Comprehensive Management of Pediatric Knee Dislocations and Proximal Tibial Fractures
Key Takeaway
Acute dislocations of the pediatric knee and proximal tibiofibular joint are exceedingly rare but carry significant morbidity, particularly regarding popliteal artery compromise. Management requires meticulous clinical evaluation, advanced imaging, and often surgical intervention for displaced physeal fractures. This guide details the biomechanics, classification systems, and step-by-step operative techniques for proximal tibial fractures, ensuring optimal outcomes and minimizing complications like angular deformity or ischemia.
ACUTE DISLOCATIONS OF THE KNEE AND PROXIMAL TIBIOFIBULAR JOINT
Acute dislocations of the knee and the proximal tibiofibular joint are exceedingly rare in the pediatric population. Unlike adults, where ligamentous failure leads to true tibiofemoral dislocation, the pediatric knee typically fails through the biomechanically weaker physes (growth plates) of the distal femur or proximal tibia. Consequently, what may clinically appear as a knee dislocation in a child is frequently a displaced physeal fracture.
True dislocations of the pediatric knee seldom require surgical treatment for the joint itself, as closed reduction is often successful. Ogden reported a comprehensive series of subluxations and dislocations of the proximal tibiofibular joint, noting that the vast majority can be managed non-operatively. The primary clinical challenge lies in accurately identifying the underlying pathological condition, recognizing subtle radiographic changes, and ruling out limb-threatening vascular compromise.
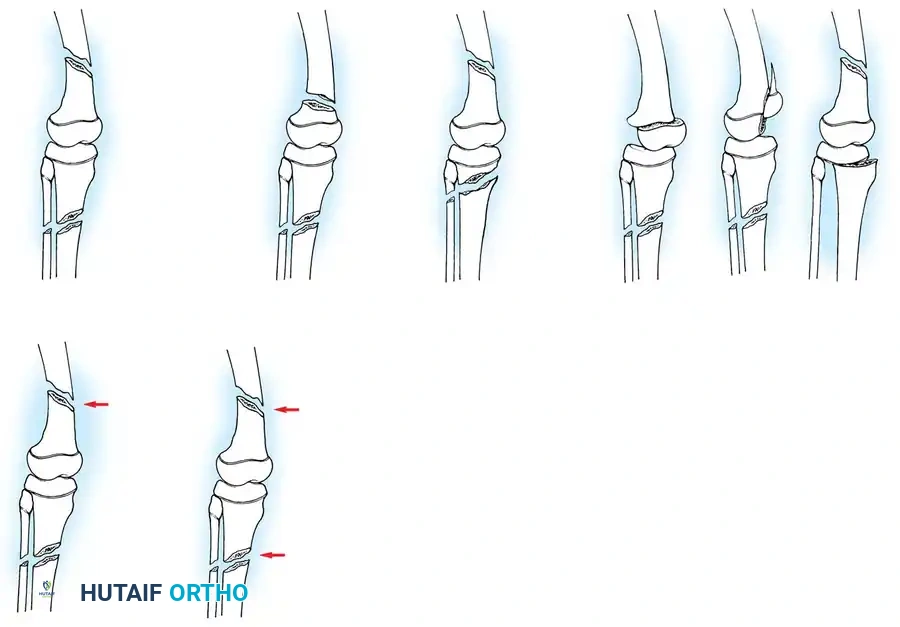
Fig. 33-171: Classification of floating knee injuries in children. (Redrawn from Letts M, Vincent N, Gouw G: The “floating knee” in children, J Bone Joint Surg 68B:442, 1986.)
Floating Knee Injuries in Children
The "floating knee" describes an ipsilateral fracture of the femur and tibia, creating a flail knee joint. These are high-energy injuries often associated with polytrauma. The Letts classification (Types A through E) categorizes these based on whether the fractures are open or closed, and whether they involve the diaphysis or the metaphysis/epiphysis.

