Surgical Management of Anterior Tarsal Tunnel Syndrome and Interdigital Neuritis
Key Takeaway
Anterior tarsal tunnel syndrome involves entrapment of the deep peroneal nerve beneath the inferior extensor retinaculum. Surgical release requires a precise dorsal approach, identifying the nerve alongside the dorsalis pedis artery, and selectively dividing the constricting retinacular bands. Concurrently, interdigital neuromas represent a degenerative perineural fibrosis rather than a true neuroma, requiring careful clinical evaluation and an understanding of forefoot biomechanics for optimal surgical and conservative management.
INTRODUCTION TO FOREFOOT NERVE ENTRAPMENT SYNDROMES
Nerve entrapment syndromes of the foot and ankle present a complex diagnostic and therapeutic challenge for the orthopedic surgeon. Among the most clinically significant, yet frequently misdiagnosed, are Anterior Tarsal Tunnel Syndrome (ATTS) and Interdigital Neuroma (commonly referred to as Morton's Neuroma). While ATTS involves the compression of the deep peroneal nerve beneath the inferior extensor retinaculum, interdigital neuromas involve a degenerative, compressive neuropathy of the common digital nerve.
This comprehensive guide details the surgical technique for anterior tarsal tunnel release as described by Mann, alongside a rigorous academic analysis of the pathological and histological findings associated with interdigital neuromas.
ANTERIOR TARSAL TUNNEL RELEASE
Anterior Tarsal Tunnel Syndrome is an entrapment neuropathy of the deep peroneal nerve. As the nerve courses over the anterior aspect of the ankle joint, it passes beneath the unyielding inferior extensor retinaculum. Compression in this anatomical bottleneck leads to localized pain, paresthesias in the first web space, and potential motor weakness in the extensor digitorum brevis (EDB) and extensor hallucis brevis (EHB).
Surgical Anatomy and Biomechanics
The deep peroneal nerve descends through the anterior compartment of the leg, crossing the ankle joint deep to the superior extensor retinaculum. As it enters the dorsum of the foot, it passes beneath the cruciform inferior extensor retinaculum. Here, it typically bifurcates into:
1. Medial Terminal Branch: Primarily sensory, supplying the first dorsal web space.
2. Lateral Terminal Branch: Primarily motor, supplying the EDB and EHB muscles, with articular branches to the tarsal joints.
Compression is most frequently caused by osteophytes at the talonavicular joint, ganglion cysts, or severe hypertrophic changes of the inferior extensor retinaculum secondary to repetitive microtrauma or tight footwear.
Clinical Pearl: Always differentiate ATTS from L5 radiculopathy or superficial peroneal nerve entrapment. A positive Tinel's sign localized strictly over the deep peroneal nerve at the level of the inferior extensor retinaculum, combined with isolated first web space paresthesia, is pathognomonic for ATTS.
Preoperative Planning and Indications
Surgical intervention is indicated only after the exhaustion of conservative measures, including footwear modification, orthoses, non-steroidal anti-inflammatory drugs (NSAIDs), and targeted corticosteroid injections.
Before proceeding to surgery, the exact area of compression must be localized. This is typically found at either the anterior ankle joint line or the dorsal talonavicular joint. High-resolution ultrasound or MRI is highly recommended to rule out space-occupying lesions such as ganglion cysts or occult osteophytes.
Surgical Technique (Mann's Approach)
The following technique, popularized by Mann and Baxter, emphasizes a targeted, minimally invasive release of the constricting structures to preserve the biomechanical integrity of the extensor mechanism.
Step 1: Positioning and Preparation
* The patient is placed in the supine position on the operating table.
* A bump is placed under the ipsilateral hip to internally rotate the leg to a neutral position, optimizing exposure of the dorsal foot.
* A thigh or calf tourniquet is applied and inflated after exsanguination to ensure a bloodless surgical field.
Step 2: Incision and Superficial Dissection
* Make a longitudinal incision, approximately 5 to 7 cm in length, over the dorsum of the foot.
* The incision should extend from the level of the talonavicular joint distally toward the first intermetatarsal space.
* Carefully dissect through the subcutaneous tissues. Extreme caution must be exercised to identify and retract any crossing branches of the superficial peroneal nerve to prevent painful postoperative neuromas.
Step 3: Deep Dissection and Nerve Identification
* Identify the deep fascia and the inferior extensor retinaculum.
