Knee Arthroplasty: Prosthesis Design, Biomechanics & Surgical Technique

Key Takeaway
Total knee arthroplasty (TKA) represents one of the most successful surgical interventions in modern orthopedics. This comprehensive guide details the evolution of prosthesis design, from early total condylar models to modern posterior-stabilized and constrained systems. It provides an in-depth analysis of knee biomechanics, precise surgical techniques, ligamentous balancing, and postoperative protocols, offering orthopedic residents and consultants an evidence-based framework for optimizing patient outcomes and implant survivorship.
Comprehensive Introduction and Patho-Epidemiology
Total knee arthroplasty (TKA) stands unequivocally as a cornerstone of modern orthopedic surgery and represents one of the most successful and cost-effective surgical interventions in the history of medicine. Designed to provide reliable pain relief, functional restoration, and improved quality of life for patients suffering from end-stage degenerative joint disease, TKA has seen an exponential rise in utilization globally. The epidemiological burden of knee osteoarthritis is staggering, driven by an aging population, rising obesity rates, and the expanding indications for arthroplasty in younger, more active patients. Consequently, orthopedic surgeons must possess a profound, nuanced understanding of knee biomechanics, the historical and modern evolution of prosthetic design, meticulous patient selection criteria, and exacting surgical technique to ensure long-term survivorship and optimal clinical outcomes.
The historical evolution of modern prosthesis design provides critical context for current surgical philosophies. Although numerous total knee designs predate the total condylar prosthesis conceptualized by John Insall and his contemporaries, its formal introduction in 1973 marked the definitive beginning of the modern era of TKA. This revolutionary prosthesis design allowed mechanical and materials engineering considerations to outweigh the contemporary desire to reproduce the exact anatomical kinematics of normal knee motion. Influenced heavily by the preceding ICLH (Imperial College/London Hospital) design, the total condylar prosthesis mandated the sacrifice of both the anterior and posterior cruciate ligaments, relying entirely on the articular surface geometry to maintain sagittal and coronal plane stability.
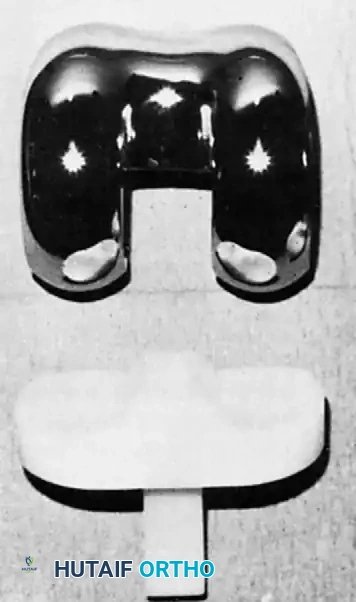
Fig. 6-1: The Total Condylar Prosthesis introduced by Insall in 1973, marking a paradigm shift in TKA survivorship.
The original cemented total condylar prosthesis dramatically reset the standard for the survivorship of total knee replacements. Landmark long-term studies, such as those by Ranawat et al., reported a remarkable prosthetic survivorship of 94% at 15-year follow-up, a figure that remains a benchmark for modern designs. The anatomical architecture of this early design included a chrome cobalt femoral component featuring a symmetrical anterior flange specifically engineered for patellar articulation. The symmetrical femoral condyles possessed a decreasing sagittal radius of curvature posteriorly and were individually convex in the coronal plane, aiming to optimize contact stresses while allowing a functional, albeit limited, range of motion.
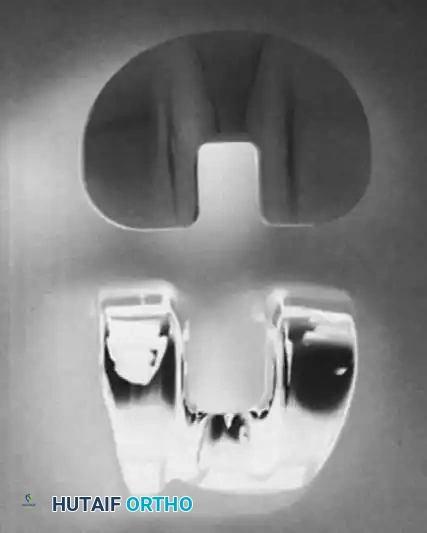
Supplementary View: Early component geometry emphasizing coronal congruency.