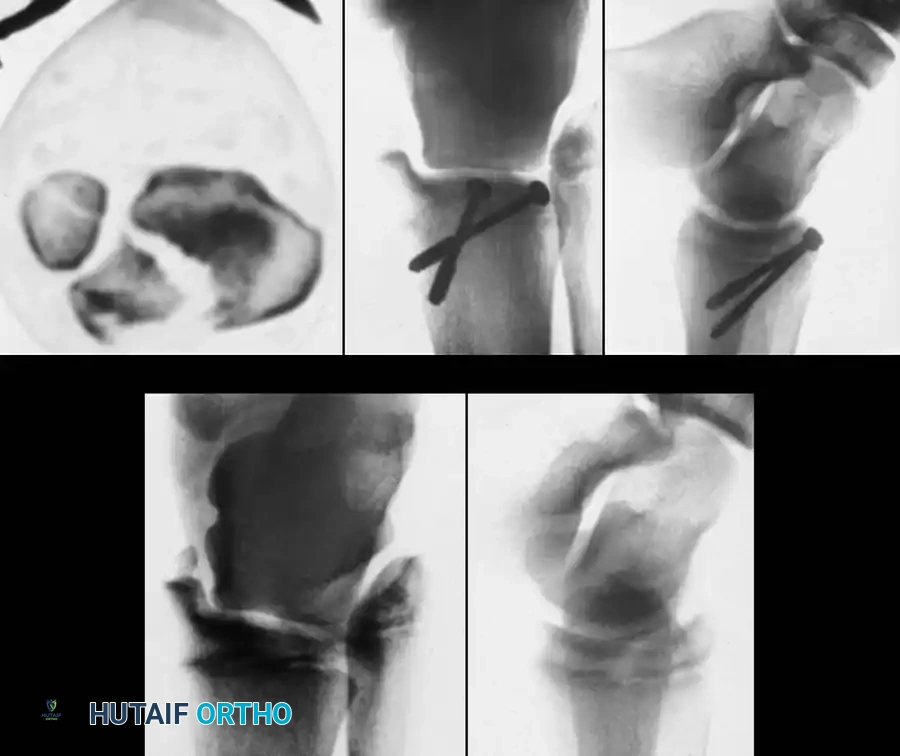
Fig. 33-172: A and B, Severe floating knee injury with midshaft fracture of femur, Salter-Harris type I fracture of distal femoral physis, and comminuted fracture of tibial shaft. C, After internal fixation of distal femoral physeal fracture with crossed pins and external fixation of fractures of femoral and tibial shafts.
The Bohn and Durbin classification system, modified by Arslan et al., further delineates these complex patterns:
* Type I: Double shaft fracture.
* Type II: One juxtaarticular fracture.
* Type IIIa: One epiphyseal fracture, one metaphyseal or diaphyseal fracture.
* Type IIIb: Both epiphyseal fractures (distal femur, proximal tibia).
* Type IV: Femur and/or tibia fracture at two distinct sites.
TIBIAL AND FIBULAR FRACTURES
Pediatric fractures of the tibia and fibula generally possess an excellent capacity for remodeling and can predominantly be treated via closed reduction and cast immobilization. Operative intervention is strictly indicated when fractures are irreducible, open, associated with compartment syndrome, or involve the proximal or distal tibial physes with unacceptable displacement.
Clinical Pearl: An incomplete metaphyseal fracture of the proximal tibia (often termed a "coaxing" or "trampoline" fracture) is highly worrisome. Even when minimally displaced, it carries a notorious reputation for developing a progressive valgus deformity (Cozen's phenomenon) during the healing phase.
Proximal Tibial Physeal Fractures
Fractures of the proximal tibial epiphysis demand heightened vigilance due to their intimate anatomical relationship with the popliteal artery.
In 1965, Aitken made two seminal observations regarding these injuries:
1. Ligamentous Anatomy: Fewer ligaments attach directly to the proximal tibial physis compared to the distal femoral physis. The medial collateral ligament (MCL) inserts distally onto the tibial metaphysis, bypassing the physis. Consequently, the distal femoral physis separates far more frequently than the proximal tibial physis (a ratio of approximately 8:1 in major trauma centers).
2. Vascular Proximity: The popliteal artery is firmly tethered posteriorly by the fibrous arch of the soleus muscle. When the proximal tibial shaft is displaced posteriorly in Salter-Harris Type I and II fractures, the artery is stretched over the sharp metaphyseal ridge, leading to intimal tearing, thrombosis, or complete transection.
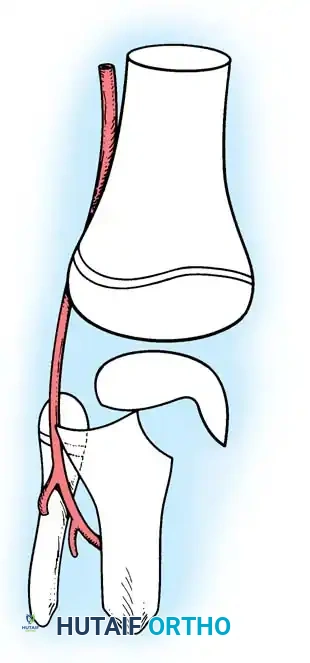
Fig. 33-173: Salter-Harris type I and II fractures with posterior displacement of the tibial shaft may severely injure the popliteal artery.
Wozasek et al. reported that 13% of patients with proximal tibial physeal injuries exhibited peripheral ischemia. Immediate vascular assessment (Ankle-Brachial Index, Doppler ultrasound, or CT angiography) is mandatory for any displaced proximal tibial fracture.
Salter-Harris Classifications and Variants
Canale and Shelton's extensive review of proximal tibial epiphyseal fractures highlighted that these injuries typically occur in older children (average age 14.2 years) approaching skeletal maturity.
- Type I and II Fractures: Most can be managed with closed reduction and a bent-knee cast. However, posterior displacement requires meticulous reduction to relieve arterial tension. Unacceptable angulation must be corrected; malunion in older children will not remodel sufficiently.