* Locate the dorsalis pedis artery, which serves as a critical anatomical landmark. The deep peroneal nerve typically lies immediately adjacent (usually lateral) to the artery.
* Trace the deep peroneal nerve as it courses beneath the extensor hallucis brevis muscle belly.
Step 4: Retinacular Release and Decompression
* Once the nerve is isolated, identify the specific constricting portion of the inferior extensor retinaculum.
* Surgical Warning: Mann and Baxter strongly recommend releasing only the portion of the retinaculum that is actively constricting the nerve. Complete division of the entire retinaculum can lead to extensor tendon bowstringing and subsequent biomechanical dysfunction.
* Carefully divide the constricting fascial bands using tenotomy scissors, ensuring the nerve is protected with a blunt elevator or right-angle forceps.
Step 5: Addressing Underlying Pathology
* Inspect the floor of the anterior tarsal tunnel.
* If a ganglion cyst is present, it must be meticulously excised down to its stalk, which often originates from the talonavicular or naviculocuneiform joint capsule.
* If dorsal osteophytes are the source of compression, use a rongeur or a small osteotome to resect the bony prominences until the nerve bed is completely flat and free of tension.
Step 6: Closure
* Deflate the tourniquet and achieve meticulous hemostasis using bipolar electrocautery. Hematoma formation in this tight space can lead to recurrent scarring and entrapment.
* Close the subcutaneous tissue with absorbable sutures and the skin with non-absorbable monofilament sutures.
Postoperative Care and Rehabilitation
- Immediate Post-op: The patient is placed in a well-padded short leg cast or a rigid removable walking boot.
- Weight Bearing: The patient may begin weight bearing to tolerance immediately, provided the pain is adequately controlled.
- Suture Removal: Sutures are typically removed at 2 weeks postoperatively.
- Immobilization: The walking boot is discontinued at 2 weeks unless localized tenderness or swelling persists.
- Return to Activity: For athletic patients, progressive training and sport-specific drills can safely resume 4 to 6 weeks after surgery, depending on the resolution of neurological symptoms.
INTERDIGITAL NEUROMA (MORTON'S NEUROMA)
While anterior tarsal tunnel syndrome involves the deep peroneal nerve, interdigital neuromas affect the common digital nerves of the forefoot, most frequently in the third web space. Despite the ubiquitous use of the term "neuroma," extensive histological analysis reveals that this condition is not a true neoplastic or proliferative neuroma, but rather a degenerative neuropathy.
Clinical Evaluation and Provocative Testing
Accurate clinical diagnosis relies heavily on targeted physical examination maneuvers designed to reproduce the patient's symptoms by compressing the enlarged nerve against the deep transverse intermetatarsal ligament.
1. Squeeze Test (Mulder's Sign)
Digital manipulation is performed with pressure applied just proximal to the metatarsal heads. The examiner squeezes the forefoot between the index finger and thumb, compressing the metatarsal heads together. This action forces the thickened nerve plantarward, often producing a palpable and audible "click" (Mulder's click) accompanied by sharp, radiating pain into the affected toes.

2. Web Space Compression
Simultaneous compression of the forefoot with one hand and direct plantar-to-dorsal compression of the affected web space with two fingers of the opposite hand will exquisitely localize the pain to the affected interdigital nerve.

Clinical Pearl: The presence of a Mulder's click combined with isolated web space tenderness is highly specific for an interdigital neuroma. Always evaluate adjacent web spaces to rule out multiple neuromas, though concurrent adjacent neuromas are exceedingly rare.
Pathological and Histological Findings
The etiopathogenesis of interdigital neuromas has been the subject of extensive academic debate. Experts differ regarding the exact underlying pathological process, but histological specimens removed from patients consistently demonstrate a pattern of chronic degeneration and fibrosis.
In a strict pathological sense, the term neuroma is incorrect. A true traumatic neuroma exhibits a haphazard, disorganized proliferation of axonal sprouts attempting to bridge a nerve gap. This proliferative axonal sprouting is entirely absent in Morton's neuroma. Instead, the gross enlargement of the nerve is accounted for by the massive deposition of hyaline and collagenous material.
Therefore, the term interdigital neuritis or perineural fibroma is far more scientifically accurate. The pathological process is fundamentally degenerative, driven by repetitive microtrauma against the unyielding deep transverse intermetatarsal ligament.
