Wrist Denervation
Introduction & Epidemiology
Arthrosis of the wrist often presents with functional movement but with substantial disability due to pain. The purpose of wrist denervation is to decrease pain by surgically dividing the nerves that transmit the afferent pain signal from the wrist. Wrist denervation represents a valuable pain-modulating procedure within the armamentarium of reconstructive and salvage options for chronic wrist pain. It is particularly indicated in cases of diffuse or localized wrist arthrosis where joint-preserving procedures are either deemed insufficient, contraindicated, or have failed, and where maintaining some degree of wrist motion is prioritized over complete arthrodesis.
Epidemiologically, wrist arthrosis is a significant source of musculoskeletal morbidity, with common etiologies including scaphoid nonunion advanced collapse (SNAC), scapholunate advanced collapse (SLAC), degenerative changes secondary to crystalline arthropathy, inflammatory arthritis, and post-traumatic conditions. While the mechanical progression of these pathologies can lead to gross instability or stiffness, a considerable proportion of patients experience persistent, debilitating pain despite relatively preserved wrist kinematics. In these scenarios, denervation offers a pathway to pain relief without altering the underlying joint mechanics or necessarily limiting future, more definitive surgical interventions. The concept of wrist denervation emerged from early observations of the rich sensory innervation of the wrist capsule and the potential to interrupt these pain pathways while preserving motor function. Its utility lies in addressing the nociceptive component of arthritic pain.
Surgical Anatomy & Biomechanics
The wrist joint is complex, with a highly intricate sensory innervation pattern derived from branches of the radial, ulnar, and median nerves. A comprehensive understanding of this neuroanatomy is paramount for effective denervation, ensuring adequate pain relief while minimizing unintended sensory deficits or motor sequelae.
The primary nerves involved in wrist joint innervation include:
-
Posterior Interosseous Nerve (PIN):
Considered the most consistently important nerve innervating the dorsal wrist capsule. The PIN is a terminal motor branch of the radial nerve, originating at the elbow, piercing the supinator muscle (arcade of Frohse), and then descending along the posterior interosseous membrane. Distal to the extensor retinaculum, it loses its motor fascicles and terminates as a purely sensory nerve, providing extensive innervation to the dorsal radiocarpal and intercarpal joint capsules. Multiple fine branches are typically found supplying the scaphoid, lunate, triquetrum, and the interosseous ligaments. Its resection is a cornerstone of dorsal wrist denervation.

- Anterior Interosseous Nerve (AIN): The AIN is a terminal motor branch of the median nerve, originating in the forearm. It descends along the interosseous membrane, supplying deep forearm flexors. Distally, it terminates as a sensory nerve, providing innervation to the palmar radiocarpal and midcarpal joint capsules, particularly the palmar ligaments and the lunate. It is typically found deep to the pronator quadratus muscle.
-
Radial Nerve:
-
Dorsal Sensory Branch of the Radial Nerve (DSRN):
Proximally, it emerges from beneath the brachioradialis tendon and divides into multiple branches supplying the dorsum of the hand and fingers. Specific articular branches contribute significantly to the innervation of the radial aspect of the dorsal wrist capsule, particularly around the scaphoid and trapezium. These branches are often targeted during radial-sided denervation.

-
Dorsal Sensory Branch of the Radial Nerve (DSRN):
Proximally, it emerges from beneath the brachioradialis tendon and divides into multiple branches supplying the dorsum of the hand and fingers. Specific articular branches contribute significantly to the innervation of the radial aspect of the dorsal wrist capsule, particularly around the scaphoid and trapezium. These branches are often targeted during radial-sided denervation.
-
Ulnar Nerve:
- Dorsal Cutaneous Branch of the Ulnar Nerve (DCUN): This branch typically arises 5-8 cm proximal to the wrist crease, courses dorsally around the ulnar head, and divides into branches supplying the ulnar aspect of the dorsum of the hand and fingers. Articular branches from the DCUN contribute to the innervation of the ulnar aspect of the dorsal wrist capsule, including the triquetrum and hamate.
