Comprehensive Management of Acute Ankle Ligament Injuries and Internal Derangements
Key Takeaway
Acute ankle ligament injuries represent the most common musculoskeletal trauma, predominantly involving the lateral ligamentous complex. Accurate diagnosis relies on delayed physical examination and targeted stress radiography. While most injuries resolve with functional rehabilitation, high-demand athletes with demonstrable mechanical instability may require anatomic surgical repair. This guide details the surgical anatomy, biomechanics, diagnostic algorithms, and operative techniques for managing complex lateral, medial, and syndesmotic ankle disruptions.
Introduction to Ankle Injuries
Other than fractures or dislocations, acute trauma to the ankle produces at least three distinct categories of joint affections: (1) acute severe ligamentous injuries resulting in frank joint disruptions, (2) ligamentous injuries of lesser magnitude stemming from a single traumatic episode or repetitive “overuse” that produce nondisruptive, microscopic abnormalities of the joint capsule, and (3) the acute aggravation of preexisting joint abnormalities. Furthermore, certain intra-articular conditions may have trauma as an inciting etiology, yet the clinical history may remain nonspecific long after the acute symptoms of injury have subsided (e.g., chondromalacia, osteochondritis dissecans, or osteochondral lesions of the talus).
Sprains constitute approximately 85% of all ankle injuries, with 85% of these specifically involving a lateral inversion mechanism. In the context of athletic trauma, ankle injuries account for 14% to 21% of all sports-related injuries. Notably, approximately 40% of basketball injuries and 25% of soccer injuries involve the ankle joint. High-impact sports such as volleyball and football also carry an exceptionally high risk of ankle ligament disruption. Epidemiological data suggests that, compared with men, women exhibit a slightly higher incidence of ankle injuries when participating in similar sporting activities.
Classification of Ankle Ligament Injuries
Ankle ligamentous injuries have traditionally been classified by O’Donoghue into three distinct categories based on pathological severity:
* Type I Sprain: Minor ligamentous “stretch” injuries with no macroscopic tearing.
* Type II Sprain: Incomplete or partial macroscopic ligamentous tears.
* Type III Sprain: Complete disruption of the ligament or ligamentous complex.
While anatomically descriptive, Clanton suggested that a more practical, treatment-oriented classification should be based on the dynamic stability of the ankle as determined by clinical stress testing.
Clinical Pearl: Clanton’s Classification of Ankle Ligament Injury
* Type I: Stable ankle to clinical testing (examination under anesthesia if necessary).
* Type II: Unstable ankle with a positive anterior drawer test, positive talar tilt test, or both.
* Grade 1: Nonathlete or older patient — managed with functional treatment.
* Grade 2: Athlete or high-demand patient.
* Type A: Negative radiograph stress test — functional treatment.
* Type B: Positive tibiotalar stress test — surgical repair indicated.
* Type C: Subtalar instability — functional treatment.
Surgical Anatomy and Biomechanics
A profound understanding of the ligamentous and muscular structures surrounding the ankle is paramount for accurate diagnosis and successful surgical intervention. Eversion and abduction of the foot may result in disruption of the medial deltoid ligament; however, inversion stress far more commonly results in ligamentous disruption on the lateral aspect of the ankle.
The Medial Ligamentous Complex (Deltoid Ligament)
Stabilizing the medial side of the ankle anteriorly and posteriorly is the robust, flat, triangular deltoid ligament, which consists of five distinct components divided into superficial and deep layers.
The deep portion of the deltoid ligament is biomechanically the most critical, providing the greatest restraint against lateral translation of the talus. It comprises two components: the anterior and posterior deep tibiotalar ligaments, which attach to the undersurface of the medial malleolus and the body of the talus. Both deep components are intra-articular but extrasynovial. The posterior deep tibiotalar ligament is the strongest component of the entire deltoid complex.
The superficial portion of the deltoid ligament consists of three components:
1. The tibionavicular component anteriorly.
2. The tibiocalcaneal component centrally.
3. The posterior tibiotalar component posteriorly.
Together, the superficial and deep components equally resist valgus tilting of the talus and serve as secondary restraints against anterior translation of the talus.
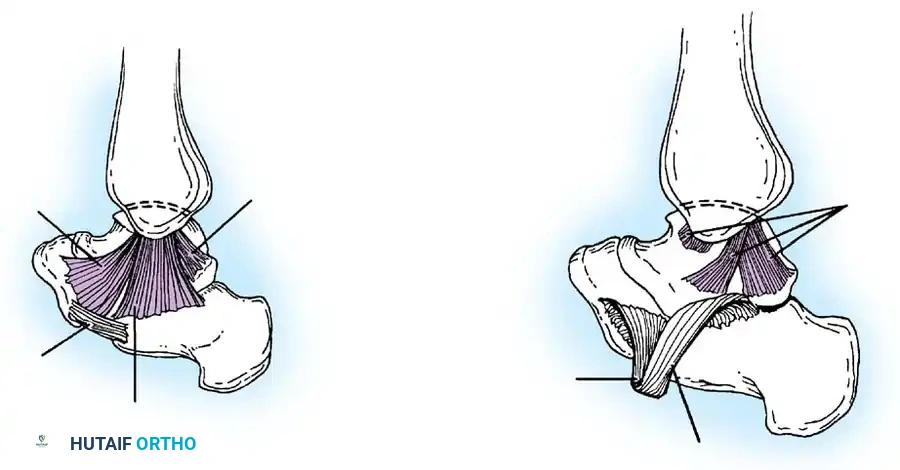
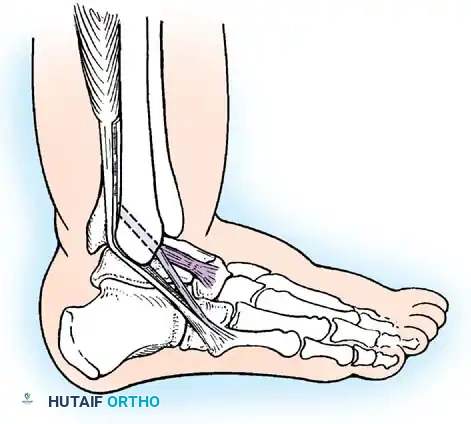
The Lateral Ligamentous Complex
Laterally, three primary ligaments stabilize the ankle, varying significantly in structure, strength, and biomechanical function.
