Anesthesia and Surgical Preparation in Upper Extremity Surgery

Key Takeaway
The selection of anesthesia in hand and upper extremity surgery is critical for achieving a painless, motionless operative field. This guide details the indications for general versus regional anesthesia, the pharmacology of local anesthetics, ultrasound-guided brachial plexus blocks, and essential surgical preparation. Mastery of these principles minimizes complications, optimizes microsurgical precision, and significantly improves postoperative patient outcomes and rehabilitation trajectories.
PRINCIPLES OF ANESTHESIA IN UPPER EXTREMITY SURGERY
Unsatisfactory anesthesia for hand and upper extremity operations prevents the surgeon from accomplishing their operative goals and is highly likely to compromise the final surgical result. The intricate anatomy of the hand demands absolute microsurgical precision. For accurate and precise work, the operative extremity must be completely motionless, the procedure must be entirely painless, and the patient must remain hemodynamically stable and comfortable throughout the duration of the case.
All anesthetic techniques carry inherent physiological risks. The selection of the optimal technique depends on a triad of factors: the specific physiological and psychological needs of the patient, the technical requirements of the surgeon, and the expertise of the anesthesiologist. Consequently, the choice of anesthesia must never be an afterthought; it must be an integral component of comprehensive preoperative planning.
Clinical Pearl: The ideal anesthetic plan for hand surgery provides dense sensory blockade, profound motor relaxation, and a sympathetic block that induces local vasodilation—an invaluable asset in microvascular repair and flap perfusion.
INDICATIONS FOR GENERAL ANESTHESIA
While regional anesthesia has become the gold standard for many upper extremity procedures, general anesthesia remains the preferred modality in specific clinical scenarios. Factors that strongly favor the administration of general anesthesia include:
- Extensive and Prolonged Operations: Procedures anticipated to exceed the duration of long-acting regional blocks (typically >6-8 hours), such as major replantations or complex brachial plexus reconstructions.
- Concurrent Procedures: Operations requiring simultaneous surgical intervention on other parts of the body, such as the chest, abdomen, or the harvesting of distant tissue grafts (e.g., fibula free flaps, iliac crest bone grafts).
- Pediatric Populations: Extensive operations in young children who cannot reliably cooperate or remain immobile under regional anesthesia alone.
- Local Contraindications: The presence of severe infection, cellulitis, or malignancy in the anatomical region where a regional block would be administered (e.g., axillary infection precluding an axillary block).
- Patient Preference and Psychology: Particularly uneasy, claustrophobic, or highly anxious patients who may not tolerate the operating room environment while awake.
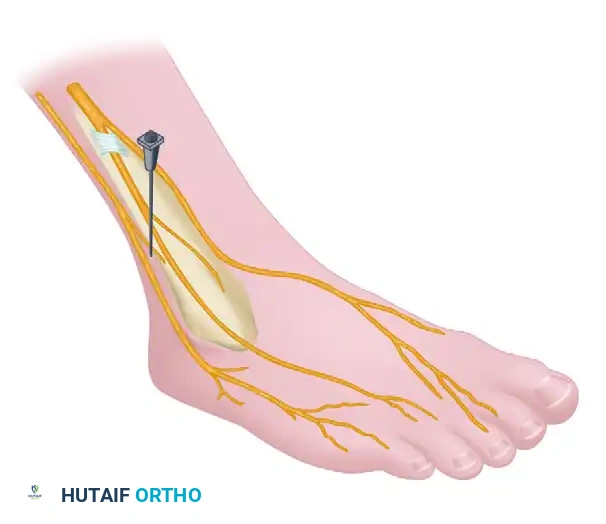
REGIONAL ANESTHESIA: THE BRACHIAL PLEXUS BLOCK
Regional anesthesia offers profound advantages in hand and upper extremity surgery, fundamentally altering the perioperative experience.
Advantages of Regional Blockade
Satisfactory regional anesthesia can be safely achieved for emergency procedures performed on patients with a full stomach, significantly mitigating the risk of aspiration associated with general anesthesia. In both emergency and elective operations, a regional anesthetic effectively blocks vasoconstrictive afferent nociceptive impulses from the surgical wound. This sympathetic blockade results in maximal vasodilation, improving tissue perfusion and facilitating microvascular anastomoses. Furthermore, it avoids many of the unpleasant postoperative complications of general anesthesia, such as postoperative nausea and vomiting (PONV), sore throat, and cognitive dysfunction.
Outpatient surgery is vastly facilitated by regional anesthetic blocks, which provide extended postoperative analgesia and reduce the immediate need for intensive postoperative nursing care.
Ultrasound Guidance vs. Nerve Stimulation
The advent of high-frequency ultrasound has revolutionized regional anesthesia. A prospective study of the multiple-injection technique for axillary blocks demonstrated that ultrasound guidance results in significantly fewer needle passes, a shorter time to the onset of surgical anesthesia, and less procedure-related pain compared to traditional nerve stimulation techniques.
