Comprehensive Introduction and Patho-Epidemiology
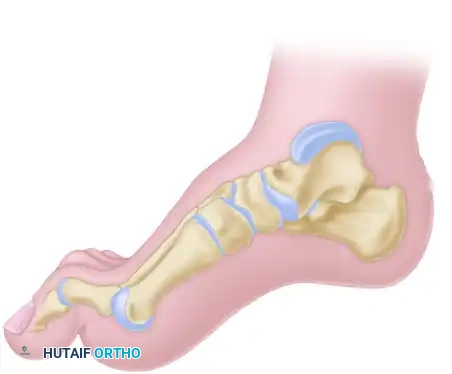
The cavus foot, clinically referred to as pes cavus, represents a highly complex, multiplanar structural deformity of the foot and ankle. It is fundamentally characterized by an abnormally high medial longitudinal arch, which is almost universally accompanied by a constellation of secondary deformities including forefoot equinus (plantarflexion), hindfoot varus, and clawing of the lesser toes. Unlike the relatively common and often asymptomatic flexible flatfoot, the cavus foot is frequently symptomatic, progressive, and associated with significant underlying neuromuscular pathology. The overarching goal of surgical intervention is not merely cosmetic correction, but the restoration of a stable, plantigrade, and functional weight-bearing limb that is braceable and resistant to recurrent ulceration.
The etiology of the cavus foot is predominantly neuromuscular, with Charcot-Marie-Tooth (CMT) disease being the most prevalent cause, accounting for up to 60-70% of bilateral cavovarus deformities. CMT is a hereditary motor and sensory neuropathy (HMSN), most commonly inherited in an autosomal dominant pattern linked to a duplication of the PMP22 gene on chromosome 17. The disease process dictates a slow, progressive distal-to-proximal demyelination and axonal degeneration, leading to highly specific patterns of muscle denervation and subsequent imbalance. Other significant etiologies include poliomyelitis, spinal dysraphism (such as tethered cord syndrome or spina bifida), Friedreich’s ataxia, cerebral palsy, and post-traumatic sequelae (e.g., malunion of midfoot fractures or compartment syndrome). While a subset of patients presents with "idiopathic" cavus, exhaustive neurological workup often reveals subtle, previously undiagnosed upper or lower motor neuron lesions.
Understanding the temporal progression of the cavus deformity is critical for surgical decision-making. The deformity typically begins in childhood or early adolescence as a purely flexible, dynamically driven malalignment. During this early phase, the foot assumes a cavovarus posture during gait and weight-bearing due to active muscle imbalances, but can be passively corrected to a neutral, plantigrade position by the examiner. However, as the disease progresses and the deforming forces persist, the soft tissues—specifically the plantar fascia, joint capsules, and ligaments—undergo adaptive shortening and contracture. Furthermore, the constant abnormal mechanical loading alters the growth and remodeling of the tarsal bones, leading to structural wedging. Consequently, the initially flexible deformity inevitably transitions into a rigid, fixed osseous deformity that is completely refractory to conservative management or isolated soft-tissue releases.
When the cavus deformity reaches this rigid, structural stage, osseous interventions become unequivocally mandated. Soft tissue procedures, such as the Steindler plantar fasciotomy or tendon transfers (e.g., Jones transfer, split tibialis anterior tendon transfer), remain essential adjunctive measures to rebalance the foot dynamically, but they cannot correct fixed bony architecture. The cornerstone of osseous correction for midfoot-driven anterior cavus lies in midtarsal osteotomies. The anterior tarsal wedge osteotomy, originally described by Cole, and the V-osteotomy of the tarsus, developed by Japas, are foundational techniques designed to surgically elevate the depressed forefoot. These procedures, often combined with adjunctive hindfoot realignments like the Dwyer or Samilson osteotomies, form the comprehensive surgical armamentarium required to address the severe, rigid cavovarus foot.