- Anterior Talofibular Ligament (ATFL): Measuring 2 to 2.5 mm thick, 15 to 20 mm long, and 6 to 8 mm wide, the ATFL attaches posteriorly to the anterior border of the lateral malleolus and anteriorly to the neck of the talus, blending with the anterolateral joint capsule. It is the weakest and most frequently injured of the lateral ligaments. Its primary biomechanical function is to resist anterior translation of the talus within the mortise.
- Calcaneofibular Ligament (CFL): Measuring 20 to 25 mm long and 6 to 8 mm wide, the CFL is stronger than the ATFL. It attaches superiorly to the tip of the lateral malleolus, extends deep to the peroneal tendons, and inserts inferiorly on the lateral surface of the calcaneus. Notably, it is the only lateral ligament that is strictly extracapsular.
- Posterior Talofibular Ligament (PTFL): Measuring 30 mm long, 5 mm wide, and 5 to 8 mm thick, the PTFL is the strongest of the lateral ligaments. It attaches anteriorly to the digital fossa of the fibula and posteriorly to the lateral tubercle on the posterior aspect of the talus.
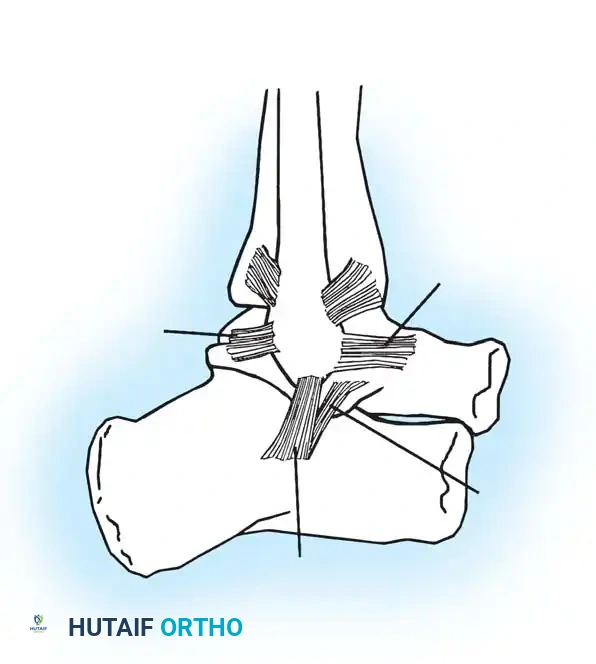
The Tibiofibular Syndesmosis
Maintaining the critical relationship between the distal tibia and fibula is the syndesmosis, a complex consisting of four primary components.
- Anterior Inferior Tibiofibular Ligament (AITFL): Attaches medially to the anterior tibial tubercle (Chaput's tubercle), extends inferiorly and laterally, and inserts on the anterior fibula (Wagstaffe's tubercle). Occasionally, a distal slip of this ligament (Baxter's ligament) may cause anterolateral impingement symptoms against the talus.
- Posterior Inferior Tibiofibular Ligament (PITFL): The strongest component of the syndesmosis. It runs in a similar oblique direction as the AITFL, stabilizing the posterior mortise.
- Inferior Transverse Tibiofibular Ligament: Located deep and inferior to the PITFL. On its anterior surface, it forms a labrum that articulates with the posterolateral talus, effectively deepening the tibiotalar joint.
- Interosseous Tibiofibular Ligament: Attaches to the contiguous rough surfaces of the tibia and fibula, continuous with the interosseous membrane proximally.
Surgical Warning: The interosseous membrane itself is not considered part of the true syndesmotic ligamentous complex. With dorsiflexion of the ankle, the intact syndesmosis allows the fibula to translate laterally, rotate externally, and migrate proximally. This complex also allows the fibula to share approximately 16% of the axial load.
Clinical Diagnosis and Evaluation
A meticulous physical examination is essential to avoid misdiagnosis, particularly in differentiating between isolated lateral sprains and complex syndesmotic or subtalar injuries.
The following structures must be systematically palpated:
* Anterior tibiofibular, calcaneofibular, bifurcate, syndesmotic, and deltoid ligaments.
* Medial and lateral malleoli.
* Base of the fifth metatarsal and the insertion of the peroneus tertius.
* Anterior process of the calcaneus and lateral process of the talus.
* Achilles, peroneal, posterior tibial, flexor hallucis longus, and flexor digitorum longus tendons.
Frey et al. demonstrated that physical examination is 100% accurate in diagnosing Grade III ligament injuries but only 25% accurate for Grade II injuries when compared with MRI findings. Clinicians frequently underestimate the extent of capsuloligamentous damage in Grade II tears.
