Amputation for Chronic Osteomyelitis: Indications, Surgical Strategies, and Outcomes
Key Takeaway
Amputation remains a definitive, life-saving intervention for refractory chronic osteomyelitis, particularly when complicated by malignant transformation, severe arterial insufficiency, or profound neurovascular compromise. This surgical guide details the critical indications, preoperative optimization, and step-by-step operative techniques required to achieve a functional, infection-free residual limb. Mastery of these principles ensures optimal prosthetic fitting and restores patient mobility when limb salvage is no longer viable.
INTRODUCTION TO AMPUTATION IN OSTEOMYELITIS
While the contemporary orthopaedic armamentarium heavily favors limb salvage through radical debridement, local antibiotic delivery systems, and complex soft-tissue reconstruction, amputation remains a critical, definitive treatment modality for chronic osteomyelitis. Amputation is performed infrequently for osteomyelitis; however, in carefully selected patients, this definitive form of treatment is vastly preferable to a protracted cycle of multiple failed operations that are unlikely to eradicate the infection.
The decision to amputate is rarely straightforward and requires a nuanced understanding of the patient's physiologic reserve, the anatomical extent of the disease, and the functional potential of the limb. In the context of the Cierny-Mader classification, amputation is most frequently indicated for Type IV (diffuse) osteomyelitis in a C-class host—a patient whose systemic or local comorbidities make the metabolic cost of limb salvage greater than the potential benefit.
Clinical Pearl: The goal of amputation in the setting of chronic osteomyelitis is not merely the extirpation of infected tissue, but the creation of a dynamic, painless, and highly functional residual limb optimized for modern prosthetic wear.
INDICATIONS FOR AMPUTATION
The transition from limb salvage to amputation is dictated by specific, evidence-based clinical thresholds. The primary indications include malignant transformation, irreversible neurovascular compromise, and systemic toxicity.
Malignant Transformation (Marjolin’s Ulcer)
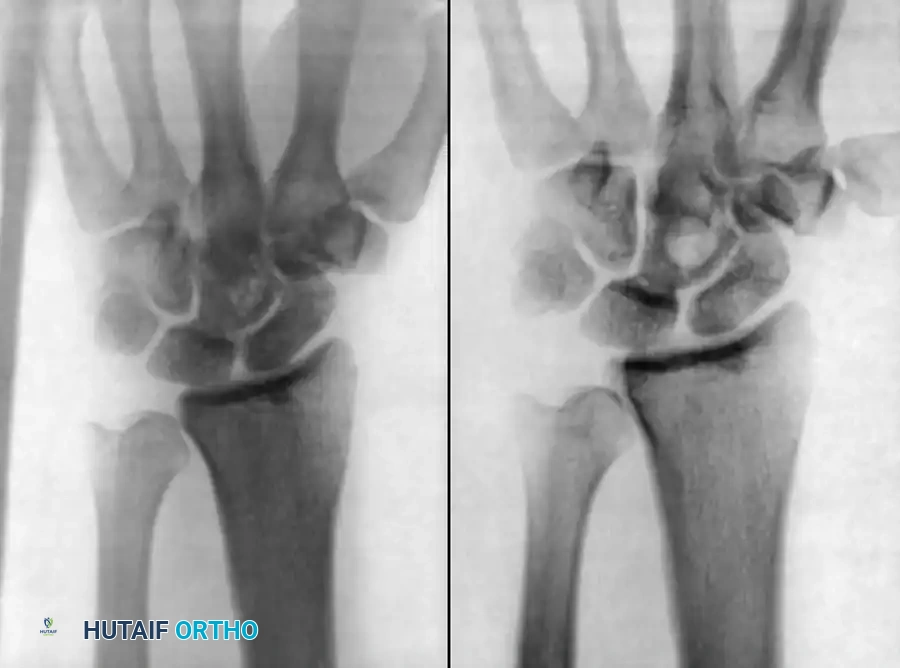
The prevalence of malignancy arising from chronic osteomyelitis has been reported to be between 0.2% to 1.6% of cases. The chronic inflammatory milieu, characterized by continuous cellular turnover and DNA damage within a chronic sinus tract, predisposes the tissue to neoplastic degeneration.
- Squamous Cell Carcinoma (SCC): The vast majority of these malignancies are well-differentiated squamous cell carcinomas arising directly from the epithelialized sinus tract.