The double-dished articular surface of the original tibial polyethylene component was perfectly congruent with the femoral component in extension and highly congruent in the coronal plane during flexion. Translation and dislocation of the components were effectively resisted by the anterior and posterior lips of the tibial component, alongside a prominent median eminence. Furthermore, the tibial component incorporated a metaphyseal stem to resist tilting of the prosthesis during asymmetrical loading, a common occurrence in the varus or valgus knee. Originally manufactured as an all-polyethylene component, metal backing was subsequently introduced to facilitate more uniform stress transfer to the underlying cancellous metaphyseal bone, thereby mitigating the risk of polyethylene deformation and catastrophic failure.
Detailed Surgical Anatomy and Biomechanics
Understanding the intricate kinematics of the native knee is the absolute prerequisite for executing a successful arthroplasty. The knee must never be conceptualized as a simple hinge joint; rather, it exhibits a highly complex polycentric motion involving simultaneous rolling, gliding, and rotation about multiple instantaneous centers of rotation. This polycentric motion is dictated by the asymmetrical geometry of the femoral condyles, the meniscal anatomy, and the complex interplay of the collateral and cruciate ligaments. Replicating or adequately compensating for these kinematics is the primary challenge in prosthetic design.

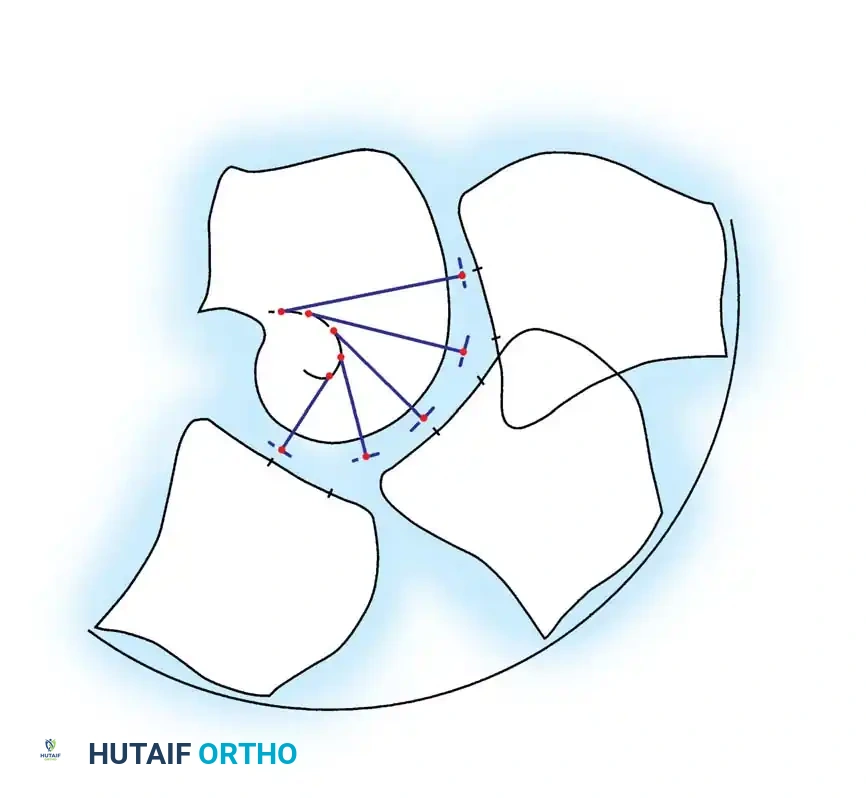
Biomechanical representation of knee kinematics, illustrating the instantaneous center of rotation and polycentric motion.
Kinematics and Femoral Rollback
During early flexion (0 to 20 degrees), the femoral condyles primarily roll posteriorly on the tibial plateau. As the degree of flexion increases, the articular motion transitions to a complex combination of rolling and gliding, eventually culminating in pure gliding at deep flexion angles. This posterior translation of the femur relative to the tibia is clinically termed femoral rollback. Rollback is biomechanically critical because it moves the tibiofemoral contact point posteriorly, thereby clearing the posterior margin of the tibia and allowing deep flexion without osseous impingement. In native anatomy, this is driven by the tensioning of the posterior cruciate ligament (PCL). In TKA, achieving rollback depends entirely on the chosen prosthetic philosophy: either retaining a functional PCL (cruciate-retaining or CR designs) or utilizing a highly engineered cam-and-post mechanism in a posterior-stabilized (PS) design.
