Comprehensive Introduction and Patho-Epidemiology
Osteochondritis dissecans (OCD) of the elbow represents a profound clinical challenge, demanding a nuanced understanding of joint biomechanics, vascular anatomy, and advanced arthroscopic techniques. Fundamentally, OCD is a progressive, focal idiopathic alteration of subchondral bone that carries a significant risk of secondary articular cartilage involvement, fragmentation, and subsequent joint degeneration. While the knee remains the most frequent anatomical site for OCD, the elbow—particularly the capitellum—is a highly prevalent location in the adolescent athletic population. As orthopedic surgeons, we frequently encounter this pathology in young athletes engaged in repetitive overhead activities, such as baseball pitchers, gymnasts, and weightlifters, typically presenting between the ages of 11 and 16 years.
It is of paramount importance to clinically differentiate capitellar OCD from Panner disease, a distinct entity that often confounds junior residents and general practitioners. Panner disease is a self-limiting osteochondrosis affecting the entire capitellar ossific nucleus, typically presenting in a younger demographic (ages 7 to 10 years). Unlike OCD, Panner disease rarely involves the articular cartilage, does not lead to loose body formation, and almost universally resolves with conservative management and time. Conversely, capitellar OCD is a localized lesion, often situated in the anterolateral aspect of the capitellum, which can progress to structural failure, subchondral collapse, and catastrophic articular cartilage delamination if left unrecognized or inadequately treated.

The epidemiology of elbow OCD is inextricably linked to the modern landscape of youth sports, characterized by early specialization and year-round participation. The repetitive valgus stress and lateral compressive forces inherent in overhead throwing and upper-extremity weight-bearing sports create a perfect storm for microtraumatic injury. The insidious onset of this condition often leads to a delayed presentation, with athletes pushing through prodromal lateral elbow pain until mechanical symptoms—such as catching, locking, or a precipitous drop in throwing velocity—manifest.
Understanding the natural history of this disease is critical for guiding our therapeutic interventions. Lesions with an intact articular surface in patients with open growth plates possess a remarkable capacity for spontaneous healing, provided the offending mechanical stresses are eliminated. However, once the subchondral bone collapses or the articular cartilage breaches, the lesion is deemed unstable. At this juncture, the biological environment of the joint is altered, and the likelihood of spontaneous resolution plummets, necessitating surgical intervention to restore joint congruity, prevent early-onset osteoarthritis, and return the athlete to their pre-injury level of function.
Detailed Surgical Anatomy and Biomechanics
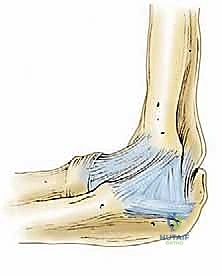
A masterful approach to elbow OCD requires an intimate, three-dimensional understanding of the joint's osseous, ligamentous, and vascular architecture. The elbow is a highly constrained, complex diarthrodial joint comprising three distinct articulations within a single synovial cavity: the ulnohumeral, the radiocapitellar, and the proximal radioulnar joints. The ulnohumeral joint acts as the primary hinge, dictating flexion and extension. Its inherent stability is derived from the highly congruent articulation between the trochlear notch of the ulna and the trochlea of the distal humerus. The axis of rotation is relatively constant, passing through the center of the trochlea and the capitellum, exiting at the anteroinferior aspect of the medial epicondyle and the center of the lateral epicondyle.
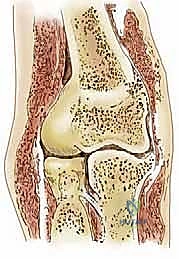
The radiocapitellar joint is the epicenter of pathology in elbow OCD. Here, the convex, hemispherical capitellum articulates with the concave fovea of the radial head. Biomechanically, the normal carrying angle of the elbow introduces an 11 to 16-degree valgus angulation. During axial loading or the acceleration phase of throwing, this angulation translates into significant, concentrated compressive forces across the lateral compartment. The radiocapitellar articulation acts as a secondary restraint to valgus stress, bearing up to 30% of the valgus load even in the presence of an intact medial ligamentous complex. When the medial structures are attenuated, this load increases exponentially, precipitating the repetitive microtrauma that drives OCD pathogenesis.
The ligamentous stabilizers of the elbow are divided into the medial and lateral collateral complexes. The Ulnar Collateral Ligament (UCL) complex, specifically its anterior bundle, is the primary restraint to valgus stress from 20 to 120 degrees of flexion. In throwing athletes, chronic attenuation or micro-tearing of the UCL leads to subtle valgus instability. This instability exacerbates the compressive forces on the radiocapitellar joint, a phenomenon often termed "valgus extension overload." Therefore, a comprehensive evaluation of a patient with capitellar OCD must always include a rigorous assessment of UCL integrity; addressing the lateral cartilage lesion without recognizing medial instability will inevitably lead to surgical failure.