- Type III Fractures: These present in two distinct patterns:
- An intra-articular fracture analogous to an adult tibial plateau fracture.
- A fracture propagating through the tibial tuberosity physis, extending proximally across the epiphysis and into the knee joint.
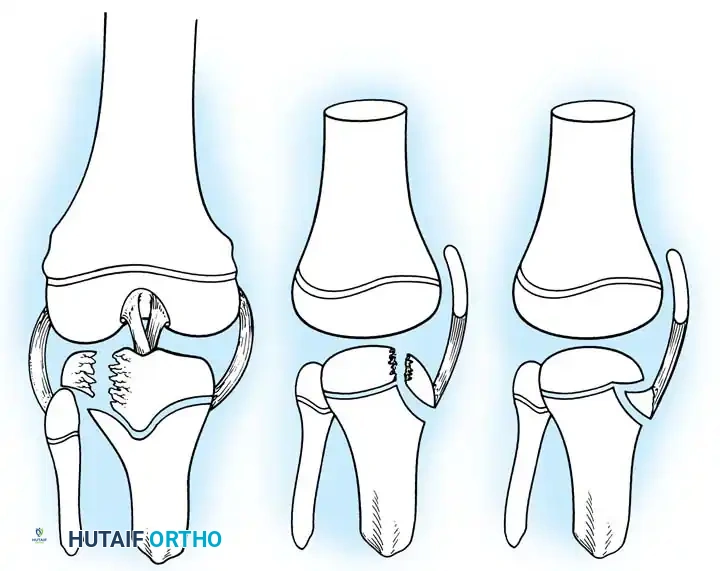
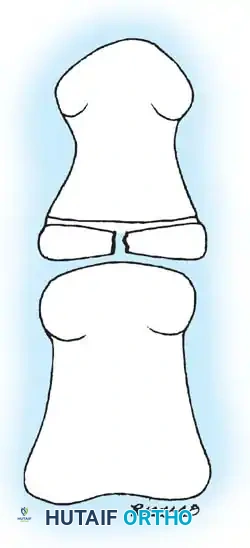
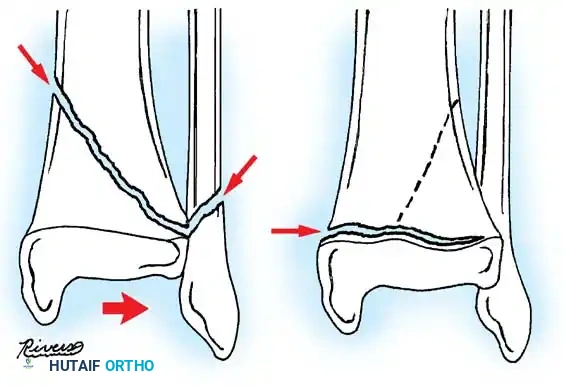
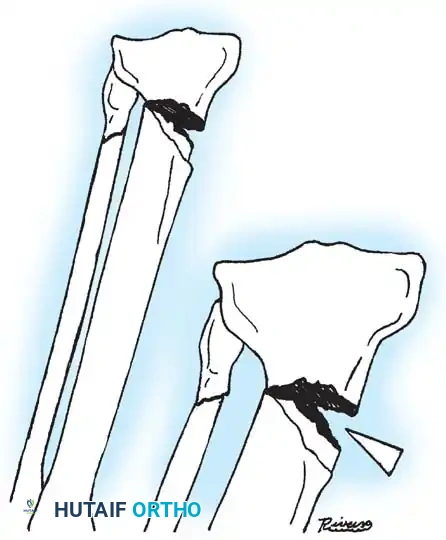
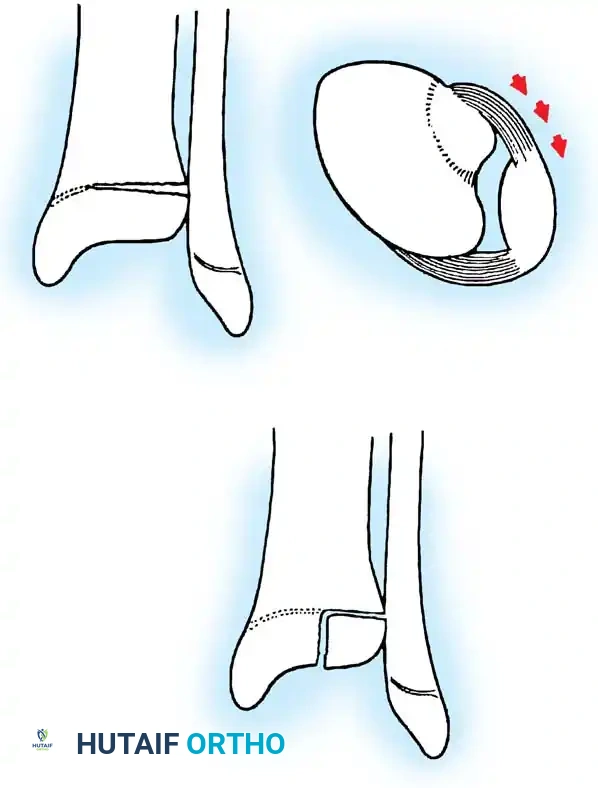
Fig. 33-174: Salter-Harris type III fracture of the proximal tibia. A, Fracture analogous to a tibial plateau fracture. B, Fracture through the tibial tuberosity and across the epiphysis into the knee joint.
