Basilar Impression: Comprehensive Surgical Management and Craniocervical Biomechanics
Key Takeaway
Basilar impression is a rare craniocervical deformity characterized by the cephalad migration of the odontoid process into the foramen magnum. This textbook-level guide covers its primary and secondary etiologies, complex clinical presentations, and precise radiographic diagnostic criteria. It provides orthopedic surgeons with step-by-step surgical protocols, including halo vest application, occipitocervical fusion, and transoral odontoidectomy, ensuring optimal neurological decompression and biomechanical stability.
BASILAR IMPRESSION: PATHOPHYSIOLOGY AND BIOMECHANICS
Basilar impression (often used synonymously with basilar invagination) is a complex and potentially life-threatening deformity of the craniocervical junction. It is characterized by the abnormal cephalad migration of the odontoid process (dens) into the foramen magnum. This architectural distortion compromises the limited space available for the brainstem and upper cervical spinal cord, leading to direct neural compression, vascular compromise, and altered cerebrospinal fluid (CSF) dynamics.
Understanding the biomechanics of the craniocervical junction is paramount. The occipitoatlantal (O-C1) and atlantoaxial (C1-C2) joints are responsible for the majority of cranial flexion/extension and axial rotation, respectively. When the structural integrity of the skull base is compromised, the axial load of the cranium drives the margins of the foramen magnum downward, effectively pushing the cervical spine upward into the cranial vault. Neurological damage ensues not only from direct anterior pressure by the odontoid but also from posterior constricting structures, circulatory insufficiency of the vertebral arteries, and the development of syringomyelia due to impaired CSF flow.
Clinical Pearl: Basilar impression often goes unrecognized in its early stages or is misdiagnosed as a posterior fossa tumor, bulbar palsy, syringomyelia, amyotrophic lateral sclerosis (ALS), or multiple sclerosis. A high index of suspicion is required when evaluating patients with vague upper motor neuron signs and a short neck.
Etiological Classification
Basilar impression is broadly categorized into primary (congenital) and secondary (acquired) forms:
- Primary (Congenital) Basilar Impression: This is a structural abnormality of the craniocervical junction present at birth. It is frequently associated with a constellation of other vertebral and neural axis defects, including atlantooccipital assimilation (fusion), Klippel-Feil syndrome, Arnold-Chiari malformation, syringomyelia, odontoid anomalies (e.g., os odontoideum), hypoplasia of the atlas, and a bifid posterior arch of C1. In many cases, these associated conditions dictate the predominant clinical symptoms.
- Secondary (Acquired) Basilar Impression: Also referred to as cranial settling, this deformity results from systemic diseases that cause osteomalacia or softening of the osseous structures at the skull base. Common etiologies include Paget disease, rheumatoid arthritis (RA), osteomalacia, rickets, osteogenesis imperfecta (particularly types III and IV), neurofibromatosis, and ankylosing spondylitis.
CLINICAL PRESENTATION AND NEUROLOGICAL EVALUATION
The clinical presentation of basilar impression is highly variable. Patients with severe radiographic deformity may remain entirely asymptomatic for decades. Symptoms typically manifest during the second and third decades of life. This delayed onset is attributed to age-related increases in ligamentous laxity, progressive craniocervical instability, and a gradually decreasing physiological tolerance to compression of the spinal cord and vertebral arteries.
Physical Examination Findings
Most symptomatic patients exhibit a characteristic physical phenotype:
* A visibly short neck.
* Asymmetry of the face or skull (plagiocephaly).
* Torticollis or restricted cervical range of motion.
* Note: These findings are non-specific and overlap significantly with other congenital vertebral anomalies.
Neurological and Vascular Symptoms
Headache in the distribution of the greater occipital nerve (C2 dermatome) is a hallmark, early complaint. DeBarros et al. classically divided the signs and symptoms into two distinct pathophysiological categories:
- Pure Basilar Impression Symptoms: Primarily motor and sensory disturbances resulting from direct medullary and upper cervical cord compression. Patients present with pyramidal tract signs, hyperreflexia, Babinski signs, and weakness or paresthesia in the extremities.
- Arnold-Chiari Associated Symptoms: Symptoms driven by cerebellar and vestibular disturbances due to tonsillar herniation. These include ataxia, dizziness, nystagmus, and lower cranial nerve palsies.