- Deep Branch of the Ulnar Nerve: While primarily motor, it may send small articular branches to the ulnar palmar wrist capsule.
-
Median Nerve:
- Palmar Cutaneous Branch of the Median Nerve (PCMN): This branch arises from the median nerve proximally and travels superficially to the transverse carpal ligament. It provides sensory innervation to the thenar eminence and the central palmar wrist capsule.
- Recurrent Intermetacarpal Nerve Branches: These are smaller, often variable branches that can arise from the dorsal sensory radial, dorsal cutaneous ulnar, or even proper digital nerves, contributing to dorsal and intercarpal joint capsule innervation. Their consistent identification can be challenging.
Capsular Innervation Patterns:
The innervation of the wrist capsule is not uniformly distributed. The dorsal capsule, particularly the radiocarpal and midcarpal joints, receives dense innervation predominantly from the PIN and branches of the DSRN and DCUN. The palmar capsule receives innervation primarily from the AIN and branches of the PCMN. Pain signals from specific areas of arthrosis often correlate with the distribution of these nerves. For instance, radioscaphoid arthrosis frequently implicates PIN and DSRN branches, while midcarpal pain can involve branches from both PIN and AIN.
Biomechanics:
It is crucial to understand that wrist denervation is a palliative procedure focused on pain modulation. It does
not
address or alter the underlying pathomechanics of the wrist joint. Arthrosis results in cartilage degradation, altered joint congruence, and abnormal force transmission, leading to inflammatory and mechanical pain. Denervation interrupts the afferent nociceptive pathways, thereby reducing the perception of pain. The range of motion, stability, and load-bearing capacity of the wrist remain unchanged by denervation. Therefore, patients with significant mechanical instability, gross degenerative changes leading to severe crepitus, or impending ankylosis may derive limited benefit from denervation alone. Its role is often to defer or avoid more invasive reconstructive procedures such as partial or total wrist arthrodesis, or proximal row carpectomy, particularly in patients with reasonable range of motion and an absence of overt mechanical blockages.
Indications & Contraindications
The judicious selection of patients for wrist denervation is critical for achieving favorable outcomes. This procedure is generally considered for patients experiencing chronic, debilitating wrist pain primarily attributable to arthrosis, where conservative measures have failed, and where preservation of motion is a priority.
Indications for Operative Denervation
- Chronic wrist pain refractory to conservative management: This includes patients who have failed non-steroidal anti-inflammatory drugs (NSAIDs), activity modification, splinting, physical therapy, and corticosteroid injections.
-
Established wrist arthrosis:
Common causative conditions include:
- Scaphoid Nonunion Advanced Collapse (SNAC)
- Scapholunate Advanced Collapse (SLAC)
- Kienbock's disease (late stages with associated arthrosis)
- Post-traumatic arthrosis (e.g., following distal radius fracture, carpal fractures)
- Degeneration secondary to inflammatory arthritis (e.g., rheumatoid arthritis, psoriatic arthritis) or crystalline arthropathy.
- Preserved, functional wrist motion: While not strictly defined, patients should ideally have a useful range of motion without significant mechanical block or stiffness, allowing for a reasonable functional baseline post-denervation.
- Absence of significant mechanical instability: While denervation can be performed in the presence of mild instability, it is not a stabilizing procedure. Gross instability requiring surgical stabilization is generally a contraindication to isolated denervation.
- Patient unsuitability or unwillingness for more extensive reconstructive surgery: This includes patients with significant medical comorbidities, advanced age, or those who wish to avoid more definitive procedures like arthrodesis or arthroplasty, or who seek a less invasive, motion-preserving option.
- Positive diagnostic nerve blocks: A temporary, significant reduction in pain following selective injection of a local anesthetic around the target nerves (e.g., PIN, AIN) is a strong predictor of a successful denervation outcome. This is a critical diagnostic step.