Van Dijk et al. suggested that diagnostic accuracy significantly improves if the physical examination is delayed until 5 days post-injury rather than performed within the first 48 hours. A delayed examination yields diagnostic information equal to that of arthrography while causing considerably less discomfort to the patient.
When instability is clinically inapparent, the surgeon must determine:
1. Is a ligament completely ruptured (Grade III sprain)?
2. How many ligaments, particularly on the lateral side, are completely disrupted?
Clinical Pearl: Diagnosis by stressing the ankle for instability without anesthesia is often difficult due to muscular guarding. Injection of local anesthetic into the peroneal sheath and lateral gutter of the ankle prior to provocative maneuvers significantly improves the reliability of the examination by eliminating pain-induced muscle spasm.
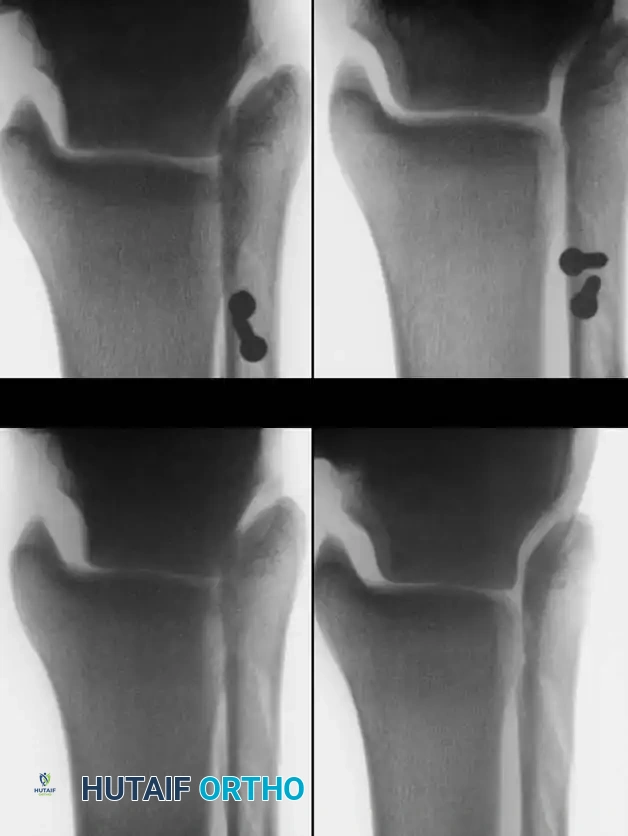
Provocative Maneuvers and Stress Radiography
Inversion/eversion stress testing and anteroposterior stress testing (anterior drawer sign) are critical for evaluating acute and chronic instability. However, stress radiographs must demonstrate a statistically significant difference between the injured and contralateral normal ankle to be considered diagnostic.
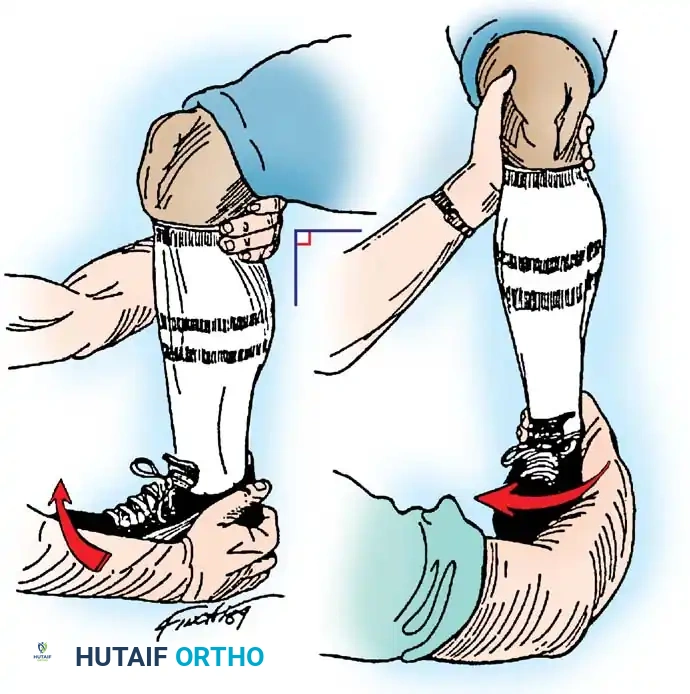
Anteroposterior Stress Test (Anterior Drawer Sign)
Broström, Castaing, and Delplace heavily emphasized the anterior drawer sign as the primary indicator of an ATFL tear.