Detailed Surgical Anatomy and Biomechanics
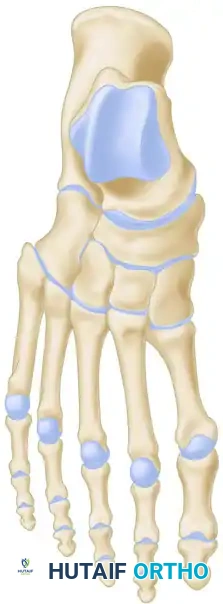
The surgical management of the cavus foot demands an exhaustive, highly technical understanding of foot and ankle biomechanics, as the deformity is fundamentally a manifestation of predictable muscle imbalances acting upon the osseous architecture. The normal foot functions as a dynamic tripod, with weight distributed evenly between the calcaneal tuberosity posteriorly, the first metatarsal head anteromedially, and the fifth metatarsal head anterolaterally. In the cavus foot, this tripod is severely distorted. The primary, initiating deforming force in the vast majority of neuromuscular cavus feet (particularly in CMT) is a fixed plantarflexion of the first ray. This occurs because the peroneus longus, which inserts on the plantar-lateral aspect of the first cuneiform and first metatarsal base, retains its strength and significantly overpowers its weakened antagonist, the tibialis anterior.
This relentless, unopposed pull of the peroneus longus drives the medial column into rigid equinus. As the patient bears weight on this plantarflexed first ray, it acts as a rigid kickstand. The ground reaction force pushes upward against the depressed first metatarsal head, which secondarily forces the hindfoot into a compensatory varus posture to allow the lateral border of the foot to contact the ground. Initially, this hindfoot varus is entirely flexible and driven solely by the forefoot deformity. However, over time, the subtalar joint capsule contracts, and a secondary muscle imbalance exacerbates the condition: the tibialis posterior (a strong invertor) overpowers the weakened peroneus brevis (an evertor), actively pulling the hindfoot into structural varus.
Concurrently, the intrinsic musculature of the foot (lumbricals and interossei) undergoes denervation and wasting, leading to an "intrinsic-minus" foot. The intrinsic muscles normally flex the metatarsophalangeal (MTP) joints and extend the interphalangeal (IP) joints. When they fail, the strong extrinsic extensors (extensor digitorum longus and extensor hallucis longus) overpower the weak intrinsics, hyperextending the MTP joints. The extrinsic flexors (flexor digitorum longus and flexor hallucis longus) subsequently flex the IP joints, resulting in rigid claw toe deformities. The hyperextension of the MTP joints further exacerbates the cavus deformity by driving the metatarsal heads plantarward, increasing the retrograde pressure on the forefoot and tightening the plantar fascia through the windlass mechanism.
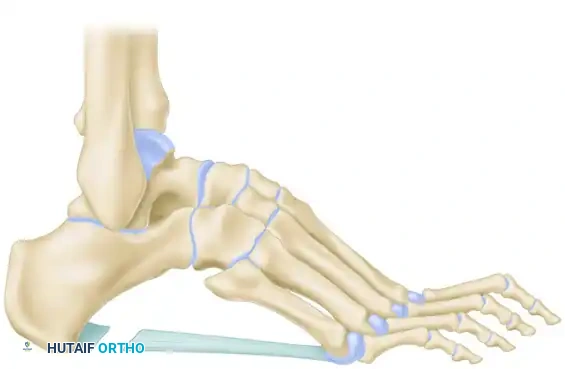
The Coleman block test is the most critical clinical and biomechanical assessment utilized to differentiate between a flexible, compensatory hindfoot varus and a rigid, structural hindfoot varus. The patient is instructed to stand with the heel and lateral border of the foot on a 1-inch wooden block, allowing the plantarflexed first ray to drop off the medial edge of the block into free space. By eliminating the ground reaction force acting on the first metatarsal, the compensatory mechanism is negated. If the hindfoot varus completely corrects to a neutral or slight valgus alignment while on the block, the hindfoot is deemed flexible; in this scenario, correcting the forefoot deformity (e.g., via a dorsiflexion osteotomy of the first metatarsal or a midtarsal osteotomy) will spontaneously correct the hindfoot. Conversely, if the hindfoot remains in varus despite the first ray dropping off the block, the hindfoot deformity is rigid, and a concomitant calcaneal osteotomy (such as a Dwyer procedure) is strictly required to realign the mechanical axis.