These tuberosity-extending fractures are not simple avulsions; they are massive, tongue-type Salter-Harris III injuries that lift the entire tibial tuberosity and anterior proximal physis superiorly. They almost universally necessitate open reduction and internal fixation (ORIF) to restore joint congruity and extensor mechanism continuity.

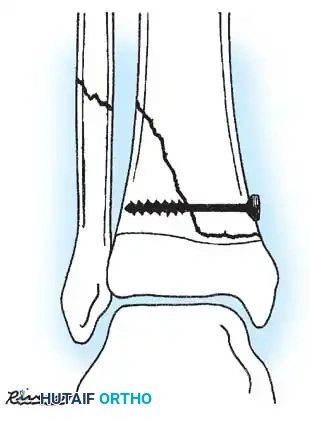
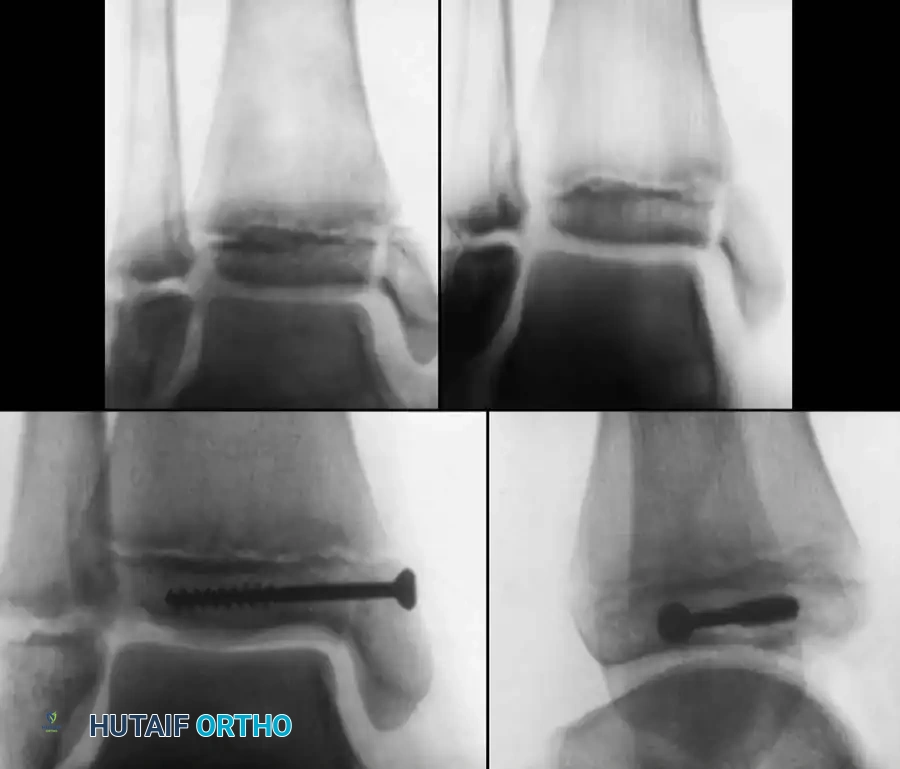
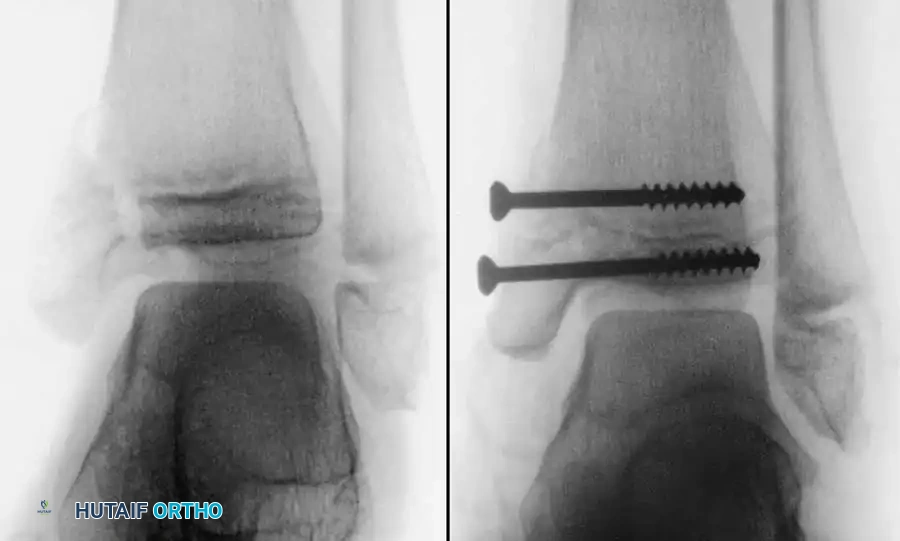