Summary of Microscopic Pathology
Histological examination of excised interdigital neuromas reveals a consistent triad of perineural fibrosis, vascular degeneration, and axonal loss. The following list summarizes the hallmark pathological findings:
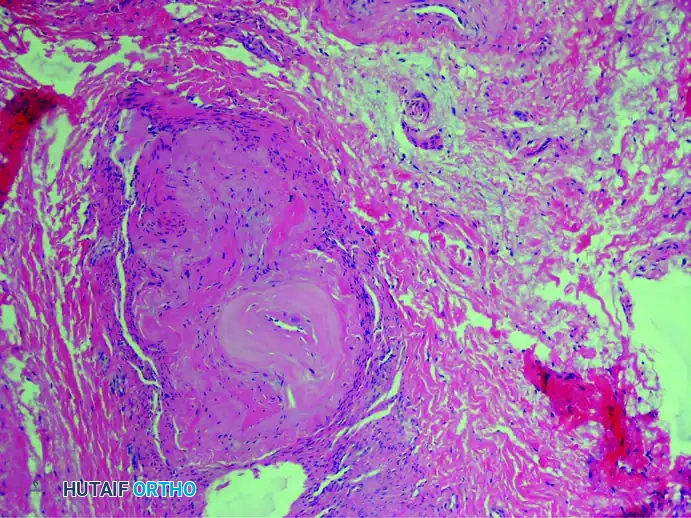
1. Perineural Fibrosis
The interdigital nerve is greatly thickened by dense, concentric layers of perineural fibrous tissue. This fibrosis acts as a constricting scar around the nerve fascicles.
(Hematoxylin and eosin stain demonstrating severe perineural fibrosis)
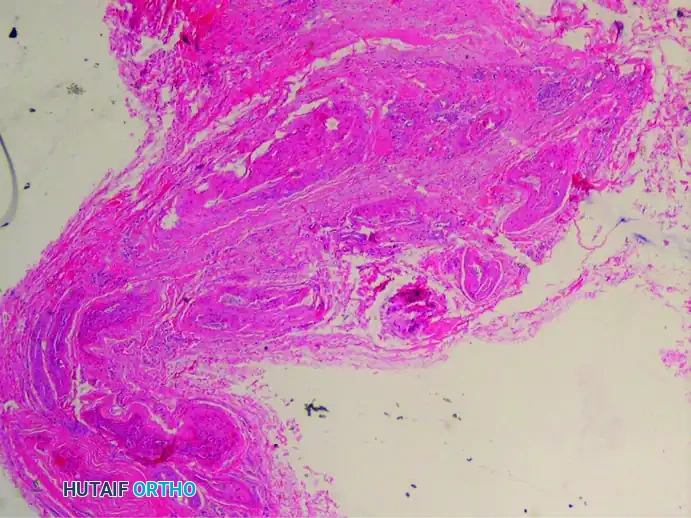
2. Vascular Degeneration (Vasa Nervorum)
There is a markedly increased number of intrafascicular arterioles. However, these vessels are not healthy; they exhibit thickened, hyalinized walls caused by the deposition of multiple layers of basement membranes. Degenerative changes such as the fraying and duplication of the internal elastic lamina are frequently observed, leading to localized nerve ischemia.
(Verhoeff-van Gieson stain highlighting vascular degenerative changes)
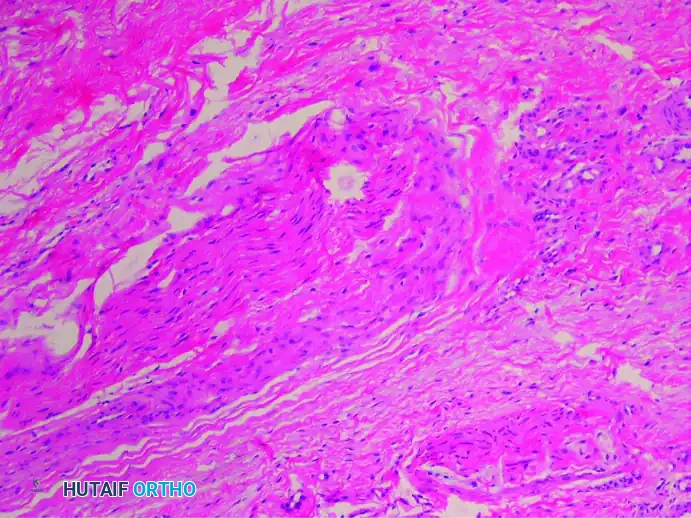
3. Axonal Demyelinization and Degeneration
Secondary to the chronic compression and ischemia, there is profound demyelinization and degeneration of the nerve fibers. Histological stains specific for nerve tissue reveal a significant decrease in the total number of viable axis cylinders.