- Other Neoplasms: Though rare, reticulum cell carcinoma, fibrosarcoma, angiosarcoma, and basal cell carcinoma have been documented in the literature.
Amputation is the most reliable and oncologically sound means of treating cases of osteomyelitis associated with malignant change. Local resection or limb salvage in the presence of a Marjolin’s ulcer carries an unacceptably high rate of local recurrence and metastatic spread, particularly to regional lymph nodes.
Surgical Warning: Any chronic osteomyelitis sinus tract that exhibits a sudden change in character—such as increased exudate, foul odor, bleeding, exophytic growth, or increasing pain—must undergo multiple deep incisional biopsies to rule out malignant transformation.
The Nonfunctional Limb
Even in the absence of malignancy, a limb may become a mechanical and metabolic liability. Indications for amputation in this category include:
* Arterial Insufficiency: Severe peripheral vascular disease that precludes adequate delivery of systemic antibiotics or the healing of reconstructive flaps.
* Major Nerve Paralysis: A sensate, motor-intact limb is a prerequisite for successful salvage. Profound neuropathy (e.g., sciatic or tibial nerve transection) resulting in an anesthetic, flail extremity inevitably leads to recurrent ulceration and infection.
* Joint Contractures and Stiffness: Severe, rigid contractures (e.g., fixed equinovarus or severe knee flexion contractures >40 degrees) that render the limb nonfunctional and preclude normal biomechanical ambulation.
Refractory Sepsis and Host Exhaustion
In patients presenting with acute-on-chronic exacerbations leading to systemic sepsis, necrotizing soft-tissue infections, or profound physiological exhaustion (the "C-host"), amputation becomes a life-saving, damage-control procedure.
PREOPERATIVE EVALUATION AND OPTIMIZATION
Multidisciplinary Assessment
The decision to amputate requires a multidisciplinary approach involving orthopaedic surgery, infectious disease, vascular surgery, psychology, and prosthetics.
Imaging and Vascular Mapping
- Magnetic Resonance Imaging (MRI): Essential for delineating the proximal extent of intramedullary and extramedullary infection. The amputation level must be planned through healthy, uninfected bone and soft tissue.
- Angiography/Doppler Ultrasound: Critical for assessing the vascular inflow. The selected amputation level must have a measurable transcutaneous oxygen tension (TcPO2) of at least 30-40 mmHg to ensure primary healing of the surgical flaps.
Nutritional and Medical Optimization
Chronic osteomyelitis induces a catabolic state. Preoperative optimization of serum albumin (>3.0 g/dL), total lymphocyte count (>1,500/mm³), and glycemic control (HbA1c < 7.0%) significantly reduces the risk of postoperative wound dehiscence and stump infection.
BIOMECHANICS AND LEVEL SELECTION
The selection of the amputation level is a delicate balance between eradicating the infection and preserving maximal limb length to minimize the energy expenditure of future ambulation.
- Energy Expenditure: A unilateral transtibial amputation (BKA) increases the metabolic cost of walking by 10-25% compared to a non-amputee. A transfemoral amputation (AKA) increases energy expenditure by 60-70%. Therefore, preserving the knee joint is of paramount importance, provided the proximal tibia is free of infection.
- Bone Contouring: The residual bone must be meticulously contoured to distribute forces evenly within the prosthetic socket. Sharp cortical edges will lead to focal pressure necrosis, recurrent ulceration, and secondary infection.
SURGICAL APPROACH: STEP-BY-STEP TECHNIQUE
In the setting of active, purulent osteomyelitis, a two-stage surgical approach is often the safest and most reliable method to prevent infection of the residual limb.
Stage 1: The Open (Guillotine) Amputation
The objective of the first stage is rapid source control and the elimination of the septic burden without closing potentially contaminated tissue.
- Positioning and Preparation: The patient is positioned supine. A pneumatic tourniquet is applied proximally but is not inflated unless life-threatening hemorrhage occurs, as tourniquet ischemia can compromise the assessment of tissue viability and exacerbate local tissue hypoxia.
- Incision and Flap Design: Circular or standard flap incisions are made distal to the planned definitive amputation level. The skin, fascia, and muscle are divided in a single plane or slightly conical fashion.
- Bone Resection: The bone is transected 2 to 3 cm proximal to the soft tissue margin using an oscillating saw. Continuous saline irrigation is applied to prevent thermal necrosis of the bone, which could act as a nidus for recurrent osteomyelitis.