Concurrent with the development of the cruciate-sacrificing total condylar prosthesis, the duopatellar prosthesis was developed, featuring a sagittal plane contour of the femoral component that was more anatomically shaped. Crucially, this prosthesis included the retention of the PCL. The duopatellar prosthesis subsequently evolved into the kinematic prosthesis, which dominated the arthroplasty landscape in the 1980s and established the foundation for modern CR total knee systems.

Fig. 6-2: Kinematic condylar prosthesis, illustrating the evolution toward anatomical shaping and PCL retention.
Two early and significant criticisms of the original total condylar prosthesis were its propensity to subluxate posteriorly in flexion—particularly if the flexion gap was not balanced perfectly symmetrically with the extension gap—and a notably smaller range of flexion compared with prosthetic designs that facilitated physiological femoral rollback. By failing to "roll back," the posterior femoral metaphysis in a total condylar knee impinged directly against the posterior aspect of the tibial articular surface at approximately 95 degrees of flexion, severely limiting the patient's functional capacity for activities requiring deep flexion.

Fig. 6-3: Total condylar design is limited in flexion by posterior impingement of the femur on the tibial polyethylene component. With PCL retention or substitution, femoral rollback allows greater flexion.
Posterior-Stabilized and Deep-Dish Designs
To definitively correct the biomechanical limitations of the total condylar knee, the Insall-Burstein posterior cruciate–substituting (posterior-stabilized or PS) design was developed in 1978. This was achieved by adding a central cam mechanism to the femoral articular surface geometry, designed to interact with a vertical polyethylene post on the tibial insert.
Fig. 6-4: Insall-Burstein II posterior-stabilized knee.
The cam on the femoral component engages the central post on the tibial articular surface at approximately 70 degrees of flexion. This engagement mechanically forces the contact point of the femoral-tibial articulation to be posteriorly displaced, effectively manufacturing femoral rollback and allowing significantly greater flexion before impingement occurs. Most current total knee designs utilized globally are direct derivatives of either the Insall-Burstein PS or the kinematic CR designs.
During the late 1980s and 1990s, as tibiofemoral kinematics improved, patellofemoral complications rapidly emerged as the primary cause for reoperation in TKA. Newer designs incorporated greater areas of patellofemoral contact through a larger range of motion and utilized asymmetrical anterior flanges specifically designed to resist patellar subluxation. Concurrently, some systems incorporated a deep-dish or ultra-congruent design as a modular tibial polyethylene option.

Fig. 6-5: Deep-dish component, utilizing sagittal plane concavity to control anteroposterior stability.
The deep-dish design utilizes profound sagittal plane concavity, or dishing, alone to control anteroposterior stability, bypassing the need for a cam-and-post mechanism. In comparing deep-dish components with posterior-stabilized devices, investigators like Laskin et al. found no statistically significant difference at long-term follow-up in range of motion, survivorship, or clinical pain scores. Proponents of this design argue that it incorporates the distinct advantages of cruciate sacrifice without necessitating the obligatory and substantial bone sacrifice in the intercondylar region of the femur required to accommodate a PS box, a resection that may theoretically predispose the distal femur to periprosthetic fracture.
Constraint and Bearing Surface Innovations
When standard CR or PS designs are insufficient to manage severe coronal plane instability, surgeons must escalate the level of constraint. The original constrained condylar knee (CCK) was developed by Insall and colleagues by modifying the posterior-substituting design. This was achieved by significantly enlarging the central post of the tibial polyethylene insert and constraining it intimately against the medial and lateral walls of a deepened, widened central box within the femoral component.

Fig. 6-6: Insall-Burstein II constrained condylar knee (CCK).