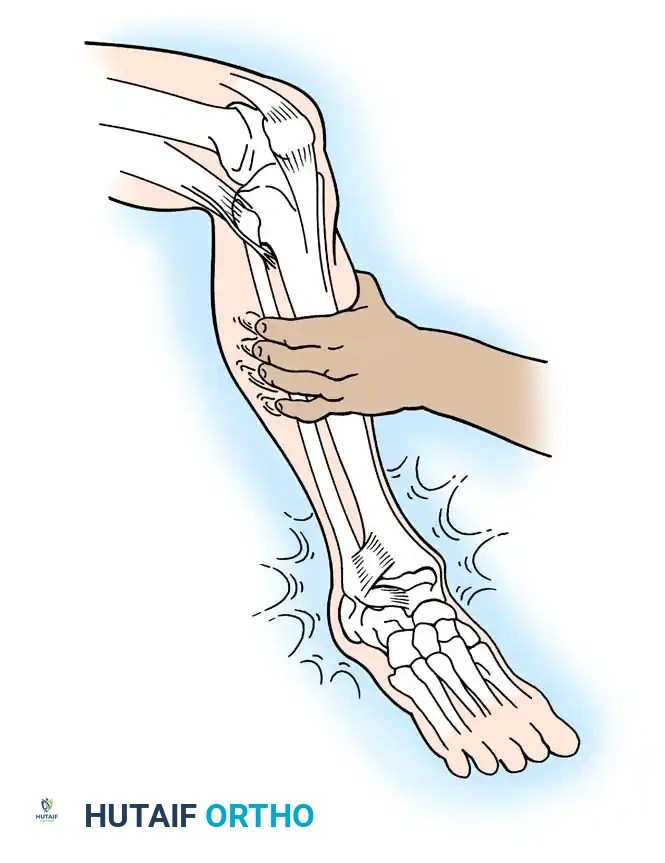
Clinically, the maneuver is performed by placing the tip of the thumb on the anterior aspect of the lateral malleolus while palpating the lateral talar process with the base of the thumb. With gentle anterior stress applied to the heel while stabilizing the tibia, the surgeon assesses the degree of anterior translation of the talus relative to the tibial plafond.

Tohyama et al., in a rigorous cadaveric study, demonstrated that applying 30 N of force during the anteroposterior stress test produced a more reliable injured-to-normal displacement ratio than applying 60 N of force. They recommended utilizing a relatively low-magnitude load when evaluating ATFL integrity to prevent secondary restraints from masking the laxity.
Anderson and LeCocq stated that 3 mm of forward talar displacement on stress radiographs is pathological and indicates lateral ligamentous rupture. However, the clinical sensation of the talus subluxating out of the mortise (the "suction sign") is often more diagnostically valuable than absolute millimeter measurements.
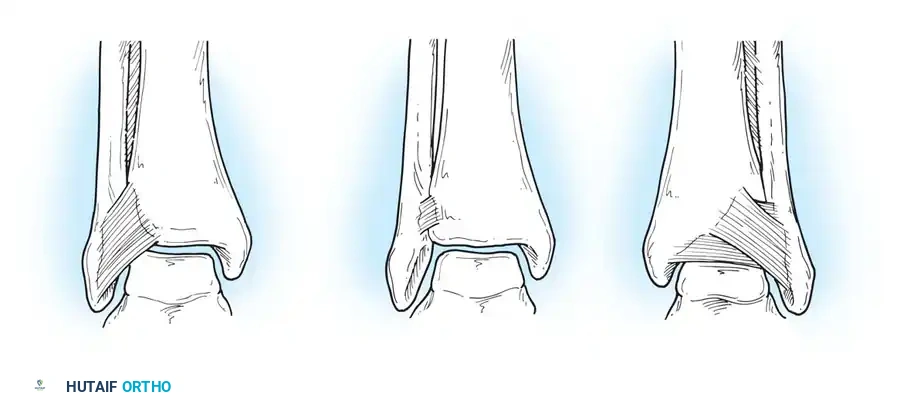
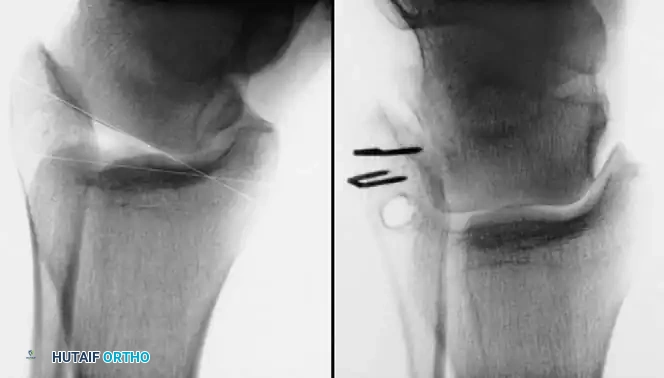
Inversion and Eversion Stress Tests (Talar Tilt)
Complete rupture of the deltoid ligament, including the deep portion, is rare in isolation. When the deltoid is completely ruptured in conjunction with a syndesmotic tear or lateral malleolus fracture, the talus shifts laterally with eversion stress.

If the lateral ligaments are completely disrupted, the talus tilts abnormally within the mortise under inversion stress. This stress is best applied with the ankle in slight plantarflexion to isolate the ATFL.
- Bonnin's Criteria: A talar tilt of 15 degrees indicates isolated ATFL rupture; 15 to 30 degrees indicates combined ATFL and CFL rupture; >30 degrees indicates rupture of all three lateral ligaments.
- Black's Criteria: Found no absolute clear-cut endpoint but noted that a talar tilt of less than 10 degrees is generally consistent with an isolated ATFL injury.

Hollis et al. noted that if an anteroposterior drawer test shows less laxity in dorsiflexion than in neutral, an isolated ATFL tear is likely. Conversely, laxity present in both 15 degrees of dorsiflexion and neutral indicates combined ATFL and CFL disruption.
Meyer et al. warned that subtalar sprains frequently masquerade as ankle sprains. Negative stress radiographs in the presence of severe clinical instability should raise high suspicion for an underlying subtalar ligamentous disruption (e.g., interosseous talocalcaneal ligament).
Operative Management of Acute Ligamentous Injuries
While the vast majority of acute ankle sprains are managed successfully with functional rehabilitation, surgical intervention is indicated for high-demand athletes with severe Grade III multi-ligamentous disruptions, cases of chronic mechanical instability failing conservative care, and injuries involving syndesmotic diastasis or displaced osteochondral fractures.