Perhaps the most critical anatomical factor in the development of capitellar OCD is its tenuous intraosseous vascularity. The developing capitellar epiphysis receives its blood supply from one or two isolated trans-chondroepiphyseal vessels that enter posteriorly. These vessels function as end-arterioles, traversing the cartilaginous epiphysis without significant collateral anastomoses from the metaphyseal circulation until the patient reaches approximately 19 years of age. This anatomical bottleneck creates a vascular "watershed" zone. Repetitive lateral compression forces can easily compress, thrombose, or otherwise injure these delicate end-arterioles, leading to focal ischemia, subchondral bone necrosis, and the classic cascade of osteochondritis dissecans.
Exhaustive Indications and Contraindications
The decision-making process in the management of elbow OCD is highly nuanced, relying on a synthesis of the patient's physiological age, symptom duration, athletic aspirations, and the morphological characteristics of the lesion as defined by advanced imaging. Non-operative management is the absolute gold standard for stable lesions in skeletally immature patients. A stable lesion is characterized by an intact articular cartilage cap, no evidence of subchondral fluid on T2-weighted MRI sequences, and the absence of loose bodies. Conservative treatment demands strict cessation of the offending activity (often throwing or gymnastics) for a minimum of 3 to 6 months, accompanied by physical therapy focusing on core stability, scapular dyskinesia correction, and gradual restoration of elbow kinematics.
Surgical intervention becomes indicated when conservative measures fail, or when the initial presentation reveals an unstable lesion. Hallmarks of instability include a breach in the articular cartilage, cystic changes deep to the lesion, a high-signal fluid rim interposing between the osteochondral fragment and the native bone bed on MRI, or the presence of frank intra-articular loose bodies. Furthermore, skeletally mature patients (those with closed capitellar physes) possess a drastically reduced healing potential; thus, even seemingly stable lesions in this demographic often warrant early surgical consideration to prevent progressive joint deterioration.

Contraindications to surgical intervention, particularly joint-preserving procedures like microfracture or osteochondral autograft transfer, must be carefully respected. Advanced, diffuse degenerative joint disease with widespread chondromalacia renders focal cartilage restoration futile. Active intra-articular infection is an absolute contraindication to any elective arthroscopic procedure. Additionally, unaddressed gross ligamentous instability (such as a high-grade UCL tear) is a relative contraindication to isolated OCD treatment; the underlying biomechanical overload must be corrected concurrently or in a staged fashion to protect the cartilage repair.
| Clinical Scenario | Indication for Surgery | Contraindication for Surgery | Rationale / Management Strategy |
|---|---|---|---|
| Stable Lesion, Open Physis | Failed >6 months of strict rest | Initial presentation | High potential for spontaneous healing with offloading. |
| Unstable Lesion (Fluid on MRI) | Absolute indication | N/A | Fluid under fragment prevents bony union; requires debridement/fixation. |
| Presence of Loose Bodies | Absolute indication | N/A | Mechanical symptoms will persist; risk of further cartilage damage. |
| Closed Physis, Symptomatic | Strong relative indication | Asymptomatic incidental finding | Poor biological healing potential necessitates surgical marrow stimulation or grafting. |
| Concomitant Active Infection | N/A | Absolute contraindication | Infection must be eradicated prior to any joint-preserving procedure. |
| Diffuse Osteoarthritis | Salvage procedures only (e.g., debridement) | Focal cartilage restoration (OATS/Microfracture) | Biologic restoration will fail in a globally degenerative joint environment. |