Contraindications
- Gross wrist instability or mechanical incongruity requiring stabilization: Denervation does not provide mechanical stability.
- Severely stiff or ankylosed wrist joint: Pain in these cases is often less responsive to denervation, as the primary issue is mechanical limitation rather than nociceptive input from a moving, arthritic joint.
- Active infection within the wrist or surrounding tissues.
- Complex Regional Pain Syndrome (CRPS): Denervation can sometimes exacerbate CRPS symptoms or be ineffective due to the systemic and central sensitization components of CRPS.
- Unrealistic patient expectations: Patients must understand that denervation aims to reduce pain, not eliminate it entirely, and does not restore joint mechanics or prevent further arthrosis progression.
- Pure neuropathic pain: If the primary pain source is definitively neuropathic (e.g., nerve compression, established neuroma) rather than nociceptive from the arthritic joint, denervation of joint sensory nerves is unlikely to be effective.
- Lack of response to diagnostic nerve blocks: A failed diagnostic block significantly decreases the likelihood of surgical success.
Summary of Indications
| Feature | Operative Denervation Indications | Non-Operative Management Indications (Initial or Primary) |
|---|---|---|
| Pain | Chronic, debilitating, localized wrist pain | Acute or intermittent wrist pain; mild-to-moderate pain; diffuse, non-arthritic pain |
| Pathology | Established wrist arthrosis (SLAC, SNAC, post-traumatic, etc.) | Early arthrosis; tendinitis; tenosynovitis; ligament sprains without established collapse |
| Conservative Tx | Failed comprehensive conservative management (≥6 months) | Initial presentation; prior to exhausting non-surgical options |
| Wrist Motion | Preserved functional range of motion | Normal or near-normal range of motion; mild stiffness responsive to therapy |
| Stability | Stable or mildly unstable wrist (no gross mechanical instability) | Stable wrist; no carpal collapse |
| Diagnosis | Positive diagnostic nerve blocks; clear source of nociceptive pain | Diagnosis unclear; negative nerve blocks; neuropathic pain components |
| Patient Factors | Willingness to undergo surgery; comorbidities precluding larger procedures | Preference for non-surgical; high surgical risk; unrealistic expectations for surgery |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential to optimize the outcomes of wrist denervation. This includes accurate diagnosis, realistic patient counseling, and meticulous surgical preparation.
Diagnostic Workup
-
History and Physical Examination:
- Detailed pain history: location, character, exacerbating/alleviating factors, duration, intensity.
- Functional limitations: activities of daily living, occupational impact, recreational activities.
- Prior treatments and their efficacy.
- Physical examination: visual inspection for swelling/deformity, palpation for tenderness (e.g., specific carpal bones, joint lines), assessment of active and passive range of motion, strength testing, and neurovascular status. Special maneuvers may help localize pain (e.g., radial/ulnar deviation with load, grind tests).
-
Imaging:
- Plain Radiographs: Standard posteroanterior (PA), lateral, and oblique views of the wrist are mandatory. Additional views such as clenched-fist PA and radial/ulnar deviation views can assess carpal alignment and instability patterns (e.g., SLAC, SNAC progression).
- MRI: Useful for assessing cartilage integrity, occult fractures, ligamentous injury, inflammatory changes, and soft tissue pathologies. It can help confirm the extent of arthrosis.
- CT Scan: Provides excellent bony detail, crucial for evaluating carpal nonunions, fracture morphology, and the extent of degenerative changes, particularly in complex articulations.
-
Diagnostic Nerve Blocks:
This is the most critical pre-operative diagnostic tool.
- Targeted Blocks: Selective blocks of the posterior interosseous nerve (PIN), anterior interosseous nerve (AIN), dorsal sensory radial nerve branches, and dorsal cutaneous ulnar nerve branches are performed under image guidance (ultrasound or fluoroscopy) with local anesthetic.