Despite its superiority, ultrasound guidance has limitations, including equipment availability, a limited two-dimensional plane of view, and highly operator-dependent image quality. Mastery of sonoanatomy is mandatory for the modern anesthesiologist and orthopaedic surgeon.
Approaches to the Brachial Plexus
- Interscalene Block: Ideal for shoulder and proximal humerus surgery. It frequently spares the ulnar nerve (C8-T1), making it suboptimal for hand surgery.
- Supraclavicular Block: Often termed the "spinal of the arm," it provides dense, rapid-onset anesthesia of the entire upper extremity distal to the shoulder. It is performed at the level of the trunks/divisions.
- Infraclavicular Block: Performed at the cord level. Excellent for procedures of the elbow, forearm, and hand, and highly suitable for continuous catheter placement due to the depth of the block and stability of the catheter.
- Axillary Block: Performed at the terminal branch level. Highly effective for forearm and hand surgery. It avoids the risk of pneumothorax but requires separate blockade of the musculocutaneous and intercostobrachial nerves to ensure complete tourniquet tolerance.
Surgical Warning: Contraindications to the axillary brachial plexus block include localized infection in the axilla, axillary lymphadenopathy, and local malignancy.
PHARMACOLOGY OF LOCAL ANESTHETICS
Drugs utilized for local and regional anesthesia must meet specific pharmacokinetic and pharmacodynamic criteria: they should become effective within a few minutes after injection, cause minimal local tissue irritation, and possess a high threshold for systemic toxicity.
Common Agents
- Lidocaine: An amide local anesthetic that fulfills the basic requirements of rapid onset and moderate duration (1-2 hours). It is the workhorse for short procedures.
- Mepivacaine (Carbocaine): Similar to lidocaine but slightly longer acting. It may, however, present a slower onset of action.
- Bupivacaine (Marcaine): Highly favored by many surgeons and anesthesiologists due to its prolonged duration of action. It is effective for 8 hours or longer, providing excellent postoperative analgesia and allowing complex procedures (e.g., axillary blocks for replantation) to proceed without general anesthesia.
- Ropivacaine and Levobupivacaine: Enantiomer-specific derivatives developed to provide the long-acting benefits of bupivacaine but with a significantly reduced profile for cardiac toxicity.
Dosing and Systemic Toxicity
Each of these agents has a strict toxicity level based on milligrams per kilogram (mg/kg) of lean body weight. This must be meticulously calculated prior to administration to prevent Local Anesthetic Systemic Toxicity (LAST).
Maximal Recommended Doses for Brachial Plexus Blocks:
(Note: These amounts serve as guidelines; practitioners must exercise clinical judgment based on patient comorbidities.)
- Bupivacaine: 2.5 mg/kg
- Bupivacaine with epinephrine: 3.0 mg/kg
- Levobupivacaine: 2.0 mg/kg
- Levobupivacaine with epinephrine: 3.0 mg/kg
- Ropivacaine: 2.0 mg/kg
- Ropivacaine with epinephrine: 3.0 mg/kg
Data modified from Bruce BG, Green A, Blaine TA, Wesner LV: Brachial plexus blocks for upper extremity orthopaedic surgery, J AAOS 20:38, 2012.
COMPLICATIONS OF REGIONAL ANESTHESIA
While highly safe, complications of brachial plexus blocks do occur, albeit in fewer than 1% of cases.
Systemic Complications
Systemic complications are primarily related to inadvertent intravascular injection or exceeding maximum weight-based dosing (LAST). Manifestations range from perioral numbness and tinnitus to catastrophic seizures, respiratory failure, and refractory cardiac arrest. Immediate availability of 20% lipid emulsion therapy is mandatory wherever regional blocks are performed.
Neurologic Complications
Peripheral nerve injury can result from mechanical trauma (needle laceration), catheter-induced trauma, direct drug neurotoxicity, localized ischemia, hematoma compression, or excessive stretch. Fortunately, permanent neurologic sequelae occur in fewer than 1% of patients.
Patients must be counseled preoperatively that transient dysesthesias and "brachialgia" may persist for days to weeks following a brachial plexus block. This is particularly critical for patients whose occupations require fine, unimpeded manipulation of the hands (e.g., musicians, surgeons, jewelers).
Pulmonary Complications
Pneumothorax is the most feared anatomical complication, historically most common with the supraclavicular approach (reported as high as 6% using landmark techniques). It has also been reported with interscalene and infraclavicular blocks. The integration of ultrasound-guided techniques has drastically reduced this risk. A prospective study found zero clinically apparent pneumothoraces in 510 patients who underwent ultrasound-guided supraclavicular blocks.