Pre-Operative Planning, Templating, and Patient Positioning
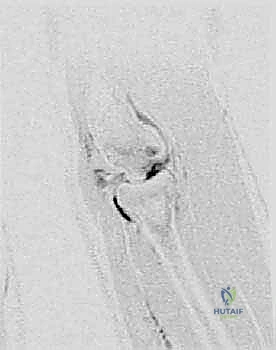
Meticulous pre-operative planning is the bedrock of a successful arthroscopic intervention for elbow OCD. The evaluation begins with high-quality, multi-planar imaging. Standard anteroposterior, lateral, and oblique radiographs are mandatory, but the 45-degree flexion AP view is particularly sensitive for profiling the anterolateral capitellum where these lesions typically reside. However, Magnetic Resonance Imaging (MRI) without contrast, utilizing high-resolution cartilage-sensitive sequences (such as T2-mapping or proton density fat-saturated sequences), is the definitive modality. MRI allows the surgeon to precisely map the lesion's dimensions, assess the integrity of the overlying cartilage, identify subchondral cyst formation, and locate elusive loose bodies residing in the olecranon fossa or posterolateral gutter.

In cases where osteochondral autograft transfer (OATS) is anticipated, pre-operative templating is essential. The surgeon must measure the exact diameter and depth of the capitellar defect on MRI to ensure that an appropriately sized graft can be harvested from the donor site (typically the lateral femoral condyle of the ipsilateral knee). If the lesion is massive or uncontained, a Computed Tomography (CT) scan with 3D reconstruction may be obtained to better appreciate the bony architecture and plan for potential structural bone grafting or complex fixation strategies.

Patient positioning for elbow arthroscopy is a matter of surgeon preference, with the lateral decubitus, prone, and supine suspended positions being the most common. In our masterclass approach, the lateral decubitus position is favored as it provides excellent access to both the anterior and posterior compartments while allowing for a stable, reproducible setup. The patient is placed in the lateral position with the operative arm supported over a padded post or suspended via an arm holder. The elbow must be free to flex and extend fully. A sterile tourniquet is applied high on the brachium.
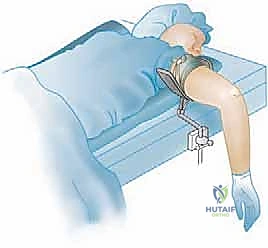
Careful marking of the anatomical landmarks—the medial and lateral epicondyles, the olecranon tip, and the radial head—is performed before joint insufflation. The ulnar nerve should be palpated and its course marked to avoid iatrogenic injury during portal placement. Joint insufflation with 20 to 30 cc of sterile saline through the soft spot (the center of the triangle formed by the lateral epicondyle, radial head, and olecranon) distends the capsule, pushing the neurovascular structures anteriorly and creating a safe working space for initial portal establishment.
Step-by-Step Surgical Approach and Fixation Technique
The arthroscopic management of elbow OCD requires a highly systematic approach, beginning with a comprehensive diagnostic arthroscopy. Standard portals include the proximal anteromedial, proximal anterolateral, and direct lateral (soft spot) portals. The proximal anteromedial portal is typically established first, located 2 cm proximal and 1 cm anterior to the medial epicondyle. This portal provides an unparalleled panoramic view of the anterior compartment, including the radiocapitellar joint. The proximal anterolateral portal is established under direct intra-articular visualization, taking meticulous care to remain anterior to the radial nerve.

Once access is achieved, the lesion is carefully probed. If the articular cartilage is intact but ballotable, and the patient is nearing skeletal maturity, retrograde drilling may be employed to stimulate revascularization without violating the articular surface. However, most operative cases involve a detached or fragmented lesion. The first step is the meticulous removal of all loose bodies, thoroughly sweeping the anterior compartment, the radiocapitellar articulation, and the posterior gutters.
For lesions that are detached but structurally intact and of sufficient size, primary fixation is the preferred technique. The fibrous tissue lining the crater base is aggressively debrided using ring curettes and motorized shavers down to bleeding subchondral bone. The osteochondral fragment is similarly debrided of fibrous tissue. The fragment is then anatomically reduced and provisionally stabilized with Kirschner wires. Definitive fixation is achieved using bioabsorbable pins, darts, or variable-pitch headless compression screws. It is imperative that the heads of any fixation devices are buried beneath the articular surface to prevent catastrophic abrasion of the opposing radial head.