Exhaustive Indications and Contraindications
The decision to proceed with complex midtarsal and hindfoot osteotomies is highly nuanced and depends heavily on the patient's age, skeletal maturity, neurological prognosis, and the precise apex of the deformity. Midtarsal osteotomies, specifically the Cole and Japas procedures, are indicated for patients with rigid anterior cavus where the apex of the deformity is located at the midtarsal (Chopart) or tarsometatarsal (Lisfranc) joints. These procedures are generally reserved for skeletally mature patients or older adolescents near skeletal maturity, as aggressive midfoot resections in young children can severely stunt foot growth and lead to unpredictable secondary deformities. Furthermore, these osseous procedures are indicated only after conservative measures—such as custom-molded ankle-foot orthoses (AFOs), accommodative footwear, and aggressive physical therapy—have failed to prevent recurrent lateral column overload, intractable plantar keratoses, or recurrent ankle instability.
Contraindications to midtarsal osteotomies must be carefully evaluated to prevent catastrophic surgical failures. Absolute contraindications include active deep soft tissue or bone infection, severe peripheral arterial disease (which precludes healing of complex osteotomies and extensive soft tissue dissection), and a purely flexible deformity that can be entirely corrected with soft tissue releases and tendon transfers. Relative contraindications include profound sensory neuropathy, such as advanced Charcot neuroarthropathy, where the lack of protective sensation significantly increases the risk of postoperative nonunion, hardware failure, and progressive rocker-bottom deformity. In such neuropathic cases, primary arthrodesis (e.g., triple arthrodesis or medial column fusion) is often a safer, more durable option than joint-sparing or joint-sacrificing osteotomies.
| Parameter | Indications for Midtarsal/Hindfoot Osteotomies | Contraindications (Absolute & Relative) |
|---|---|---|
| Deformity Type | Rigid structural cavovarus deformity; Apex at midfoot. | Purely flexible deformity (manage with soft tissue). |
| Skeletal Maturity | Skeletally mature or nearing skeletal maturity (>14 years). | Immature skeleton with significant growth remaining. |
| Clinical Presentation | Intractable plantar keratoses, recurrent lateral ankle sprains, brace intolerance. | Asymptomatic cavus; Active infection; Severe ischemia. |
| Neurological Status | Slowly progressive or static neuromuscular disease (e.g., CMT). | Rapidly progressive disease; Advanced Charcot arthropathy. |
| Hindfoot Flexibility | Rigid varus (requires adjunctive Dwyer/Samilson). | Flexible varus (corrects with forefoot intervention alone). |
The choice between a Cole anterior tarsal wedge osteotomy and a Japas V-osteotomy depends largely on the severity of the deformity and the acceptable functional trade-offs. The Cole procedure is highly powerful and provides excellent, predictable correction of severe sagittal plane deformities by resecting a substantial dorsal wedge. However, it inevitably shortens the medial and lateral columns of the foot, which can make shoe fitting challenging and alter the biomechanics of the lever arm. The Japas V-osteotomy, conversely, avoids significant shortening by utilizing a V-shaped cut that allows the midfoot to be depressed without removing a large block of bone. However, the Japas procedure is technically more demanding, requires meticulous extraperiosteal dissection to avoid joint violation, and may not provide sufficient correction for the most extreme cases of rigid anterior cavus.