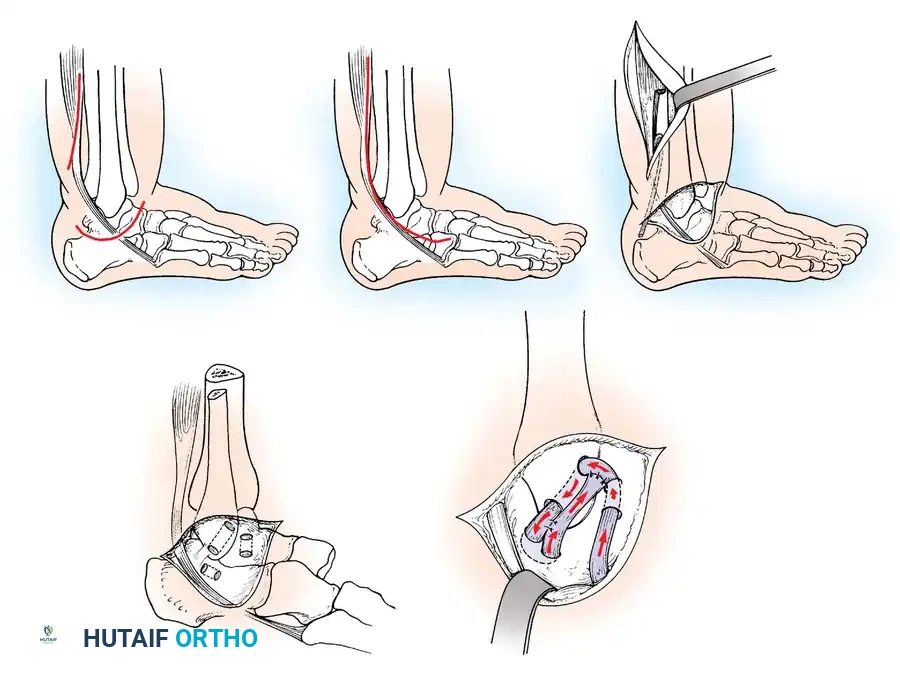
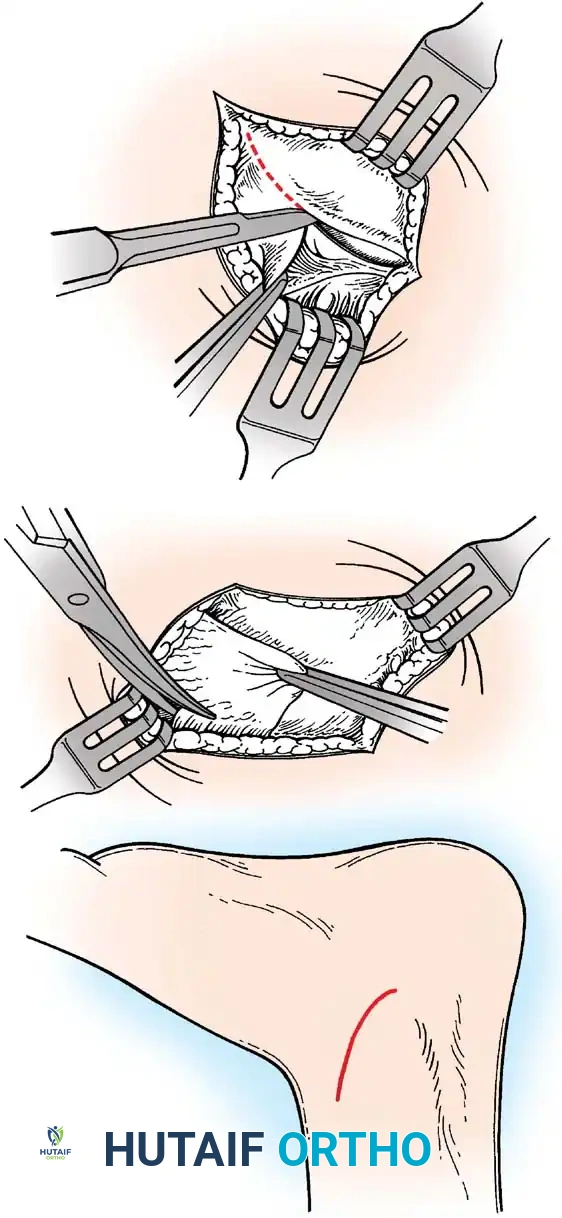
Repair of Acute Rupture of the Lateral Ligaments
The modified Broström-Gould procedure remains the gold standard for anatomic repair of the lateral ligamentous complex.
Surgical Technique:
1. Positioning: The patient is placed supine with a bump under the ipsilateral hip to internally rotate the leg, bringing the lateral malleolus into direct view. A thigh tourniquet is applied.