SURGICAL PREPARATION AND INSTRUMENTATION
The transition from anesthesia to surgical execution requires meticulous preparation of the operative field and instrumentation. Hand surgery demands specialized, delicate instruments designed to minimize tissue trauma.
The Basic Hand Surgery Tray
Standardization of the surgical tray enhances operative flow. The basic tray should contain instruments specifically scaled for the intricate anatomy of the hand.
FIGURE 64-4: Basic instruments for any surgical procedure on the hand. The octagonal knife handle is preferable to a flat handle because the knife is more commonly held by a precision pinch in hand surgery. Instruments shown include the knife handle, small rat-tooth forceps, dissecting scissors, small hemostats, ruler, marking pencil, double-hook Lovejoy retractors, and a probe.
Biomechanical Considerations of Instrumentation:
Notice the design of the scalpel handle in the basic tray. An octagonal knife handle is vastly preferable to the standard flat handle (e.g., a standard #3 handle). In macroscopic orthopaedics, a scalpel is often held in a power grip. In hand surgery, the scalpel is manipulated using a "precision pinch" (lumbrical plus position). The octagonal geometry allows the surgeon to roll the instrument seamlessly between the thumb, index, and long fingers, allowing for sweeping, multidirectional curvilinear incisions without repositioning the wrist.
Instrument Handling: The "Drop Technique"
Efficiency at the surgical field is maintained through the "drop technique." Using this method, the surgeon discards an instrument onto a designated sterile drape area immediately after use, and the scrub nurse returns it to its precise place on the tray. With practice, this allows the surgeon to reach for instruments without diverting their eyes from the microscopic surgical field.
Instruments that are in constant rotation—such as the discarded knife, delicate tissue forceps, and dissecting scissors—are not retrieved by the nurse unless specifically requested. Special instruments, additional knife blades, and fine microsurgical sutures (e.g., 8-0 or 9-0 nylon) should be readily available on a secondary large table so they can be handed quickly to the surgeon upon request.
PATIENT POSITIONING AND OPERATIVE SETUP
Proper positioning of the patient and the upper extremity is as critical as the surgical dissection itself. The patient is typically positioned supine with the operative arm extended onto a radiolucent hand table.
Tourniquet Application
A well-padded pneumatic tourniquet is applied to the proximal arm. Exsanguination is achieved using an Esmarch bandage prior to inflation. The tourniquet provides a bloodless field, which is an absolute prerequisite for identifying microscopic neurovascular structures. Tourniquet time should be strictly monitored, generally not exceeding 120 minutes without a reperfusion interval.
Hand Stabilization and Exposure
Surgical exposure in the hand frequently utilizes zigzag (Bruner) incisions to prevent postoperative flexion contractures across flexion creases. Making these incisions requires precise skin tension.

FIGURE 64-3: Ideal position for the assistant to stabilize the patient’s hand as the surgeon makes a zigzag incision.
As illustrated, the surgical assistant plays a vital role. The assistant must provide firm, unyielding counter-tension. By stabilizing the digits and applying longitudinal traction, the assistant flattens the palmar skin, allowing the surgeon's octagonal scalpel to glide smoothly through the dermis without skiving or creating jagged, traumatized skin edges. This collaborative tension is the foundation of atraumatic soft tissue handling, which directly correlates with reduced postoperative edema and improved wound healing.
POSTOPERATIVE PROTOCOLS AND CONSIDERATIONS
The postoperative phase begins the moment the surgical dressing is applied. The dressing must be non-constrictive to accommodate anticipated swelling, yet rigid enough (often incorporating a volar plaster splint) to protect tendon or nerve repairs.
Managing Rebound Pain
A significant consideration when utilizing long-acting regional anesthesia (such as bupivacaine or ropivacaine) is the phenomenon of "rebound pain." When the dense sensory block resolves—often abruptly between 8 to 14 hours postoperatively—the patient may experience a sudden, severe onset of nociceptive pain.
To mitigate this, a multimodal analgesic protocol must be initiated before the block wears off. This includes:
1. Scheduled acetaminophen and NSAIDs (if not contraindicated by bone healing or bleeding risks).
2. Oral neuromodulators (e.g., gabapentin) for nerve-related procedures.
3. A short course of oral opioids for breakthrough pain.
4. Thorough patient education regarding the expected timeline of block resolution.
Neurological Monitoring
Because the regional block masks immediate postoperative neurological function, the surgical team must rely on intraoperative anatomical certainty regarding nerve integrity. Once the block dissipates, a thorough neurovascular examination must be documented. Any persistent motor or sensory deficits beyond the expected pharmacological duration of the anesthetic agent warrant immediate clinical evaluation to rule out compressive hematoma, tight dressings, or iatrogenic injury.
You Might Also Like