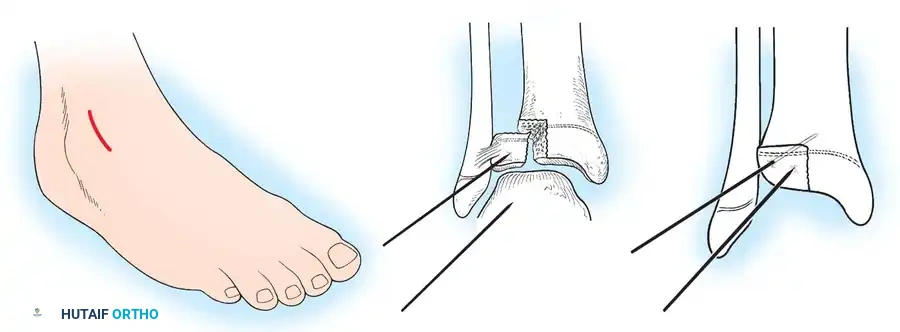
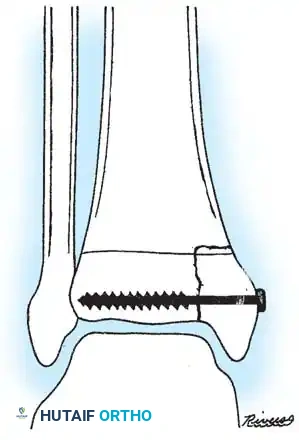
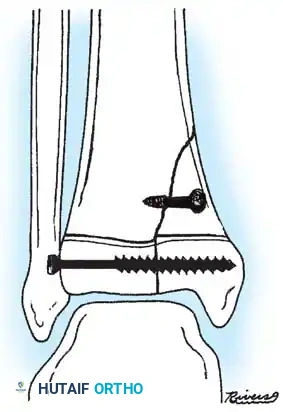
Fig. 33-175: Fixation of a tongue-type Salter-Harris III fracture utilizing cancellous screws.
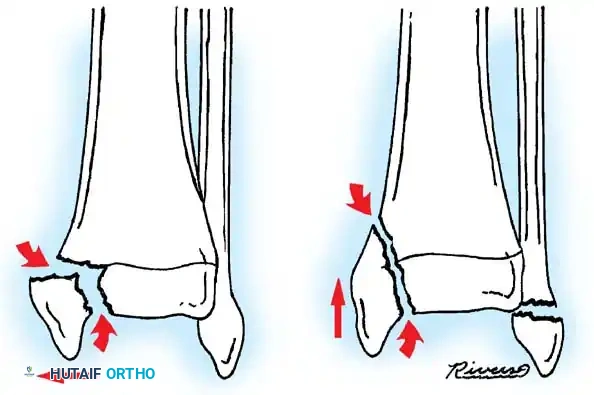
- Type IV Fractures: These cross both the epiphysis and metaphysis. They carry a high risk of growth arrest and joint incongruity. Stress radiographs are invaluable for diagnosing associated ligamentous