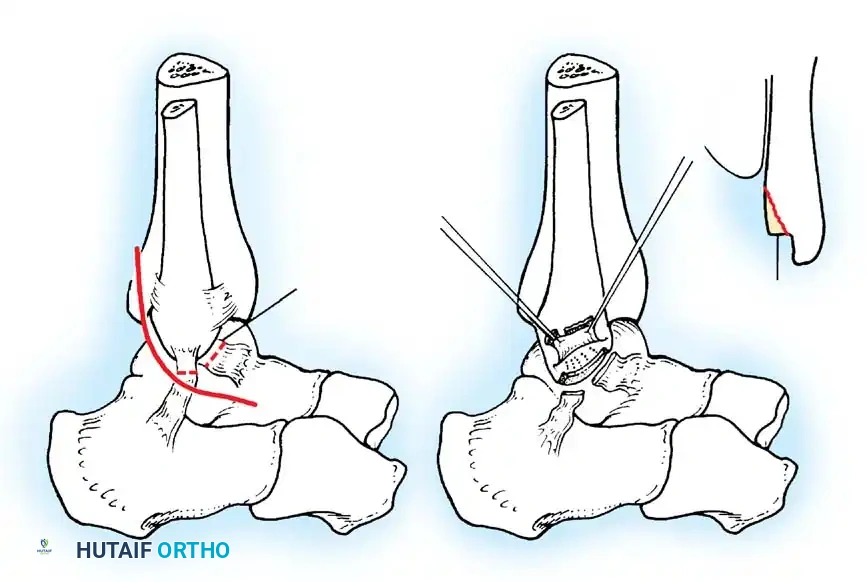
2. Incision: A 4- to 5-cm curvilinear incision is made along the anterior border of the distal fibula, extending toward the sinus tarsi.
3. Dissection: Care is taken to identify and protect the intermediate dorsal cutaneous branch of the superficial peroneal nerve superiorly and the sural nerve inferiorly.
4. Capsulotomy: The extensor retinaculum is identified and mobilized. A vertical arthrotomy is performed 2 mm anterior to the fibular margin, leaving a small cuff of tissue for repair.
5. Joint Inspection: The joint is inspected for osteochondral lesions or loose bodies.
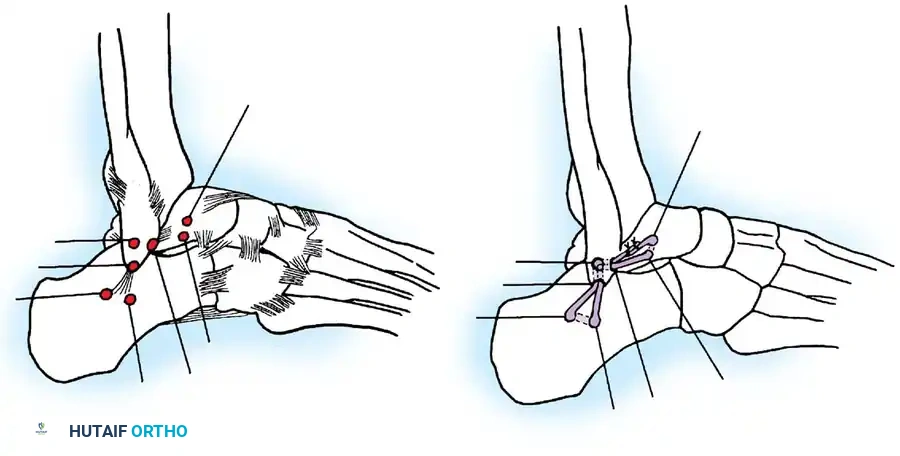
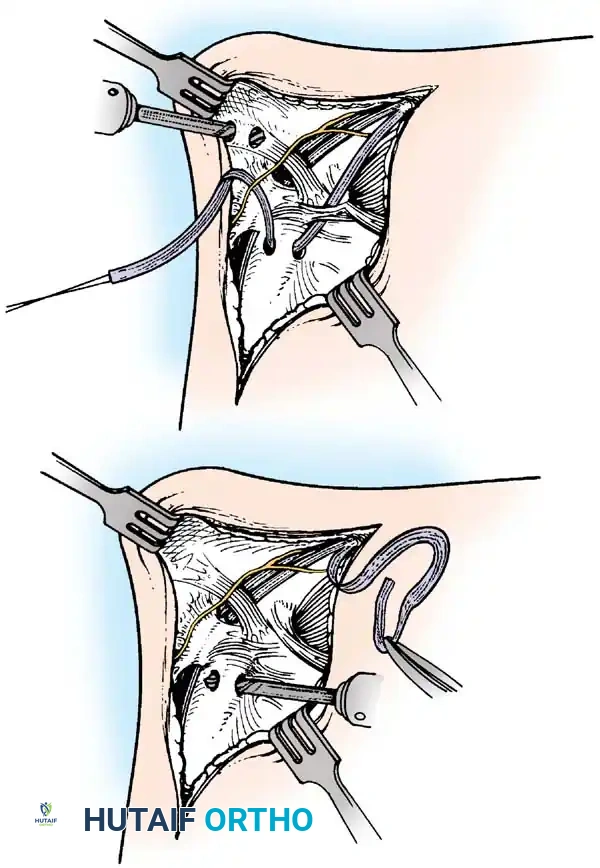
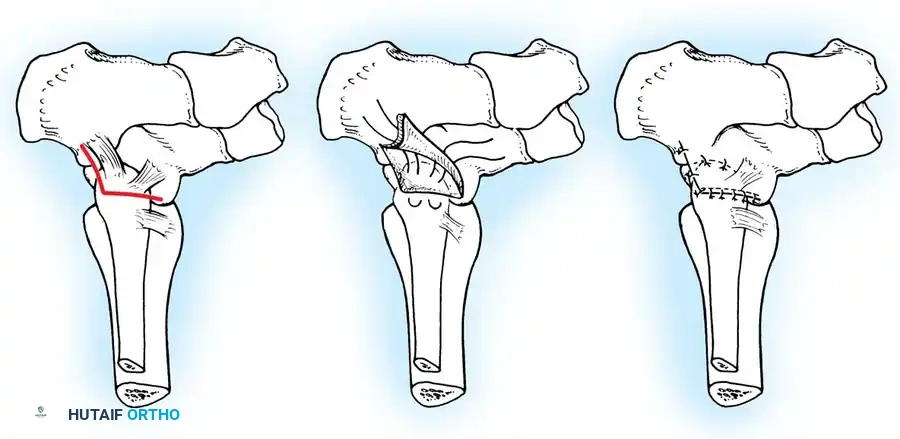
6. Ligament Repair: The torn ends of the ATFL and CFL are identified. If the tissue is robust, direct end-to-end repair is performed using non-absorbable sutures (e.g., 0 or 2-0 FiberWire). If the ligaments are avulsed from the fibula, suture anchors (typically 2.5 mm to 3.0 mm) are placed into the anterior border of the lateral malleolus.