Involvement of the lower cranial nerves (Trigeminal [V], Glossopharyngeal [IX], Vagus [X], and Hypoglossal [XII]) occurs as they are stretched or compressed emerging from the medulla oblongata. Furthermore, sexual disturbances, including impotence and reduced libido, have been reported in up to 27% of patients.
Vertebral Artery Compromise
Compression or kinking of the vertebral arteries as they traverse the distorted foramen magnum is a critical source of morbidity. Bernini et al. demonstrated a significantly higher incidence of vertebral artery anomalies in patients with basilar impression and atlantooccipital fusion. Symptoms of vertebrobasilar insufficiency include dizziness, drop attacks, seizures, mental deterioration, and syncope.
Surgical Warning: Children with occipitocervical anomalies are exceptionally susceptible to vertebral artery injury and brainstem ischemia if longitudinal skull traction is applied indiscriminately. Traction can stretch the already compromised vertebral arteries, leading to intimal dissection or catastrophic thrombosis.
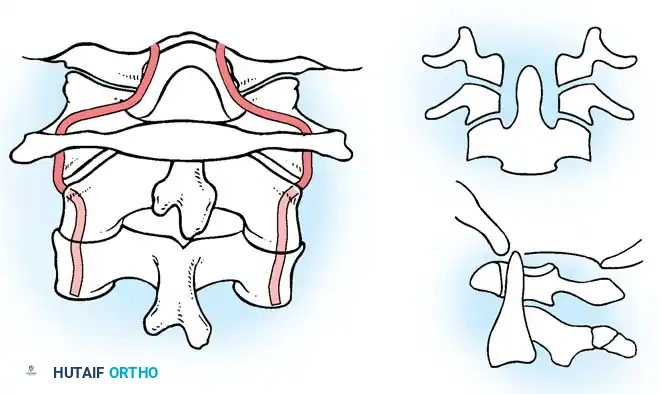
Normal position and alignment of the vertebral artery at the craniocervical junction.
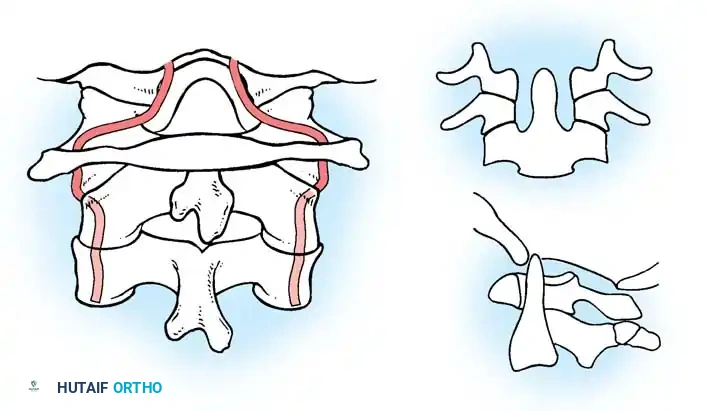
Position of the vertebral artery after cranial settling, demonstrating tortuosity and kinking.
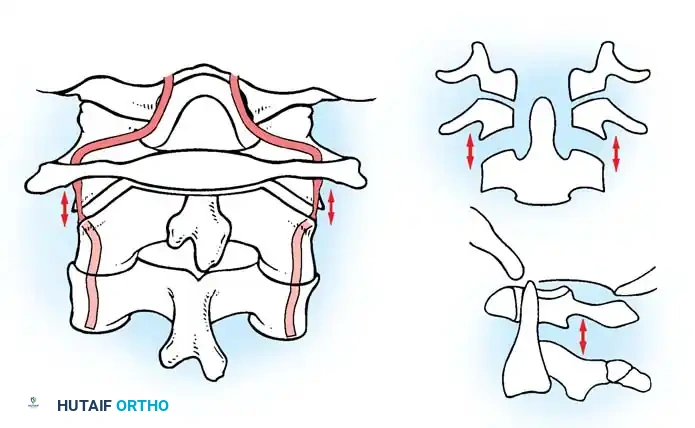
Effect of longitudinal traction on the vertebral arteries in the setting of basilar impression, highlighting the risk of ischemic injury.