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for cavus foot reconstruction requires a meticulous combination of clinical examination and advanced radiographic analysis. The clinical examination must document the exact range of motion of the ankle, subtalar, and transverse tarsal joints. Muscle strength testing (specifically isolating the tibialis anterior, tibialis posterior, peroneus longus, and peroneus brevis) is paramount for planning concurrent tendon transfers. The Silfverskiöld test is performed to evaluate for gastrocnemius or Achilles tendon contracture, which frequently accompanies the cavus foot and must be addressed surgically to prevent postoperative forefoot overload. Finally, the vascular status must be rigorously assessed, as the extensive dorsal incisions required for midtarsal osteotomies demand robust perfusion for adequate wound healing.
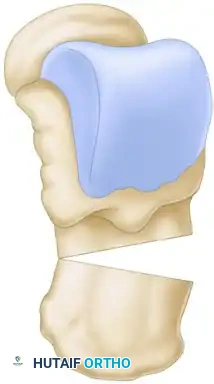
Standard weight-bearing anteroposterior (AP) and lateral radiographs of the foot and ankle are the cornerstone of radiographic planning. On the lateral radiograph, several key angles are measured to quantify the deformity and pinpoint its apex. Meary’s angle, the angle formed by the intersection of the longitudinal axis of the talus and the longitudinal axis of the first metatarsal, is normally 0 degrees. In a cavus foot, this angle is increased with the apex pointing dorsally; an angle greater than 15 degrees indicates severe cavus. The Hibbs angle, formed by the intersection of the longitudinal axis of the calcaneus and the first metatarsal, normally ranges from 135 to 140 degrees; in severe cavus, this angle approaches 90 degrees. The calcaneal pitch, the angle between the inferior border of the calcaneus and the supporting surface, is normally 20 to 30 degrees but is significantly increased in calcaneocavus variants.
Advanced imaging, specifically weight-bearing computed tomography (WBCT), has revolutionized preoperative templating for complex midfoot osteotomies. WBCT provides a true three-dimensional representation of the osseous architecture under physiologic load, allowing the surgeon to precisely map the apex of the deformity and calculate the exact dimensions of the required bone resection. For a Cole procedure, the surgeon can template the exact millimeter width of the dorsal wedge needed to restore Meary’s angle to neutral. This templating minimizes the risk of intraoperative under-correction or over-correction (which can result in a devastating rocker-bottom deformity). Furthermore, CT imaging helps assess the bone stock and identify any pre-existing degenerative changes in the transverse tarsal or subtalar joints, which might necessitate a primary arthrodesis rather than an osteotomy.
Patient positioning and operating room setup are critical for the seamless execution of these complex, multi-stage procedures. The patient is placed supine on the operating table. A significant bump (often a large gel pad or folded blankets) is placed under the ipsilateral hip to internally rotate the lower extremity, bringing the foot into a neutral, vertically oriented position. This is essential, as the severe varus deformity naturally forces the foot into external rotation when supine, making dorsal and lateral approaches exceedingly difficult. A well-padded thigh or calf tourniquet is applied to ensure a bloodless field, which is critical for identifying and protecting the delicate dorsal neurovascular structures. Fluoroscopy must be readily available and positioned to easily obtain true AP, lateral, and axial views of the foot and ankle throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
Soft Tissue Release (Steindler Stripping)
Before executing any osseous midfoot correction, the contracted plantar soft tissues must be released to allow the forefoot to unfurl. The Steindler plantar fasciotomy is the gold standard approach. A 3- to 4-cm longitudinal incision is made on the medial aspect of the heel, overlying the medial tuberosity of the calcaneus. The dissection is carried down to the plantar fascia. Using electrocautery and a periosteal elevator, the plantar fascia, along with the origins of the abductor hallucis, flexor digitorum brevis, and abductor digiti minimi, are completely detached from the calcaneal tuberosity. The dissection must stay strictly on the bone to avoid injury to the lateral plantar nerve and artery. Once released, the surgeon should be able to palpate a significant increase in the flexibility of the longitudinal arch.