instability, which may masquerade as a simple non-displaced physeal fracture.

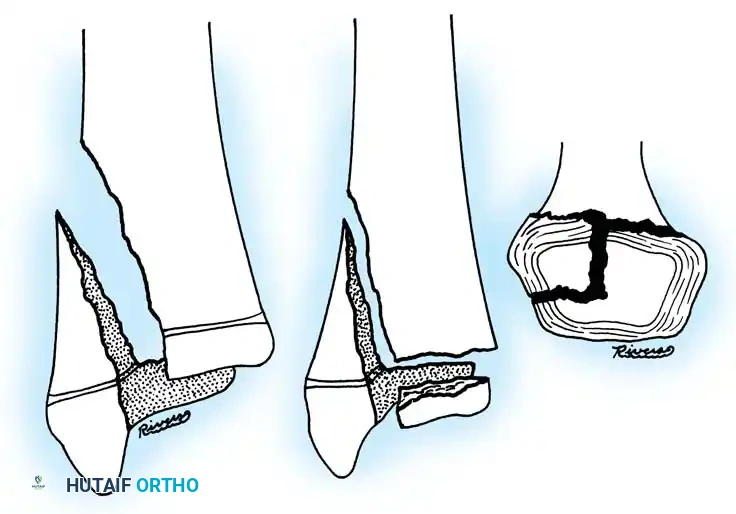
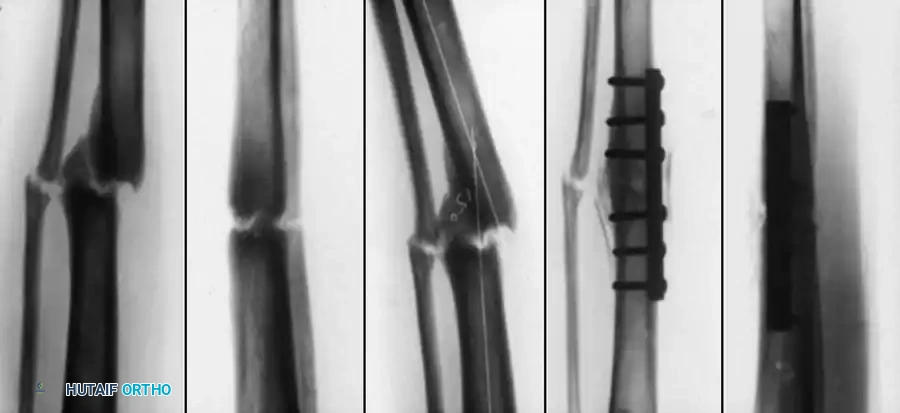
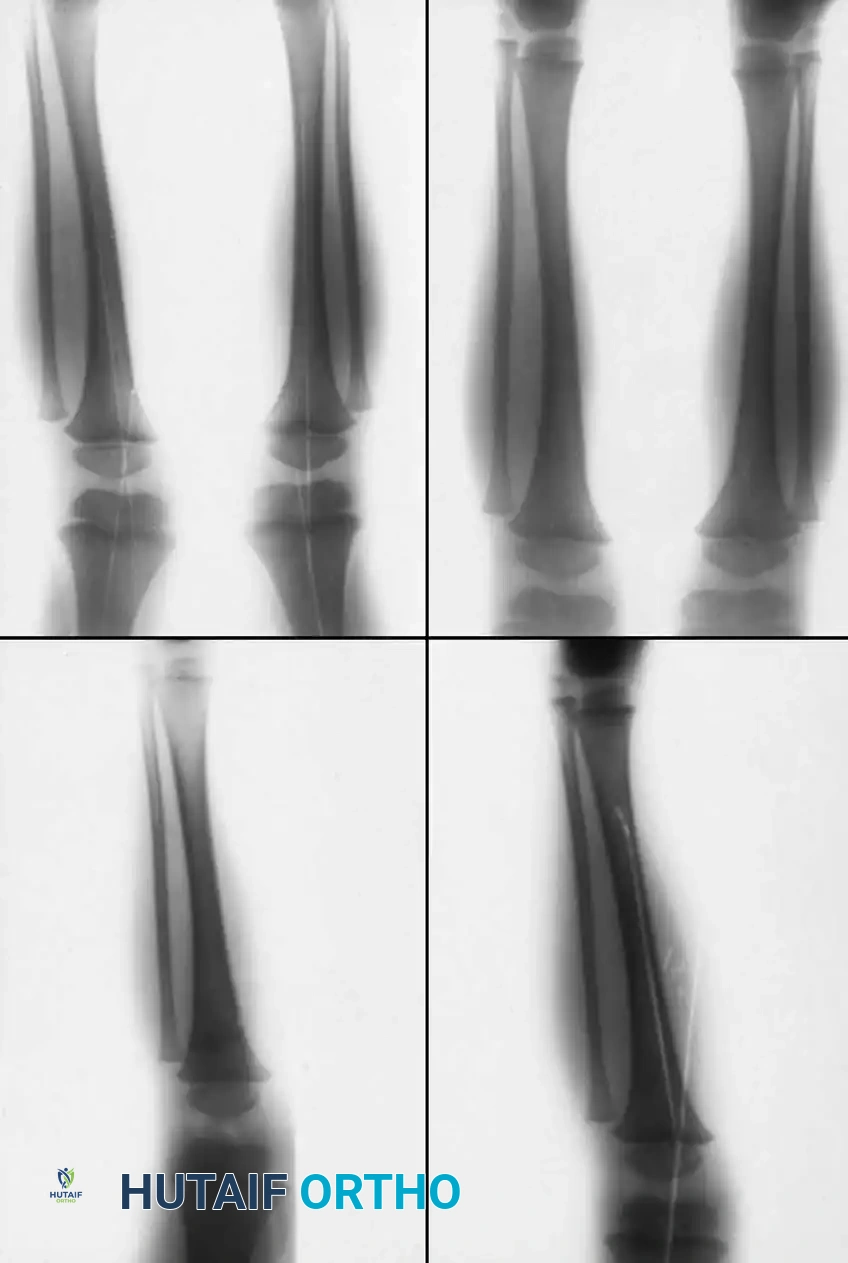
Fig. 33-176: Physeal fracture with major ligamentous injury. A, Nondisplaced Salter-Harris type IV fracture. B, Stress radiograph shows fracture displacement and medial joint line opening, implying tibial collateral ligament injury. C, Intraoperative view during ORIF.