-
Interpretation:
A reproducible, significant (e.g., >50%) reduction in pain for the duration of the anesthetic's action strongly indicates that the targeted nerve bundle is a primary source of nociception and predicts a favorable surgical outcome. Multiple blocks may be required to precisely delineate the pain source.

Patient Counseling
- Realistic Expectations: It is crucial to inform patients that denervation aims to reduce pain, not necessarily eliminate it. The procedure does not alter the underlying pathology or prevent disease progression.
- Potential for Numbness/Dysesthesia: Patients must be aware of the possibility of sensory changes, particularly when superficial sensory branches are resected. While typically minor, persistent numbness or dysesthesia can occur.
- Recovery Timeline: Discuss the expected post-operative course, including immobilization, rehabilitation, and time to return to activities.
- Salvage Options: Explain that denervation does not preclude future, more definitive procedures (e.g., arthrodesis, arthroplasty) if pain recurs or progresses.
Anesthesia and Patient Positioning
- Anesthesia: The procedure can be performed under regional anesthesia (e.g., axillary or interscalene block) with sedation, or general anesthesia. Regional anesthesia offers excellent post-operative pain control.
- Tourniquet: A pneumatic tourniquet on the upper arm is routinely used to provide a bloodless surgical field, which is essential for meticulous nerve identification and dissection.
-
Positioning:
The patient is typically positioned supine on the operating table. The affected arm is abducted and placed on a specialized hand table. For dorsal approaches, the forearm is pronated. For palmar approaches, the forearm is supinated. Secure padding of pressure points is imperative.
Instrumentation
- Standard hand surgery tray.
- Magnification: Loupe magnification (2.5x to 4.5x) is considered essential for precise identification and dissection of small nerve branches, reducing the risk of damaging adjacent structures. Operating microscope may be used in selected cases.
- Fine-tipped bipolar cautery.
- Micro-nerve hooks and scissors.
- Marking pen.
Detailed Surgical Approach / Technique
The goal of wrist denervation is to surgically interrupt the sensory innervation to the wrist joint capsule. This typically involves the resection of specific nerve branches that transmit nociceptive signals. The extent of denervation can range from selective targeting of individual nerves to a more comprehensive four-corner denervation.
General Principles of Denervation
- Direct Visualization and Magnification: All targeted nerves must be directly visualized under adequate magnification (loupes at minimum).
- Segmental Resection: A segment of each nerve branch (typically 1-2 cm) is resected to minimize the potential for reinnervation and painful neuroma formation.
- Burying Nerve Endings: Whenever possible, the cut nerve stumps should be buried into adjacent muscle tissue, bone, or fascia to further reduce the risk of neuroma formation.
- Hemostasis: Meticulous hemostasis is crucial throughout the procedure, facilitated by a pneumatic tourniquet.
Specific Surgical Approaches
The choice of approach depends on the targeted nerves and the surgeon's preference. A "complete" or "four-corner" denervation typically involves addressing the PIN, AIN, and articular branches of the dorsal sensory radial and dorsal cutaneous ulnar nerves.
1. Dorsal Approach for PIN and Dorsal Sensory Radial/Ulnar Branches
This is the most common approach as the dorsal capsule receives dense innervation.
-
Incision:
A longitudinal skin incision, approximately 6-8 cm in length, centered over Lister's tubercle. It can be slightly curvilinear, following Langer's lines, but must provide adequate access to the extensor compartments. Alternatively, two separate incisions (radial and ulnar) can be used.

-
Dissection:
- The incision is deepened through the subcutaneous tissue. Care is taken to identify and protect the branches of the dorsal sensory radial nerve and dorsal cutaneous ulnar nerve, which often course superficially in this plane. While articular branches are targeted, preserving the main cutaneous distribution is ideal if possible.
-
Posterior Interosseous Nerve (PIN):
- The interval between the third (extensor pollicis longus, EPL) and fourth (extensor digitorum communis, EDC) dorsal extensor compartments is identified. The EPL tendon is retracted radially, and the EDC tendons ulnarly.