Varus-valgus stability is strictly controlled by this mechanism, though a highly calibrated, small amount of varus-valgus toggle (typically 1 to 2 degrees) is permitted to reduce stress transmission to the implant-cement-bone interface. It is critical to note that a CCK cannot be used for the management of severe recurvatum deformity, as the cam-post mechanism does not control hyperextension. The CCK design has been used extensively for complex revision arthroplasty when profound collateral ligament instability is present, and for exceedingly difficult primary arthroplasties in patients presenting with extreme valgus deformity and concurrent medial collateral ligament insufficiency. Rosenberg, Verner, and Galante previously reported progressive bone loss and catastrophic aseptic loosening in highly constrained, rigid hinged designs; the CCK mitigates this specific failure mode by allowing controlled toggle, thus acting as a stress-shielding buffer.
In an effort to address the persistent issue of polyethylene wear, mobile bearing knees, such as the renowned Low Contact Stress (LCS) design, were introduced. The biomechanical rationale was to drastically reduce volumetric polyethylene wear by maximizing articular congruency while simultaneously allowing the bearing itself to move relative to the fixed tibial baseplate.

Supplementary View: Mobile bearing component demonstrating the rotating platform mechanism.
The LCS total knee system, and its modern derivatives, includes a rotating platform design featuring highly congruent tibiofemoral geometry in extension. However, the tibial polyethylene is additionally free to rotate unhindered within the highly polished stem of the tibial baseplate. The theoretical and practical advantages include significantly lower contact stresses at the articulating surfaces, the accommodation of rotational motion of the tibial polyethylene during the complex phases of the gait cycle, and the self-alignment of the tibial polyethylene, which can elegantly compensate for small degrees of rotational malalignment of the tibial baseplate introduced during implantation.
Exhaustive Indications and Contraindications
The decision to proceed with a total knee arthroplasty must be predicated on a rigorous, evidence-based evaluation of the patient's clinical presentation, radiographic findings, and exhaustive failure of non-operative modalities. TKA is primarily indicated for patients suffering from severe, radiographically confirmed osteoarthritis (Kellgren-Lawrence Grade III or IV), advanced rheumatoid arthritis, or debilitating post-traumatic arthritis. The hallmark clinical symptom is intractable mechanical joint pain that severely limits activities of daily living, disrupts sleep architecture, and fundamentally degrades the patient's quality of life.
Before surgical intervention is considered, the patient must have completed and formally failed a comprehensive regimen of conservative management. This regimen typically includes activity modification, aggressive weight loss protocols, targeted physical therapy focusing on quadriceps and hamstring strengthening, the judicious use of non-steroidal anti-inflammatory drugs (NSAIDs), and intra-articular therapies such as corticosteroid or hyaluronic acid injections. Only when these modalities no longer provide acceptable symptomatic relief should arthroplasty be entertained.
Unicompartmental Knee Arthroplasty (UKA) Indications
While TKA is the gold standard for tricompartmental disease, many specialized surgeons strongly advocate for the use of unicompartmental knee arthroplasty (UKA) when arthritic changes are strictly limited to a single knee compartment—most commonly the medial compartment. These prostheses precisely replace the articular surface of either the medial or the lateral femoral condyle and the directly adjacent tibial plateau surface, preserving the cruciate ligaments and the unaffected compartments.