Triplane Variants: Variants of Salter-Harris III and IV fractures have been described as "triplane fractures of the proximal tibial epiphysis," analogous to the more common distal tibial triplane fractures. These occur during the transitional phase of physeal closure. If displaced, they require precise ORIF.
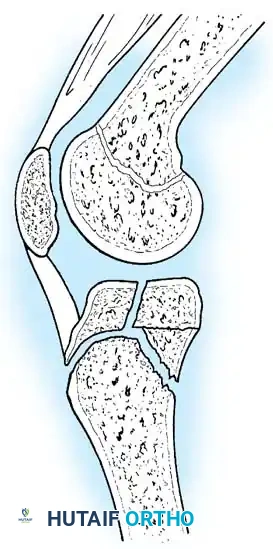
Fig. 33-177: Sagittal view of the knee depicting a coronal split fracture of the proximal tibia epiphysis through a partially closed physis.
Advanced imaging (CT with sagittal and coronal reconstructions, or MRI) is critical to determine the exact fracture geometry and the degree of articular step-off. Plain radiographs often underestimate the severity of the displacement, providing a false sense of security.
SURGICAL TECHNIQUE: ORIF OF TIBIAL TUBEROSITY / PHYSEAL FRACTURES
When displacement dictates surgical intervention, meticulous handling of the soft tissues and anatomic restoration of the articular surface are paramount.
Surgical Warning: The anterior tibial recurrent artery and the anterior compartment musculature are in close proximity. Avoid excessive lateral dissection to prevent devascularization of the fragment or iatrogenic compartment syndrome.
Technique 33-44: Open Reduction and Internal Fixation
1. Preparation and Positioning:
* Place the patient supine on a radiolucent table.
* Apply a high thigh tourniquet. Exsanguinate the limb and inflate the tourniquet.
* Prepare and drape the limb to allow full flexion and extension of the knee.
2. Surgical Approach:
* Make a longitudinal medial or lateral parapatellar incision, dictated by the primary location of the fracture line.
* Carry the dissection through the subcutaneous tissues down to the fracture site. Expose the fracture widely, but preserve the periosteal attachments to the anterior fragment to maintain vascularity.
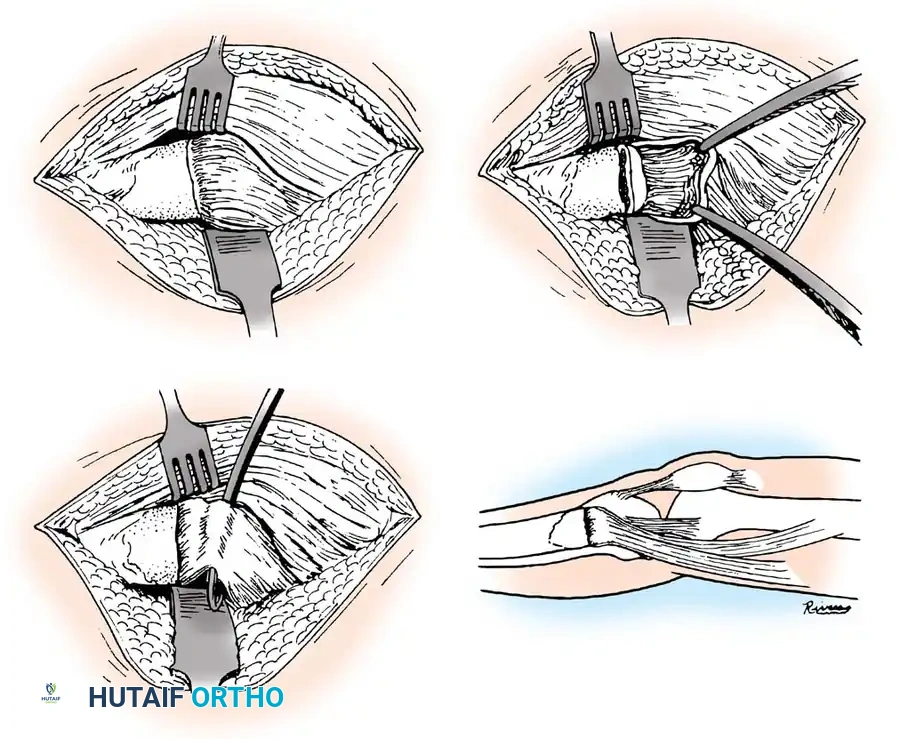
Intraoperative exposure demonstrating the parapatellar approach.
Elevation of the soft tissues to visualize the fracture hematoma.
3. Debridement and Joint Inspection:
* The Salter-Harris III or IV injury is frequently a tongue-type fracture anteriorly, with the entire tibial tuberosity elevated and hinged posteriorly.
* Dissect medially and laterally into the joint capsule until the intra-articular physeal fracture line is visualized.
* Elevate the entire physeal fragment gently. Irrigate the joint copiously to remove hematoma and osteochondral debris.
* Critically, extract any interposed soft tissues (such as torn periosteum or the anterior horn of the meniscus) from the fracture site, as these will mechanically block reduction.