RADIOGRAPHIC DIAGNOSIS AND CRITERIA
The radiographic evaluation of the craniocervical junction is notoriously difficult due to overlapping osseous structures (e.g., mastoid processes, mandible, occiput). A multimodal imaging approach—utilizing plain radiography, tomography, CT, and MRI—is essential to confirm the diagnosis and plan surgical intervention.
Lateral Radiographic Measurements
The most commonly utilized diagnostic lines are drawn on a true lateral radiograph of the skull and upper cervical spine.
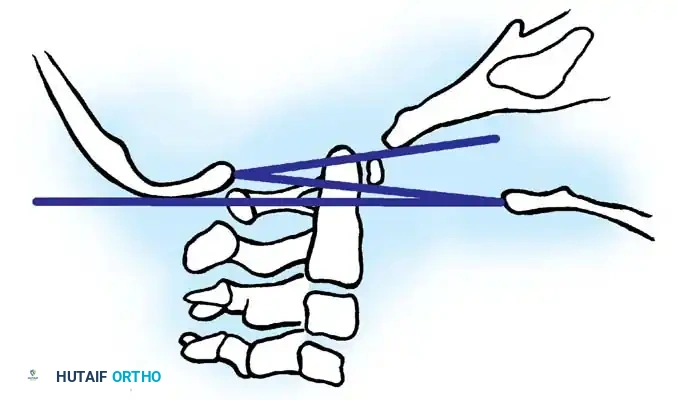
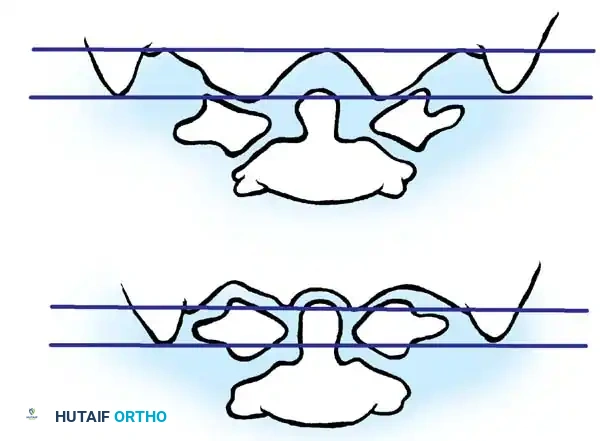
Base of the skull and upper cervical spine showing the location of the McRae, McGregor, and Chamberlain lines.
- Chamberlain Line: Drawn from the posterior edge of the hard palate to the posterior border of the foramen magnum (opisthion). Symptomatic basilar impression is suspected when the tip of the odontoid extends above this line. Pitfall: The posterior margin of the foramen magnum is often invaginated or difficult to visualize on standard radiographs.
- McGregor Line: A modification of Chamberlain's line, drawn from the upper surface of the posterior edge of the hard palate to the most caudal point of the occipital curve. This is the preferred routine screening test because the landmarks are easily identifiable. An odontoid tip projecting >4.5 mm above this line is considered abnormal.
- McRae Line: Defines the anteroposterior dimension of the foramen magnum, drawn from the anterior margin (basion) to the posterior margin (opisthion). If the tip of the odontoid remains below this line, the patient is generally asymptomatic. Protrusion above this line indicates critical encroachment into the foramen magnum.
Anteroposterior (AP) Tomographic Measurements
Because lateral lines rely on the hard palate—which can be distorted by facial anomalies or a high-arched palate—Fischgold and Metzger developed a coronal plane assessment.
Fischgold and Metzger lines. The line is drawn between the digastric grooves (A) to assess the relative height of the odontoid and atlantooccipital joints.
- Fischgold and Metzger (Digastric) Line: Drawn between the two digastric grooves (the junction of the medial aspect of the mastoid process at the base of the skull) on an AP tomogram or coronal CT reconstruction. Normally, this line passes 10.7 mm above the odontoid tip and 11.6 mm above the atlantooccipital joint. Odontoid projection above this line confirms basilar impression.
Measurements for Rheumatoid Arthritis (Adults)
In adults with secondary basilar impression (cranial settling) due to rheumatoid arthritis, specific criteria are utilized:
* Clark Station: The odontoid is divided into three equal sagittal parts. If the anterior ring of the atlas aligns with the middle third (Station II) or caudal third (Station III), basilar invagination is present.