7. Gould Modification: The inferior extensor retinaculum is mobilized and advanced proximally and laterally over the repaired ligaments, suturing it to the fibular periosteum. This imbrication reinforces the repair, limits inversion, and helps address subtalar instability.
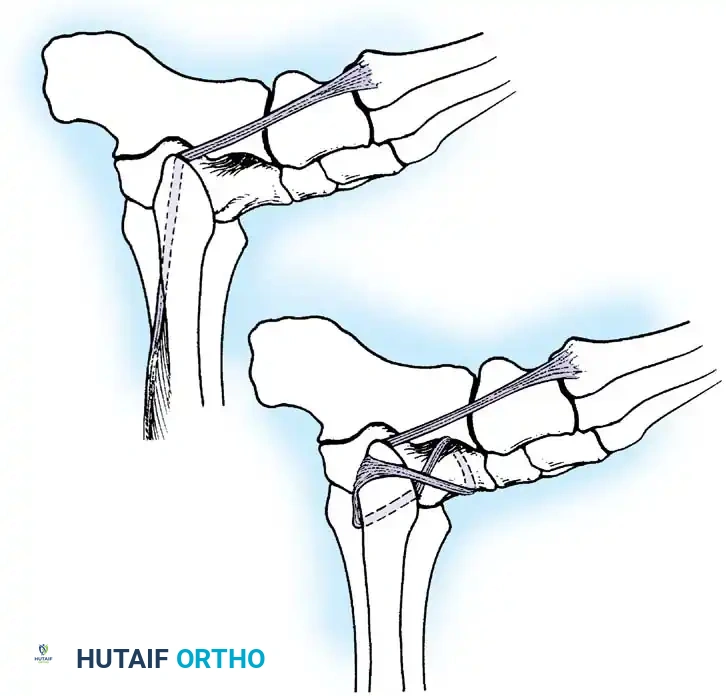
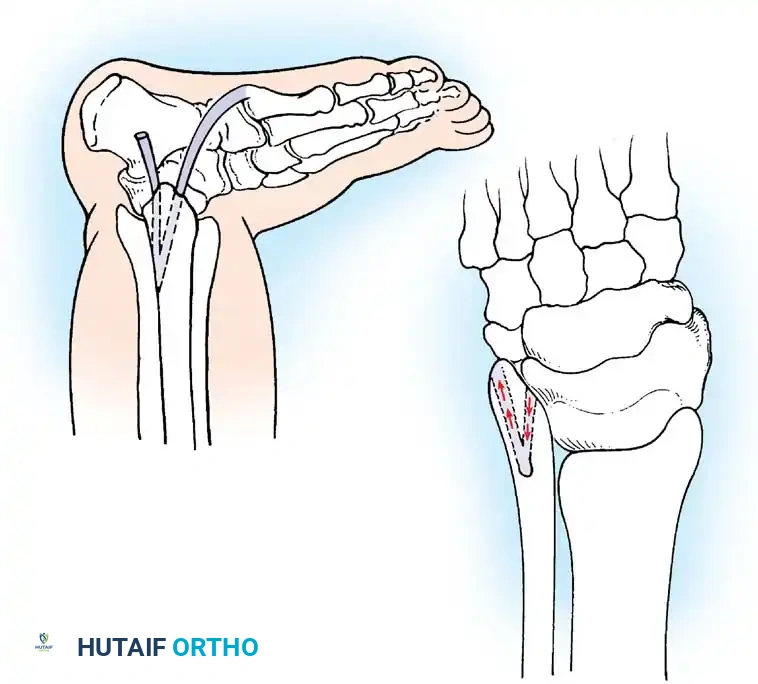
For chronic instability with severely attenuated tissues, non-anatomic tenodesis (e.g., Chrisman-Snook or Watson-Jones) or anatomic reconstruction using allograft/autograft may be required.