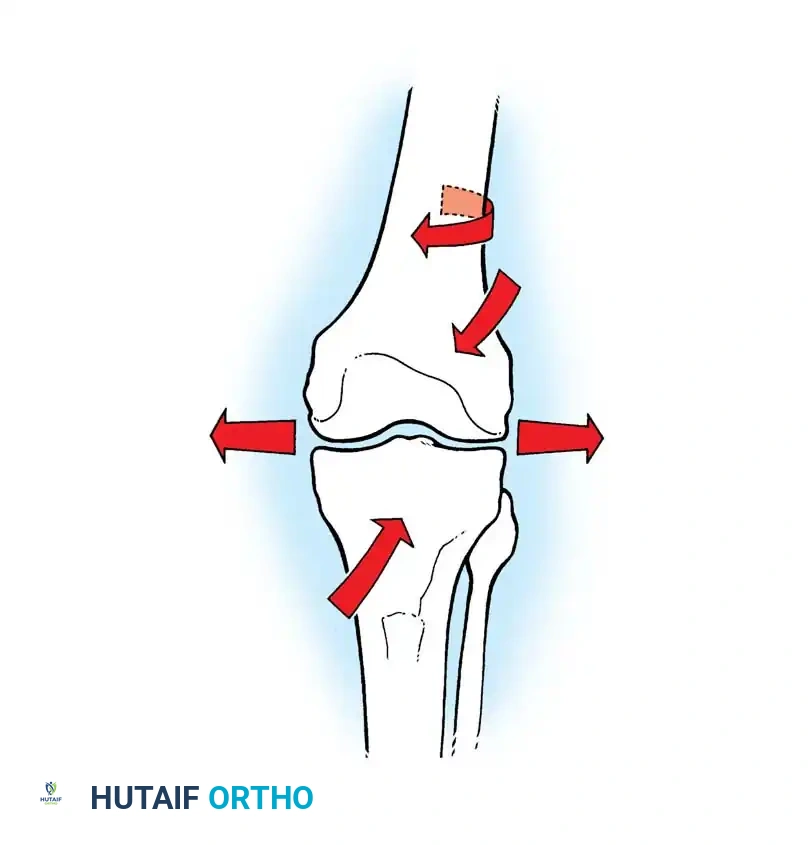
Fig. 6-7: Unicompartmental knee arthroplasty (UKA) components.
Supplementary View: UKA surgical application demonstrating isolated compartmental resurfacing.
The current global trend toward minimally invasive surgical techniques and rapid recovery protocols has substantially rekindled academic and clinical enthusiasm for UKA devices. However, the indications for UKA are exceptionally strict and must be adhered to without compromise to prevent early failure. Classical indications (often referred to as the Kozinn and Scott criteria) include isolated medial or lateral osteoarthritis, an absolutely intact and functional anterior cruciate ligament (ACL), a passively correctable varus or valgus deformity (indicating preserved collateral ligament integrity), a flexion contracture of less than 15 degrees, and a complete absence of significant patellofemoral symptoms or anterior knee pain.
Table: Indications and Contraindications for Knee Arthroplasty
| Category | Total Knee Arthroplasty (TKA) | Unicompartmental Knee Arthroplasty (UKA) |
|---|---|---|
| Primary Indications | End-stage tricompartmental OA, RA, Post-traumatic arthritis. | Isolated medial or lateral compartment OA, AVN of a single condyle. |
| Prerequisites | Failure of >6 months of exhaustive conservative management. | Intact ACL, correctable deformity, flexion contracture <15°, arc of motion >90°. |
| Absolute Contraindications | Active systemic or local joint infection, non-functioning extensor mechanism, severe vascular disease. | Inflammatory arthritis (RA), absent ACL, fixed angular deformity, tricompartmental disease. |
| Relative Contraindications | Severe neuropathic (Charcot) joint, profound osteoporosis, poor soft-tissue envelope, severe medical comorbidities. | Obesity (BMI > 35, historically), heavy manual labor, patellofemoral chondrocalcinosis. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the invisible foundation upon which every successful knee arthroplasty is built. The goal of templating is not merely to select the correct implant size, but to comprehensively map the restoration of the mechanical axis, anticipate the necessary bone resections, identify potential soft-tissue balancing challenges, and recognize any extra-articular deformities that could compromise the final alignment.
Standard radiographic evaluation must include weight-bearing anteroposterior (AP) views, a true lateral view in 30 degrees of flexion, and a skyline (Merchant) patellar view to assess the patellofemoral joint. Crucially, full-length standing hip-to-knee-to-ankle (orthoroentgenogram) radiographs are highly recommended, and in many academic centers, considered mandatory. These full-length films allow the surgeon to accurately measure the mechanical axis deviation (MAD) and identify the center of rotation of angulation (CORA) for any femoral or tibial bowing that might dictate an alteration in the intramedullary or extramedullary alignment guides.
Digital templating software is utilized to superimpose prosthetic outlines over the calibrated radiographs. On the femoral side, templating determines the approximate AP size of the component and establishes the precise angle of the distal femoral resection. Because the mechanical axis of the femur differs from its anatomical axis, the distal femoral cut is typically templated at 5 to 7 degrees of valgus relative to the anatomical axis, ensuring the final joint line is perfectly perpendicular to the mechanical axis of the lower extremity. On the tibial side, templating assesses the required depth of resection, the presence of asymmetrical bone loss (e.g., a massive medial tibial plateau defect requiring metal augments or structural bone graft), and the optimal posterior slope.