- Neurovascular Management: Major vessels are individually isolated, clamped, and double-ligated with non-absorbable suture. Nerves are drawn distally under gentle tension, ligated, sharply transected, and allowed to retract deep into the proximal muscle beds to prevent terminal neuroma formation at the weight-bearing surface.
- Wound Management: The wound is left entirely open. It is packed with sterile dressings, negative pressure wound therapy (NPWT), or antibiotic-impregnated polymethylmethacrylate (PMMA) beads to deliver high local concentrations of antibiotics.
Pitfall: Attempting primary closure in the presence of active, purulent osteomyelitis or compromised soft-tissue margins almost universally leads to stump infection, wound dehiscence, and the need for revision to a higher, more proximal amputation level.
Stage 2: Definitive Closure and Stump Reconstruction
Once the systemic infection has resolved and the local wound bed demonstrates healthy granulation tissue (typically 7 to 14 days later), the patient is returned to the operating room for definitive closure.
- Debridement and Lavage: The open wound is aggressively irrigated and any residual necrotic tissue is excised.
- Bone Contouring: The bone is shortened to the definitive level. In a transtibial amputation, the anterior cortex of the tibia is beveled at a 45-degree angle, and the fibula is resected 1 to 2 cm proximal to the tibial cut to prevent distal fibular pain during prosthetic loading.
- Myodesis/Myoplasty: To provide a robust, dynamic soft-tissue envelope, a myodesis is performed. The muscle fascia (e.g., the posterior calf musculature in a BKA) is brought forward and sutured directly to the bone via drill holes. This stabilizes the bone within the soft tissue envelope and improves venous return.
- Skin Closure: The skin flaps are approximated without tension. Dog-ears are meticulously excised to ensure a smooth, cylindrical, or conical stump profile. Deep closed-suction drains are placed to prevent hematoma formation.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
Immediate Postoperative Care
- Dressings: A rigid or semi-rigid dressing (e.g., Immediate Postoperative Prosthesis - IPOP) is highly recommended. This controls edema, protects the wound from trauma, and prevents knee flexion contractures.
- Antibiotic Therapy: Systemic antibiotics are tailored based on deep intraoperative cultures. If all infected bone and soft tissue were completely resected with negative margins, a short postoperative course (24-48 hours) is sufficient. If residual microscopic disease is suspected, a 4-to-6-week course of targeted intravenous or highly bioavailable oral antibiotics is mandated.
Rehabilitation Timeline
- Days 1-14: Focus on pain control, edema management, and prevention of joint contractures. Aggressive physical therapy is initiated for upper extremity strengthening and contralateral limb preservation.
- Weeks 3-6: Suture removal occurs once the wound is completely healed (often delayed in vascularly compromised patients). Shrinker socks are applied to mature the stump.
- Weeks 6-10: Once the stump volume has stabilized and the incision is robust, the patient is cast for a preparatory (temporary) prosthesis. Gait training commences.
COMPLICATIONS AND MANAGEMENT
Despite meticulous surgical technique, amputations for chronic osteomyelitis carry a distinct complication profile:
- Recurrent Infection: The most dreaded complication. It usually stems from inadequate proximal resection margins or retained infected bone. Treatment requires prompt surgical debridement and revision to a higher level.
- Wound Dehiscence: Often secondary to premature suture removal, excessive flap tension, or unrecognized arterial insufficiency. Managed with NPWT or surgical revision.
- Phantom Limb Pain and Neuromas: Neuropathic pain can be debilitating. Prevention via high nerve transection and targeted muscle reinnervation (TMR) is key. Established neuromas may require surgical excision and burying of the nerve stump into deep muscle or bone.
- Flexion Contractures: Particularly common at the knee following transtibial amputation. Prevention through rigid dressings, early physical therapy, and avoiding prolonged wheelchair sitting is critical. Severe contractures may render the patient unable to use a prosthesis.
CONCLUSION
Amputation for chronic osteomyelitis is a definitive, highly technical reconstructive procedure rather than a failure of treatment. When indicated by malignant transformation, severe neurovascular compromise, or intractable infection, a meticulously planned and executed amputation can eradicate disease, alleviate chronic suffering, and restore functional independence through modern prosthetic rehabilitation. Mastery of soft-tissue handling, precise bone contouring, and staged surgical principles are paramount to achieving a successful, durable outcome.
You Might Also Like