Anterior Tarsal Wedge Osteotomy (Cole)
The Cole procedure involves the resection of a dorsally based wedge of bone through the navicular-cuneiform and cuboid articulations. A 10-cm dorsal longitudinal incision is made centered over the midtarsal joints. The superficial peroneal nerve branches and the dorsalis pedis artery are meticulously identified, mobilized, and protected with vessel loops. The extensor hallucis longus (EHL) is retracted medially, and the extensor digitorum longus (EDL) is retracted laterally. The periosteum over the navicular, cuneiforms, and cuboid is incised longitudinally and elevated to expose the osseous anatomy.
Using an oscillating saw, the proximal cut is initiated vertically through the center of the navicular and the cuboid. The distal cut is then made through the proximal portions of the cuneiforms and the distal cuboid, angling proximally to meet the first cut at the plantar cortex. The width of the dorsal wedge is dictated by preoperative templating, typically ranging from 15 to 20 mm. It is absolutely critical to leave the plantar cortex intact to act as a stabilizing hinge; complete violation of the plantar cortex risks gross instability and a rocker-bottom deformity. Once the wedge of bone is removed en bloc, the forefoot is gently elevated (dorsiflexed) to close the osteotomy gap. Fixation is achieved using heavy, crossed Steinmann pins, large-fragment cannulated screws, or modern dorsal locking plates, ensuring rigid compression across the osteotomy site.
V-Osteotomy of the Tarsus (Japas)
The Japas V-osteotomy offers an alternative that preserves foot length. Through a similar dorsal approach, the extraperiosteal exposure is carried from the talonavicular joint to the tarsometatarsal joints. The apex of the "V" is marked directly in the midline of the navicular. The medial limb of the osteotomy is directed distally and medially, exiting through the medial cuneiform just proximal to the first metatarsocuneiform joint. The lateral limb is directed distally and laterally, exiting through the cuboid just proximal to the fifth metatarsocuboid joint.
The cuts are made with a combination of a reciprocating saw and sharp osteotomes. The surgeon must exercise extreme caution to avoid violating the talonavicular or calcaneocuboid joints, which would lead to rapid arthritic degeneration.

Once the V-cut is completed, the distal forefoot segment is depressed plantarward and translated slightly dorsally relative to the proximal segment, effectively flattening the longitudinal arch without resecting a bone block. The correction is held with longitudinal traction, and fixation is secured with two or three stout Steinmann pins driven from the metatarsals proximally into the midfoot and hindfoot.

Adjunctive Hindfoot Osteotomies (Dwyer and Samilson)
If the Coleman block test demonstrated a rigid hindfoot varus, a Dwyer lateral closing wedge osteotomy is performed concurrently. A curved lateral incision is made posterior and inferior to the lateral malleolus. The sural nerve is identified and protected. The lateral wall of the calcaneus is exposed, and an oscillating saw is used to resect a laterally based wedge of bone (typically 8 to 12 mm wide) just posterior to the posterior facet of the subtalar joint.

The medial cortex is intentionally left intact and broken manually (greensticked) to close the gap, shifting the calcaneal tuberosity into valgus. Fixation is achieved with a single large cannulated screw or a stepped staple.
For severe calcaneocavus deformities, a Samilson crescentic osteotomy is preferred. Through a lateral approach, a dome-shaped cut is made through the calcaneal tuberosity using a specialized crescentic saw blade.

This allows the posterior fragment to be rotated dorsally, decreasing the calcaneal pitch, and translated laterally to correct varus.


This multiplanar correction is highly versatile and is fixed with two large-fragment screws directed from posterior to anterior.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, midtarsal and hindfoot osteotomies for the cavus foot carry a significant risk profile. The complexity of the multiplanar deformity, combined with the often compromised soft tissue envelope and underlying neurological pathology, predisposes these patients to various postoperative challenges. Nonunion and delayed union are among the most serious complications, occurring in approximately 5% to 10% of midtarsal osteotomies. The risk is elevated if there is excessive periosteal stripping, thermal necrosis from aggressive saw use without adequate irrigation, or failure to achieve rigid compression across the osteotomy site. Nonunions present with persistent midfoot pain, swelling, and progressive loss of correction, necessitating revision surgery.