When the fragment is fragmented, non-viable, or un-salvageable, the surgical strategy shifts to lesion debridement and marrow stimulation. The necrotic bone is excised, and the margins of the defect are sharply debrided to create vertical walls of healthy, stable hyaline cartilage. Microfracture is then performed using specialized, angled arthroscopic awls. The awl is advanced through the subchondral bone plate at 2 to 3 mm intervals, starting at the periphery and moving centrally. The surgeon must visualize the release of marrow fat droplets and blood into the joint space upon releasing the arthroscopic pump pressure, confirming adequate penetration into the vascularized cancellous bone. This technique relies on the formation of a "super clot" containing mesenchymal stem cells, which will eventually differentiate into fibrocartilage, filling the defect.

For large (>10 mm), uncontained lesions, or those that have failed prior marrow stimulation, Osteochondral Autograft Transfer (OATS) is the definitive reconstructive option. This technically demanding procedure involves harvesting a cylindrical plug of healthy bone and hyaline cartilage from a non-weight-bearing portion of the lateral femoral condyle. The capitellar defect is reamed to a precise diameter and depth to match the harvested graft. The graft is then delivered into the elbow via a mini-open lateral arthrotomy or through a specialized large-diameter arthroscopic cannula. The graft must be inserted perpendicular to the articular surface and seated perfectly flush with the surrounding native cartilage to restore seamless radiocapitellar kinematics.
Complications, Incidence Rates, and Salvage Management
While arthroscopic management of elbow OCD is generally highly successful, the surgeon must be acutely aware of potential complications, which can be devastating to the young athlete's career. The elbow is an unforgiving joint, densely surrounded by critical neurovascular structures and highly prone to post-operative stiffness. Meticulous surgical technique, precise portal placement, and rigorous adherence to post-operative rehabilitation protocols are essential to minimize these risks.
Neurological injury is the most feared complication in elbow arthroscopy. The radial nerve is particularly vulnerable during the establishment of the anterolateral portal and during aggressive debridement of the lateral capsule. The ulnar nerve is at risk if the anteromedial portal is placed too posteriorly or if fluid extravasation causes significant cubital tunnel compression. The medial antebrachial cutaneous nerve is frequently encountered near the anteromedial portal and can result in painful neuromas if transected.

Post-operative stiffness, or arthrofibrosis, is perhaps the most common complication, occurring in up to 10-15% of patients. The elbow capsule is highly reactive to surgical trauma and hemarthrosis. Prevention relies on meticulous hemostasis, the use of intra-articular drains in extensive procedures, and the immediate initiation of passive range of motion post-operatively. If profound stiffness develops and is refractory to aggressive physical therapy and dynamic splinting, an arthroscopic capsular release may be required as a salvage procedure, typically delayed until at least 6 months post-index surgery.

In cases of internal fixation, hardware-related complications such as pin migration, screw back-out, or localized chondrolysis from prominent implants can occur. This necessitates immediate arthroscopic hardware removal and assessment of the joint surfaces. For OATS procedures, graft subsidence, failure of graft incorporation, or donor site morbidity at the knee are recognized risks. In the catastrophic event of massive capitellar collapse or failed massive OATS grafting, salvage options are severely limited in the young patient. Procedures such as capitellar resurfacing with focal synthetic implants or, in the most extreme and rare cases of profound radiocapitellar destruction, radial head excision, are considered end-stage salvage operations that permanently alter the biomechanics of the joint.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management |
|---|---|---|---|
| Neurological Injury (Radial/Ulnar) | < 1-2% | Precise portal placement; adequate joint distension; minimize fluid extravasation. | Observation (often neuropraxia); formal nerve exploration if transection suspected. |
| Arthrofibrosis / Severe Stiffness | 5-15% | Meticulous hemostasis; early aggressive passive ROM; use of CPM if indicated. | Dynamic splinting; delayed arthroscopic capsulotomy/release. |
| Hardware Prominence / Failure | 2-5% (Fixation cases) | Bury screw heads completely; utilize bioabsorbable implants when appropriate. | Immediate arthroscopic implant removal; assess for secondary cartilage damage. |
| Graft Subsidence (OATS) | 3-8% | Precise depth measurement; achieve press-fit fixation; avoid early axial loading. | Revision grafting; capitellar resurfacing (salvage). |
| Donor Site Morbidity (Knee) | 5-10% | Harvest from extreme periphery of lateral femoral condyle; backfill donor site. | Symptomatic treatment; localized injections; rarely requires surgical intervention. |