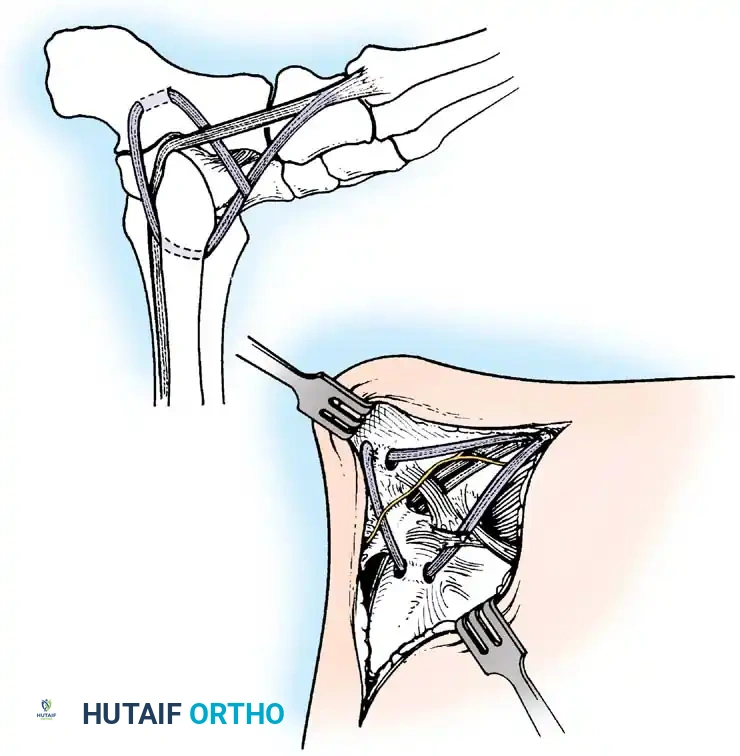
Repair of Acute Rupture of the Deltoid Ligament
Isolated surgical repair of the deltoid ligament is rarely indicated. However, in the setting of a bimalleolar equivalent fracture (fibular fracture with complete deltoid rupture and lateral talar shift), the deltoid may become incarcerated within the medial clear space, preventing anatomic reduction of the mortise.
Surgical Technique:
1. A medial longitudinal incision is made centered over the medial malleolus.
2. The joint is cleared of hematoma and the interposed deltoid ligament is extracted from the mortise.
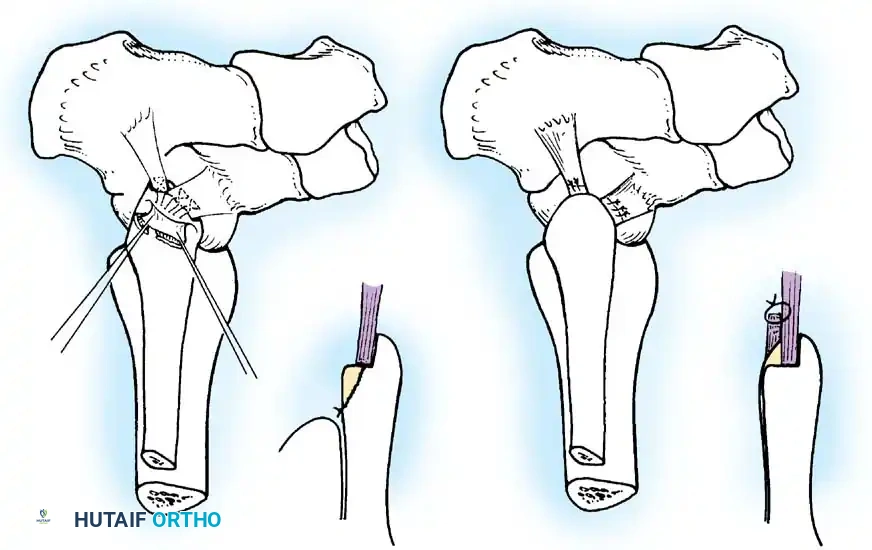
3. The deep posterior tibiotalar ligament is repaired first using suture anchors placed into the medial talar body or medial malleolus.
4. The superficial deltoid is then imbricated and repaired in a pants-over-vest fashion.
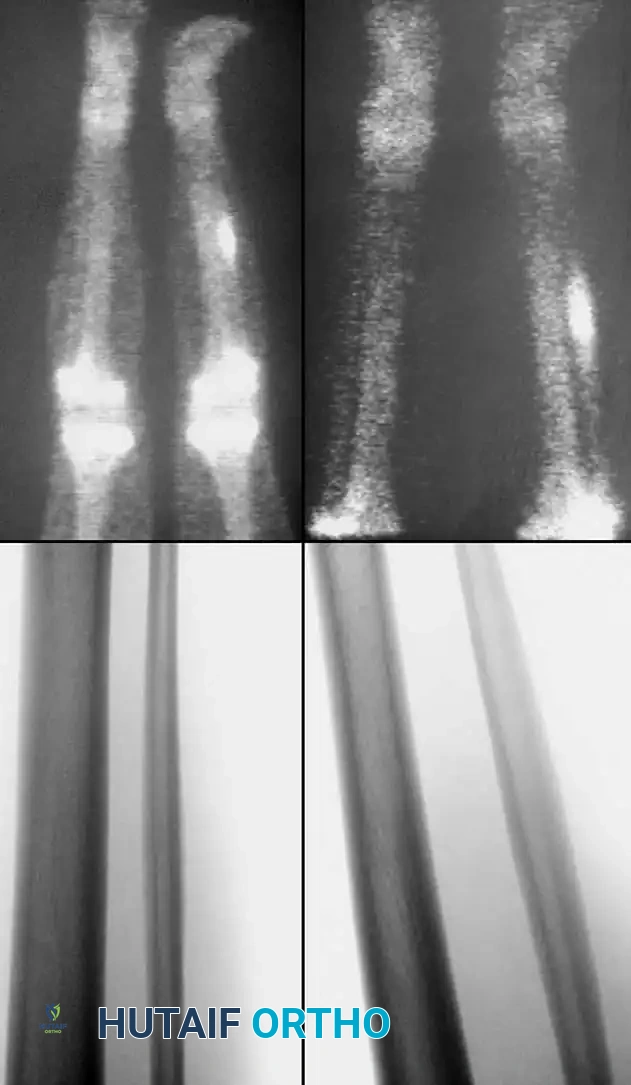
Repair of the Distal Tibiofibular Syndesmosis
Associated Surgical & Radiographic Imaging


You Might Also Like