* Redlund-Johnell Criterion: Measures the distance between the McGregor line and the midpoint of the caudal margin of the C2 vertebral body. Abnormal is <34 mm in men and <29 mm in women.
* Ranawat Criterion: Measures the distance between the center of the C2 pedicle and the transverse axis of the atlas. Abnormal is <15 mm in men and <13 mm in women.
Advanced Imaging: CT and MRI
McAfee et al. emphasize that CT and MRI are complementary. High-resolution CT with sagittal and coronal reconstructions provides unparalleled osseous detail, essential for evaluating facet joint anatomy and planning screw trajectories. MRI provides superior soft-tissue resolution, evaluating the spinal cord for myelomalacia, syringomyelia, and the exact degree of neural compression. "Functional" MRI (flexion-extension MRI) is invaluable for demonstrating dynamic spinal cord compression caused by occult instability.
PREOPERATIVE MANAGEMENT: HALO VEST APPLICATION
In cases of severe instability or when preoperative reduction is required, halo vest application is indicated. The application requires meticulous technique, particularly in pediatric patients where skull thickness is a limiting factor.
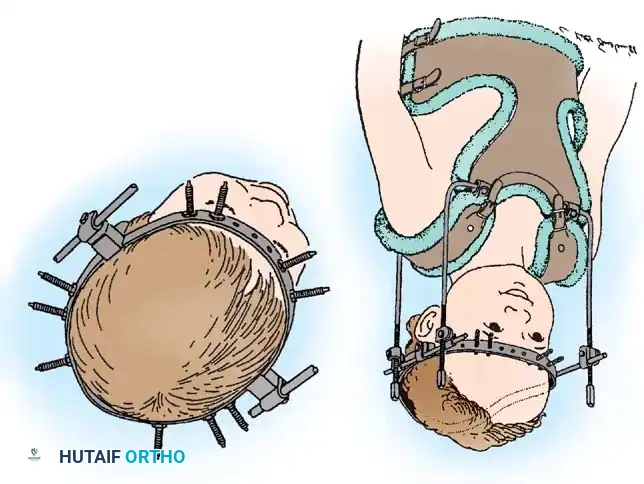
A, Ten-pin placement sites for infant halo ring attachment using a multiple-pin, low-torque technique. B, Custom halo vest and light superstructure.
Step-by-Step Halo Application Technique
- Preparation: Shave the immediate areas of pin insertion. Prepare the skin with a surgical antiseptic solution (e.g., chlorhexidine or povidone-iodine).
- Local Anesthesia: Infiltrate the skin and periosteum at the selected pin sites with a local anesthetic (e.g., 1% lidocaine with epinephrine).
- Positioning the Ring: Support the halo ring around the patient’s head using positioning pins or an assistant. The ring must sit below the maximum diameter (equator) of the skull, approximately 1 cm above the eyebrows and 1 cm above the tips of the ears.
- Anterior Pin Placement: Select the anterior pin sites in the anterolateral aspect of the skull, above the lateral two-thirds of the orbit. Surgical Pitfall: Avoid the temporalis muscle laterally (penetration causes severe pain during mastication and risks pin loosening due to thin temporal bone) and the supraorbital nerve medially.
- Posterior Pin Placement: Place the posterior pins diagonally opposed to the anterior pins, inferior to the equator of the skull.
- Tightening Sequence: Introduce the pins through the halo ring. Ensure the patient’s eyes are closed during anterior pin tightening to prevent tethering the forehead skin, which could impede eyelid closure. Tighten diagonally opposed pins simultaneously to maintain ring concentricity.
- Torque Specifications:
- Infants/Young Children: Insert 10 to 12 pins to finger tightness or a maximum of 2 inch-pounds. Use multiple pins to distribute the load over the thin pediatric calvarium.
- Older Children: Use standard 4-pin constructs at 2 to 4 inch-pounds of torque.
- Adolescents (near skeletal maturity): Torque can be increased to 6 to 8 inch-pounds, guided by preoperative CT assessment of skull thickness.
- Adults: Standard torque is 8 inch-pounds.
- Final Assembly: Secure the pins with lock nuts. Apply the polypropylene vest and attach the superstructure to the halo ring.