Positioning and Anesthesia Modalities
The surgical procedure is typically performed under regional anesthesia—most commonly a spinal or epidural block—combined with advanced peripheral nerve blocks. The adductor canal block has largely replaced the femoral nerve block in modern practice, as it provides profound sensory analgesia to the anteromedial knee while brilliantly preserving quadriceps motor function, thereby facilitating rapid postoperative mobilization and reducing the risk of inpatient falls.
The patient is positioned perfectly supine on the operating table. A pneumatic tourniquet is applied to the proximal thigh, though its inflation is often delayed until cementation in modern "tourniquet-less" or "limited-tourniquet" protocols to minimize ischemic muscle damage and postoperative thigh pain. The operative leg is placed in a specialized, rigid leg holder or a lateral post system that allows for stable hyperflexion (up to 120 degrees) and provides a fulcrum for applying varus or valgus stress during meticulous soft-tissue balancing.
Step-by-Step Surgical Approach and Fixation Technique
The execution of a total knee arthroplasty demands uncompromising precision. The standard surgical approach begins with a perfectly midline longitudinal skin incision, extending from the distal third of the quadriceps tendon, passing over the center of the patella, to the medial border of the tibial tubercle. Full-thickness fasciocutaneous flaps are elevated to preserve the delicate prepatellar vascular plexus and minimize the risk of devastating postoperative skin necrosis.
Arthrotomy and Exposure
The medial parapatellar arthrotomy remains the most versatile and universally utilized deep approach. The incision extends longitudinally through the medial retinaculum, leaving a robust cuff of tissue on the medial border of the patella for secure closure, and extends proximally into the quadriceps tendon, splitting the rectus femoris and vastus medialis obliquus (VMO). Once the joint is entered, the patella is either everted or laterally subluxated.
Alternative, quadriceps-sparing approaches, such as the midvastus or subvastus approaches, may be utilized by experienced surgeons. These approaches theoretically spare the extensor mechanism from direct surgical trauma, potentially accelerating early straight-leg raise recovery and reducing postoperative pain. However, they offer inherently more limited exposure and are generally contraindicated in revision scenarios, severely stiff knees, or morbidly obese patients where visualization is paramount.
Bone Preparation: Measured Resection vs. Gap Balancing
The fundamental philosophy of bone preparation is dictated by either the measured resection technique or the gap balancing technique. Most modern, high-volume arthroplasty systems utilize a sophisticated hybrid approach.
Distal Femoral Resection: The medullary canal of the femur is accessed just anterior to the origin of the PCL. An intramedullary alignment rod is introduced, and the distal cutting block is securely pinned at the preoperatively templated valgus angle (usually 5 to 7 degrees). A measured resection is then performed, typically removing 9 to 10 mm of bone from the prominent distal condyle, which precisely matches the thickness of the distal flange of the chosen femoral component. This step establishes the extension gap.
Proximal Tibial Resection: The tibia is typically prepared using an extramedullary alignment guide, referencing the medial third of the tibial tubercle proximally and the center of the talus distally. The cut is made perfectly perpendicular to the mechanical axis of the tibia in the coronal plane. In the sagittal plane, a 3 to 5-degree posterior slope is often incorporated to aid in deep flexion and to balance the PCL in cruciate-retaining designs.
Rotational Alignment and Soft Tissue Balancing
Establishing the correct rotational alignment of the femoral component is arguably the most critical step in preventing postoperative complications. Malrotation, particularly internal rotation of the femoral component, fundamentally alters patellofemoral tracking, leading to intractable anterior knee pain, patellar subluxation, and premature, catastrophic polyethylene wear.
Clinical Pearl: The femoral component must be aligned parallel to the surgical transepicondylar axis (sTEA). Alternatively, it can be set perfectly perpendicular to Whiteside’s line (the anteroposterior axis of the trochlea) or externally rotated 3 degrees relative to the posterior condylar axis (PCA) to compensate for the natural internal torsion of the proximal tibia.