Phased Post-Operative Rehabilitation Protocols
The surgical intervention is only the first half of the battle; a meticulously structured, phased rehabilitation protocol is equally critical to achieving an optimal outcome. The rehabilitation timeline is heavily dictated by the specific surgical procedure performed. Procedures involving marrow stimulation (microfracture) or structural grafting (OATS) require a delicate balance between protecting the healing biological tissue and preventing joint contracture.
Phase 1: Protection and Early Motion (Weeks 0-2)
Immediately post-operatively, the elbow is typically immobilized in a well-padded splint at 90 degrees of flexion for 3 to 7 days to allow for initial soft tissue healing and to manage edema. Following this brief immobilization, the transition to a hinged elbow brace is initiated. The paramount goal of Phase 1 is the restoration of early, pain-free passive range of motion (PROM) and active-assisted range of motion (AAROM). For microfracture and OATS patients, continuous passive motion (CPM) machines may be utilized to nourish the developing fibrocartilage or hyaline graft without applying shear stresses. Axial loading and valgus stress are strictly prohibited.
Phase 2: Active Motion and Early Strengthening (Weeks 3-6)
As the soft tissues heal and the joint effusion subsides, the focus shifts to achieving full active range of motion (AROM). The hinged brace is gradually unlocked and eventually discontinued. Isometric strengthening of the biceps, triceps, and forearm musculature is introduced. Scapular stabilization exercises, which are critical for overhead athletes, are aggressively pursued during this phase. It is vital to monitor the patient for any signs of increasing pain or recurrent effusion, which may indicate that the rehabilitation is progressing too rapidly and compromising the healing articular surface.
Phase 3: Advanced Strengthening and Proprioception (Weeks 7-12)
Once full, painless AROM is achieved, the protocol advances to isotonic strengthening. Concentric and eccentric exercises for the entire upper extremity kinetic chain are implemented. Plyometric exercises and advanced proprioceptive training are introduced to prepare the neuromuscular system for the demands of sport. For throwing athletes, particular attention is paid to strengthening the dynamic stabilizers of the medial elbow (flexor-pronator mass) to help offload the radiocapitellar joint during the eventual return to throwing.
Phase 4: Return to Sport and Interval Programs (Months 3-6+)
The final phase is a highly individualized, criteria-based progression back to competitive play. For patients who underwent simple debridement or loose body removal, this phase may begin as early as 8 to 10 weeks. However, for microfracture, fixation, or OATS procedures, the biological timeline dictates a delay of at least 4 to 6 months before initiating sport-specific activities. Throwing athletes must complete a formal, supervised interval throwing program, starting with short-distance, flat-ground tossing and gradually progressing to mound work and breaking pitches over several months. Clearance for full competition requires a painless elbow, full ROM, symmetrical upper extremity strength, and perfect throwing mechanics.
Summary of Landmark Literature and Clinical Guidelines
The evolution of arthroscopic management for elbow OCD is deeply rooted in robust clinical research and landmark literature. A thorough understanding of these foundational studies is essential for the academic orthopedic surgeon to practice evidence-based medicine and counsel patients effectively regarding long-term expectations.
Takahara et al. provided one of the most critical long-term natural history studies, demonstrating that patients with closed capitellar physes and advanced lesion fragmentation at the time of presentation universally experienced poor outcomes with non-operative management, inevitably progressing to early-onset osteoarthritis. This study solidified the modern clinical guideline that advanced lesions, particularly in skeletally mature adolescents, mandate surgical intervention to alter the devastating natural history of the disease.