Aftertreatment: Pin sites must be cleansed daily with hydrogen peroxide or povidone-iodine. Pins are retightened 48 hours post-application. Complications include pin loosening, infection, bleeding, and dural puncture. If a pin loses resistance, it must be removed and relocated to an alternative site.
SURGICAL MANAGEMENT STRATEGIES
Conservative treatment (e.g., cervical collars) is universally unsuccessful in halting the progression of symptomatic basilar impression. Surgery is indicated based on the presence and progression of clinical neurological symptoms, not solely on the radiographic severity of the deformity. Once a patient becomes symptomatic, relentless progression is the natural history.
The surgical strategy is dictated by the direction of neural impingement (anterior vs. posterior) and the reducibility of the deformity.
1. Occipitocervical Fusion (Posterior Stabilization)
If the basilar impression is reducible (often assessed via preoperative traction, bearing in mind the vertebral artery risks), or if the primary pathology is dynamic instability leading to intermittent anterior impingement, stabilization in extension via an occipitocervical (O-C2 or O-C3) fusion is the procedure of choice.
- Positioning: Prone, with the head secured in a Mayfield clamp or the pre-applied halo ring. The neck is positioned in a neutral to slightly extended posture (the "military tuck" position) to optimize the space available for the cord.
- Approach: A standard posterior midline approach from the external occipital protuberance (inion) down to the subaxial cervical spine.
- Instrumentation: Modern constructs utilize rigid screw-rod systems. Occipital plates are secured with bicortical screws in the thick keel of the occiput. C1 lateral mass screws and C2 pedicle or pars screws are placed under fluoroscopic or stereotactic navigation guidance.
- Bone Grafting: Meticulous decortication of the occiput, C1 arch, and C2 lamina is performed. Autologous iliac crest bone graft (structural and cancellous) is applied to ensure a robust arthrodesis.
2. Transoral Odontoidectomy (Anterior Decompression)
If the basilar impression is fixed (irreducible) and the patient suffers from severe anterior brainstem impingement by the odontoid process, an anterior decompression is mandatory. This is typically performed via a transoral-transpharyngeal approach.
- Procedure: Working with an ENT or neurosurgical colleague, the posterior pharyngeal wall is incised vertically. The anterior arch of C1 is identified and partially resected. The base of the odontoid is drilled using a high-speed burr, and the dens is carefully amputated and removed, relieving pressure on the ventral medulla.
- Subsequent Stabilization: Because transoral odontoidectomy destroys the anterior stabilizing structures (transverse ligament, alar ligaments), it must be followed by a posterior occipitocervical fusion, either under the same anesthetic or as a staged procedure.
3. Suboccipital Craniectomy and Laminectomy (Posterior Decompression)
When the primary pathology involves posterior impingement (often seen in primary basilar impression with associated Arnold-Chiari malformations), posterior decompression is required.
- Procedure: A suboccipital craniectomy is performed, removing the posterior margin of the foramen magnum. This is combined with a laminectomy of C1 and occasionally C2.
- Dural Opening: The dura is often opened (durotomy) to inspect for fibrous bands, arachnoid adhesions, or tonsillar herniation. An expansile duraplasty using a fascial graft or synthetic substitute is performed to restore normal CSF dynamics and decompress the neural elements.
- Fusion Consideration: If the decompression destabilizes the craniocervical junction (e.g., removal of >50% of the C1/C2 facet joints), a concomitant posterior instrumented fusion is required.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
Postoperative care is critical for ensuring graft incorporation and preventing hardware failure.
* Immobilization: Patients treated with rigid internal fixation may be managed in a rigid cervical orthosis (e.g., Aspen or Miami J collar) for 6 to 12 weeks. If bone quality is poor (e.g., severe RA or osteogenesis imperfecta), postoperative halo vest immobilization may be maintained until radiographic union is confirmed.
* Monitoring: Continuous neurological monitoring in an intensive care setting is standard for the first 24-48 hours. Swallowing function must be formally evaluated, especially following transoral approaches or extensive upper cervical traction, to prevent aspiration pneumonia.
* Follow-up Imaging: Upright lateral radiographs are obtained at 2, 6, and 12 weeks to monitor alignment and hardware integrity. A CT scan at 6 months is the gold standard to confirm solid osseous fusion.