Removal of interposed periosteum from the fracture site.
Direct visualization of the articular surface to ensure anatomic reduction.
4. Reduction:
* Reduce the fracture anatomically. The motion should mimic closing a book or a hinge.
* Extend the knee; if the reduction springs open or feels elastic, soft tissue entrapment is still present and must be addressed.
* Confirm joint congruity visually and via fluoroscopy.
Fluoroscopic confirmation of anatomic reduction prior to definitive fixation.
5. Fixation:
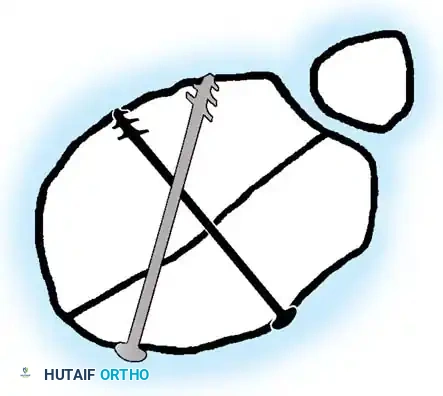
* For vertical fracture components, insert transverse guide pins.
* In older children and adolescents nearing skeletal maturity, utilize 4.0mm or 4.5mm partially threaded cancellous bone screws to achieve interfragmentary compression.
* In younger children with significant remaining growth potential, utilize smooth Kirschner wires (K-wires) placed transversely or horizontally to minimize the risk of physeal arrest.
Placement of transverse fixation pins.
Final construct utilizing cancellous screws for rigid fixation.
6. Closure:
* Deflate the tourniquet and achieve meticulous hemostasis.
* Irrigate the wound copiously.
* Repair the retinaculum and close the subcutaneous tissues and skin in layers.
Postoperative Protocol:
Apply a well-padded, long-leg bent-knee cast (flexed to 30-40 degrees to relax the extensor mechanism). The cast remains in place for 4 to 6 weeks. At 2 weeks, a window is made for suture removal and wound inspection. Gentle, progressive mobilization of the knee is initiated between 4 and 6 weeks, tailored to the child's age and radiographic evidence of healing.
PROXIMAL TIBIAL METAPHYSEAL FRACTURES AND VALGUS DEFORMITY
Displaced fractures of the proximal tibial metaphysis carry a risk of posterior tibial artery injury. However, even non-displaced or minimally displaced metaphyseal fractures are notorious for a delayed complication: progressive valgus angular deformity, commonly known as Cozen's phenomenon.
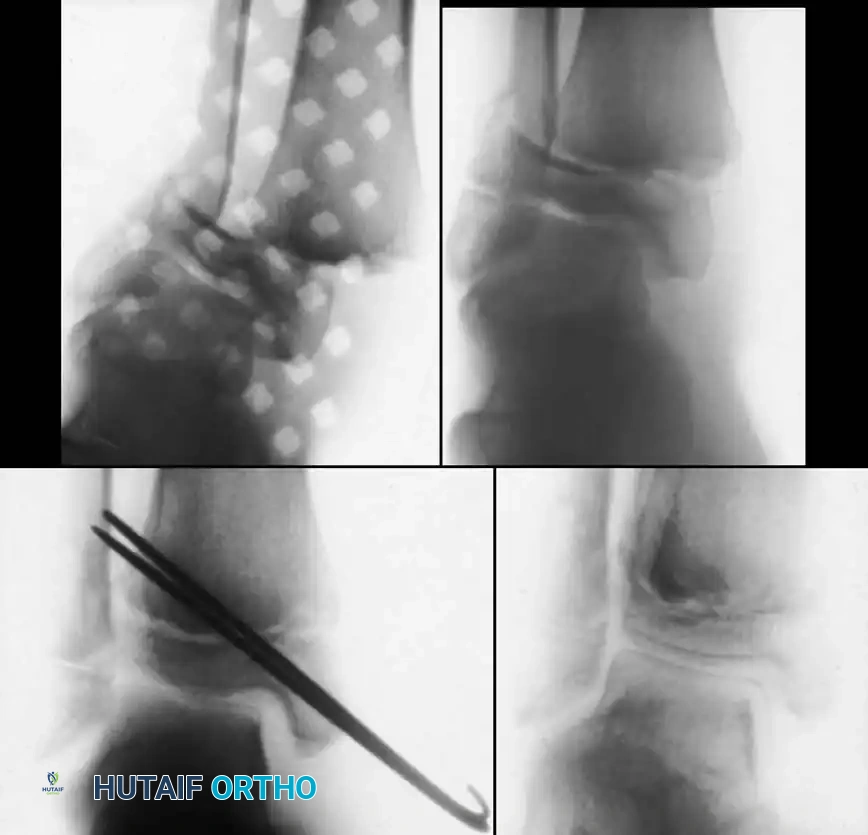
Associated Surgical & Radiographic Imaging




You Might Also Like