Malalignment, specifically under-correction or over-correction, represents a failure of preoperative planning or intraoperative execution. Under-correction typically occurs when the surgeon fails to recognize a rigid hindfoot varus and omits the necessary Dwyer osteotomy, or when the dorsal wedge resected during a Cole procedure is insufficiently sized. This results in residual lateral column overload and recurrent plantar ulceration. Conversely, over-correction is a catastrophic complication that occurs when the plantar cortex is completely violated during a midtarsal wedge resection, allowing the forefoot to dorsiflex excessively. This creates a rocker-bottom deformity, shifting the weight-bearing axis to the vulnerable midfoot, which inevitably leads to severe pain and ulceration.
Neurological complications are also highly prevalent. The superficial peroneal nerve and the deep peroneal nerve (along with the dorsalis pedis artery) are at significant risk during the dorsal approaches for the Cole and Japas procedures. Aggressive retraction can lead to neuropraxia, while inadvertent transection results in painful neuromas and sensory deficits. Similarly, the sural nerve is highly vulnerable during the lateral approach for the Dwyer and Samilson calcaneal osteotomies. Careful, blunt dissection and the use of atraumatic retractors are mandatory to mitigate these risks.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Revision Strategy |
|---|---|---|---|
| Nonunion / Delayed Union | 5% - 10% | Excessive stripping, thermal necrosis, inadequate fixation, smoking. | Revision with autologous bone grafting (iliac crest) and rigid plate fixation; consider primary midfoot arthrodesis. |
| Under-correction (Residual Varus) | 10% - 15% | Failure to perform Dwyer; inadequate soft tissue release; undersized wedge. | Revision calcaneal osteotomy; first metatarsal dorsiflexion osteotomy; targeted tendon transfers. |
| Over-correction (Rocker-Bottom) | < 5% | Violation of plantar cortex hinge; excessive dorsal wedge resection. | Complex structural bone grafting; extended medial/lateral column arthrodesis to restore arch. |
| Nerve Injury (Neuroma) | 5% - 12% | Aggressive retraction or transection of superficial peroneal or sural nerves. | Conservative: Gabapentin, targeted injections. Surgical: Neuroma excision and targeted muscle reinnervation (TMR) or burial into bone. |
| Wound Dehiscence / Necrosis | 5% - 8% | Poor vascularity, excessive tourniquet time, premature weight-bearing. | Local wound care, negative pressure wound therapy (NPWT); rarely requires local rotational flaps. |
Salvage management for failed cavus foot reconstructions is exceptionally challenging and typically requires sacrificing joint mobility to restore stability. If a midtarsal osteotomy goes on to a painful nonunion or severe malunion, the definitive salvage procedure is a triple arthrodesis (fusion of the subtalar, talonavicular, and calcaneocuboid joints) combined with a midfoot fusion if necessary. While an arthrodesis reliably eliminates pain and corrects deformity, it significantly alters the biomechanics of the foot, increasing stress on the adjacent ankle joint and potentially accelerating tibiotalar osteoarthritis over the ensuing decades.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following complex midtarsal and adjunctive hindfoot osteotomies is lengthy, demanding, and requires strict adherence to phased protocols to ensure osseous union and prevent catastrophic loss of correction. The immediate postoperative phase (Weeks 0-2) focuses entirely on wound healing, edema control, and pain management. In the operating room, the limb is placed in a bulky, well-padded short-leg splint or a bivalved cast, extending from the base of the toes to just below the tibial tubercle. The patient is made strictly non-weight-bearing (NWB) on the operative extremity. Elevation of the limb above the level of the heart is absolutely critical during the first 72 hours to prevent severe swelling, which can compromise the dorsal incisions and lead to wound necrosis. Chemical deep vein thrombosis (DVT) prophylaxis is initiated based on patient risk factors, typically utilizing low-molecular-weight heparin or direct oral anticoagulants.
The intermediate phase (Weeks 2-8) begins at the first postoperative clinic visit. The initial spl