===
📚 Medical References
- Adam AM: Skull radiograph measurements of normals and patients with basilar impression: use of Landzert’s angle, Surg Radiol Anat 9:225, 1987.
- Bernini F, Elefante R, Smaltino F, et al: Angiographic study on the vertebral artery in cases of deformities of the occipitocervical joint, AJR Am J Roentgenol 107:526, 1969.
- Chamberlain WE: Basilar impression (platybasia): a bizarre developmental anomaly of the occipital bone and upper cervical spine with striking and misleading neurologic manifestations, Yale J Biol Med 11:487, 1939.
- DeBarros MC, daSilva WF, Filho HD, et al: Disturbances of sexual potency in patients with basilar impression and ArnoldChiari malformation, J Neurol Neurosurg Psychiatry 38:598, 1975.
- DeBarros MC, Farias W, Ataide L, et al: Basilar impression and Arnold-Chiari malformation: a study of 66 cases, J Neurol Neurosurg Psychiatry 31:596, 1968.
- Dickinson LD, Tuite GF, Colon GP, Papadoupoulos SM: Vertebral artery dissection related to basilar impression: case report, Neurosurgery 36:835, 1995.
- Engelbert RHH, Gerver WJM, Breslau-Siderius LJ: Spinal complications in osteogenesis imperfecta, Acta Orthop Scand 69:283, 1998.
- Fielding JW, Hensinger R, Hawkins RJ: The cervical spine. In Lovell WW, Winter RB, eds: Pediatric orthopaedics, 2nd ed, Philadelphia, 1986, Lippincott. Fischgold H, Metzger J: Etude radiotomographique de l’impression basilaire, Rev Rheum Mal Osteoartic 19:261, 1952.
- Harkey HL, Crockard HA, Stevens JM, et al: The operative management of basilar impression in osteogenesis imperfecta, Neurosurgery 27:782, 1990.
- Hayes M, Parker G, Ell J, et al: Basilar impression complicating osteogenesis imperfecta type IV: the clinical and neuroradiological fi ndings in four cases, J Neurol Neurosurg Psychiatry 66:357, 1999.
- Hensinger RN: Osseous anomalies of the craniovertebral junction, Spine 11:323, 1986.
- Hensinger RN, MacEwen GD: Congenital anomalies of the spine. In Rothman RH, Simeone FA, eds: The spine, 2nd ed, Philadelphia, 1982, Saunders. Kohno K, Sakaki S, Nakamur H, et al: Foramen magnum decompression for syringomyelia associated with basilar impression and Chiari I malformation, Neurol Med Chir 31:715, 1991.
- Kulkarni MV, Williams JC, Yeakley JW, et al: Magnetic resonance imaging in the diagnosis of the craniocervical manifestations of the mucopolysaccharidoses, Magn Reson Imaging 5:317, 1987.
- Lee CK, Weiss AB: Isolated congenital cervical block vertebrae below the axis with neurological symptoms, Spine 6:118, 1981.
- McAfee PC, Bohlman HH, Han JS, et al: Comparison of nuclear magnetic resonance imaging and computed tomography in the diagnosis of upper cervical spinal cord compression, Spine 11:295, 1986.
- McGregor M: The signifi cance of certain measurements of the skull in the diagnosis of basilar impression, Br J Radiol 21:171, 1948.
- McRae DL: The signifi cance of abnormalities of the cervical spine, AJR Am J Roentgenol 84:3, 1960.
- Raynor RB: Congenital malformations of the base of the skull. In Cervical Spine Research Society: The cervical spine, Philadelphia, 1983, Lippincott. Riew KD, Hilibrand AS, Palumbo MA, et al: Diagnosing basilar invagination in the rheumatoid patient: the reliability of radiographic criteria, J Bone Joint Surg 83A:194, 2001.
- Rush PJ, Berbrayer D, Reilly BJ: Basilar impression and osteogenesis imperfecta in a three-year-old girl: CT and MRI, Pediatr Radiol 19:142, 1989.
- Teodori JB, Painter MJ: Basilar impression in children, Pediatrics 74:1097, 1984.
- Wong V, Fung CF: Basilar impression in a child with hypochondroplasia, Pediatr Neurol 7:62, 1990.
You Might Also Like


