass at the base of the middle finger. Due to the unyielding palmar aponeurosis, deep palmar lipomas often project dorsally, causing interference with grasp and finger adduction.
Clinical presentation demonstrating significant dorsal prominence of the middle finger when the hand is clenched into a fist.

Dorsal view with fingers extended, highlighting the asymmetric mass effect and web space widening caused by the palmar tumor projecting dorsally.
The patient is positioned supine with the arm on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Intravenous regional anesthesia (Bier block) or an axillary brachial plexus block is administered.
Step 2: Surgical Approach
A volar zig-zag (Bruner) incision is designed over the palmar aspect of the affected digit, extending proximally into the palm. This approach prevents flexion contractures and provides wide, extensile exposure of the flexor tendon sheath and neurovascular bundles.
Step 3: Dissection and Neurovascular Preservation
The skin flaps are elevated full-thickness to preserve the subdermal vascular plexus. The palmar fascia is incised. The tumor is frequently much larger than clinically apparent, exhibiting extensive lobulation.
Intraoperative view revealing a large, lobulated lipoma extensively enveloping the digital nerves and flexor tendons.
Surgical Pearl: Careful, blunt dissection using tenotomy scissors or a blunt dissector is mandatory. The lipoma often intimately surrounds the common and proper digital nerves. The nerves must be identified proximally in normal tissue and traced distally through the tumor mass using vessel loops for gentle retraction.
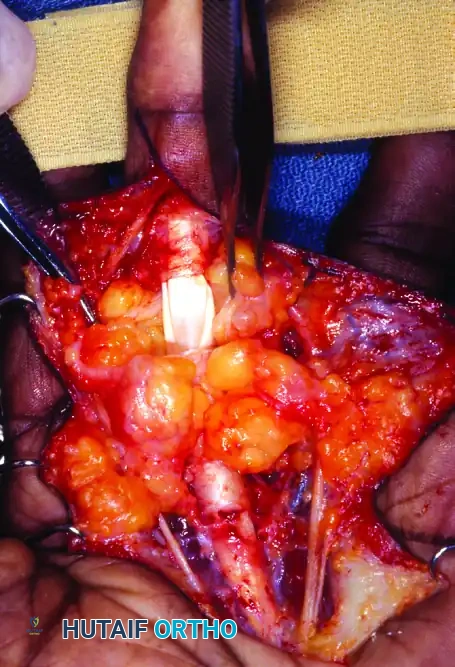
Step 4: Tumor Extirpation
The tumor is marginally excised. Because lipomas are encapsulated, they can typically be "shelled out" once the neurovascular structures are safely mobilized. The flexor tendon sheath (A1 and A2 pulleys) should be preserved unless directly infiltrated by a different pathology.

Surgical bed following complete excision of the lipoma. Note the pristine surgical sparing of the glistening white flexor tendons and the intact digital nerves.
The tourniquet is deflated prior to closure to ensure meticulous hemostasis, preventing postoperative hematoma which can lead to fibrosis and stiffness.
Step 5: Closure and Postoperative Protocol
The wound is irrigated copiously with sterile saline. The skin is closed using non-absorbable monofilament sutures (e.g., 4-0 or 5-0 Nylon) in an interrupted fashion.
Final closure of the Bruner incision, allowing for complete tumor excision while preventing linear scar contracture across the flexion creases.
Postoperative Care:
* A bulky, soft compressive dressing is applied, immobilizing the wrist in slight extension and the MCP joints in 70 degrees of flexion (intrinsic-plus position) for 3 to 5 days to allow initial wound healing.
* Early active range of motion (AROM) is initiated within the first week to prevent tendon adhesions and joint stiffness.
* Sutures are removed at 10 to 14 days.
* Strengthening exercises commence at 4 weeks postoperatively. Recurrence after complete marginal excision of a classic lipoma is exceptionally rare.
You Might Also Like