(Bielschowsky stain showing missing axons and severe degenerative changes)
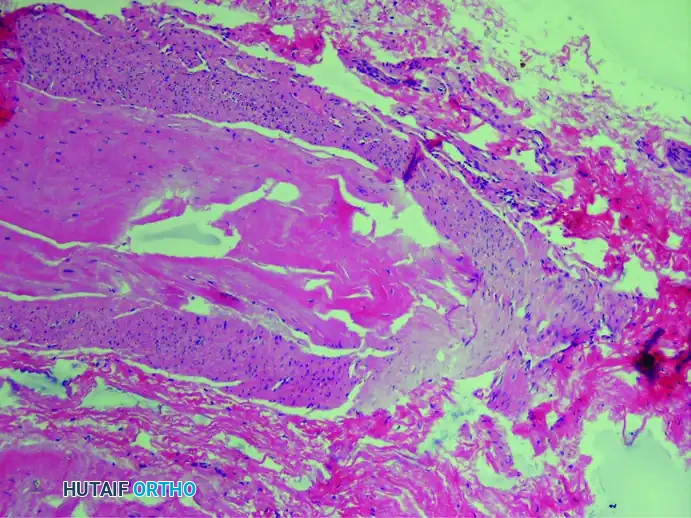
4. Associated Bursal Tissue
It is highly frequent to find reactive bursal tissue accompanying the excised nerve specimen. This intermetatarsal bursitis is often the initial source of inflammation that subsequently leads to the perineural fibrosis of the adjacent nerve.
(Hematoxylin and eosin stain showing an associated small bursa)
5. Additional Histological Features
* Endoneural Edema: Chronic swelling within the nerve fascicles.
* Absence of Inflammatory Cells: Unlike acute neuritis, chronic interdigital neuromas lack a significant presence of lymphocytes or macrophages, confirming the process is degenerative rather than actively inflammatory.
* Amorphous Eosinophilic Deposition: With the aid of electron microscopy, Lassmann identified the deposition of an amorphous, eosinophilic material built up by filaments of tubular structure. While this finding is present in normal nerves, it is exponentially increased in interdigital neuromas.
Vascular Considerations in Neurectomy
When performing a surgical neurectomy for an interdigital neuroma, surgeons must be aware of the intimate relationship between the common digital nerve and the digital artery.
Su et al. conducted a landmark study examining 674 consecutive pathologic specimens obtained after neurectomy for interdigital neuroma. They found that a digital artery was inadvertently excised and accompanied the nerve in 39% of the specimens.
Surgical Warning: Despite the high rate of concomitant digital artery resection during neurectomy, clinical complications (such as digital ischemia) are exceedingly rare. This is due to the extensive and robust vascular collateralization of the digital vessels in the forefoot. However, meticulous dissection should still be employed to separate the artery from the nerve whenever anatomically feasible.
Etiology and Biomechanics of Degeneration
The exact etiology of this degenerative process remains multifactorial, but the leading consensus points to biomechanical entrapment.
During the terminal stance phase of the gait cycle, the metatarsophalangeal joints are maximally dorsiflexed. This action stretches the common digital nerve tightly across the distal edge of the deep transverse intermetatarsal ligament. Repetitive microtrauma from this bowstringing effect, combined with the compressive forces of narrow toe-box footwear, initiates a cascade of localized trauma.
The resulting sequence of events includes:
1. Repetitive Microtrauma: Mechanical shearing against the ligament.
2. Intermetatarsal Bursitis: Reactive inflammation of the adjacent bursa.
3. Ischemia: Occlusion of the vasa nervorum due to pressure and vascular wall hypertrophy.
4. Endoneural Edema: Swelling within the nerve fascicles due to ischemic damage.
5. Perineural Fibrosis: The final, irreversible stage of collagenous deposition and nerve enlargement.
Ultimately, these combined factors are responsible for the intractable symptoms of interdigital neuritis. Understanding this pathophysiology is critical for the orthopedic surgeon, as it underscores why conservative treatments (like metatarsal pads that splay the metatarsal heads and relieve ligamentous tension) can be effective in early stages, while advanced fibrotic stages almost universally require surgical excision or ligamentous release.
You Might Also Like