Once the bone cuts are complete, the surgeon must ensure that the extension gap and the flexion gap are perfectly equal and rectangular. If the knee is excessively tight in extension but balanced in flexion, additional distal femur must be resected or the posterior capsule must be released. Conversely, if the knee is tight in flexion but balanced in extension, the tibial slope may be increased, or a smaller femoral component (reducing the posterior condylar offset) may be selected.
Component Cementation
The vast majority of primary TKAs utilize polymethylmethacrylate (PMMA) bone cement for definitive fixation. The sclerotic bone surfaces must be meticulously prepared using pulsatile lavage to remove marrow, fat, and debris, ensuring optimal micro-interlock between the cement and the cancellous bone trabeculae. The bone is meticulously dried. The cement is applied in a doughy state, and the components are impacted into place. The knee is then brought into full extension to axially pressurize the cement mantle while it polymerizes. All extruded cement must be rigorously removed, particularly from the posterior recesses, to prevent third-body wear or mechanical impingement.
Complications, Incidence Rates, and Salvage Management
Despite the overwhelming success of TKA, complications can and do occur, often requiring complex, morbid revision surgeries. The orthopedic surgeon must be highly vigilant in both the prevention and rapid management of these catastrophic events.
Periprosthetic joint infection (PJI) remains the most devastating complication, occurring in approximately 1% to 2% of primary TKAs. Diagnosis relies on a high index of suspicion, elevated serum inflammatory markers (CRP, ESR), and definitive synovial fluid analysis (cell count > 3,000 cells/µL with > 80% PMNs). Acute infections (within 4 weeks of surgery) may be managed with a thorough Debridement, Antibiotics, and Implant Retention (DAIR) procedure, provided the implants are solidly fixed. Chronic infections mandate a grueling two-stage revision arthroplasty, involving the complete removal of all hardware, the insertion of an antibiotic-impregnated cement spacer, a prolonged course of targeted intravenous antibiotics, and eventual reimplantation once the infection is definitively eradicated.
Aseptic loosening and osteolysis, historically driven by polyethylene wear debris leading to a macrophage-mediated inflammatory cascade, have decreased significantly with the advent of highly cross-linked polyethylene. However, it remains a primary cause of late failure. Management requires revision arthroplasty, often utilizing metaphyseal cones or diaphyseal stems to bypass areas of profound bone loss and achieve stable fixation.
Instability following TKA is broadly categorized by the arc of motion in which it occurs. Extension instability is typically due to an over-resected distal femur or unrecognized collateral ligament injury. Flexion instability often presents as recurrent effusions and a sense of giving way when descending stairs, resulting from an excessive anterior-posterior dimension of the flexion gap. Mid-flexion instability is a complex kinematic conflict often resulting from joint line elevation or improper component rotation.
Table: Common TKA Complications and Management
| Complication | Approximate Incidence | Primary Etiology | Salvage / Management Strategy |
|---|---|---|---|
| Periprosthetic Joint Infection (PJI) | 1.0% - 2.0% | Bacterial colonization (Staph aureus, CoNS). | Acute: DAIR. Chronic: 2-stage exchange with articulating spacer. |
| Aseptic Loosening / Osteolysis | 2.0% - 4.0% (at 15 yrs) | Particulate wear debris, micromotion, poor initial cementation. | Revision arthroplasty with stems, augments, or metaphyseal cones. |
| Patellofemoral Instability | 1.0% - 3.0% | Internal rotation of femoral/tibial components, valgus malalignment. | Lateral retinacular release, proximal realignments, or component revision. |
| Periprosthetic Fracture | 0.5% - 2.0% | Osteopenia, anterior femoral notching, trauma. | ORIF (locking plates) if implant stable; Revision to long-stem/distal femoral replacement if loose. |
| Arthrofibrosis (Stiffness) | 3.0% - 5.0% | Inadequate pain control, poor rehab, oversized components. | Aggressive PT, Manipulation Under Anesthesia (MUA) at 6-12 weeks, Arthroscopic lysis. |
Phased Post-Operative Rehabilitation Protocols
The success of a technically perfect TKA can be completely undermined by a poorly executed postoperative rehabilitation protocol. Modern recovery emphasizes rapid mobilization, multimodal pain management, and the aggressive prevention of arthrofibrosis and venous thromboembolism (VTE).
Phase 1: Acute Recovery (0 to