- The floor of the fourth compartment, which is the distal part of the posterior interosseous membrane and the dorsal aspect of the wrist capsule, is exposed.
- The PIN is identified as it emerges from beneath the extensor indicis proprius (EIP) muscle and travels on the posterior interosseous membrane. It is typically a very thin, filamentous nerve at this point.
- Multiple fine branches of the PIN are seen ramifying over the dorsal radiocarpal and midcarpal joint capsules. These branches are meticulously identified, individually grasped with a nerve hook, and a 1-2 cm segment is resected. The proximal and distal stumps are cauterized and allowed to retract into soft tissue.
- A more radical approach, sometimes called "Volkmann's denervation" or "dorsal capsular stripping," involves elevating the dorsal capsule from the carpal bones to resect the nerve branches more proximally, though this is less commonly performed than direct nerve resection.
-
Dorsal Sensory Radial Nerve (DSRN) Branches:
- After addressing the PIN, attention is turned radially. Branches of the DSRN that supply the radial wrist capsule are identified. These are typically located distal to the radial styloid and can be found by carefully dissecting in the subcutaneous plane and then deeper towards the joint capsule on the radial side. They are distinct from the more superficial cutaneous branches.
- The articular branches are identified and resected segmentally.
-
Dorsal Cutaneous Ulnar Nerve (DCUN) Branches:
- Ulnarly, articular branches from the DCUN are identified. These are found around the ulnar styloid and distal to it, innervating the ulnar aspect of the dorsal capsule. Careful dissection is required to distinguish these from the main cutaneous branches.
- Segmental resection is performed.
-
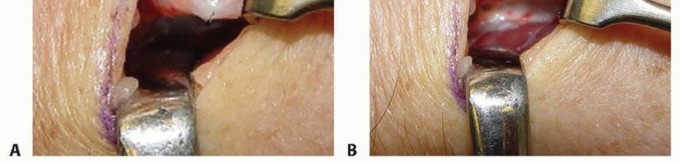
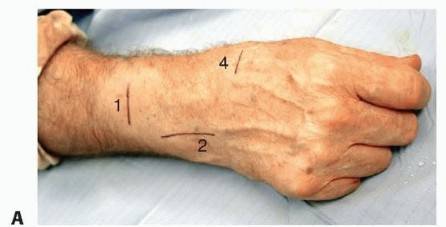
Image Integration:
Here are some images that can be placed in this section to illustrate the dorsal anatomy and technique:



2. Palmar Approach for AIN and Palmar Cutaneous Median Branches
This approach can be performed as a separate procedure or concomitantly with the dorsal approach for a more complete denervation.
- Incision: A longitudinal incision, approximately 4-6 cm, in the distal forearm, between the flexor carpi radialis (FCR) tendon and the median nerve (or palmaris longus tendon if present).
-
Dissection:
- The incision is deepened. The FCR tendon is identified and retracted radially. The median nerve, located ulnar to the FCR, is identified and carefully protected (retracted ulnarly).
-
Anterior Interosseous Nerve (AIN):
- The AIN is found coursing on the anterior interosseous membrane, often deep to the pronator quadratus muscle. It is typically located between the flexor pollicis longus (FPL) tendon radially and the flexor digitorum profundus (FDP) tendons ulnarly.
- The terminal sensory branches of the AIN to the palmar radiocarpal and midcarpal capsules are identified. These can be very fine and require diligent search.
- Segmental resection of 1-2 cm of these branches is performed.
-
Palmar Cutaneous Median Nerve (PCMN) Branches:
- Branches of the PCMN, if targeted, are typically more superficial and supply the central palmar wrist capsule. They arise from the median nerve proximally and course superficial to the transverse carpal ligament.
- Careful dissection is needed to identify these while protecting the main median nerve trunk.
- Segmental resection of articular branches.
-
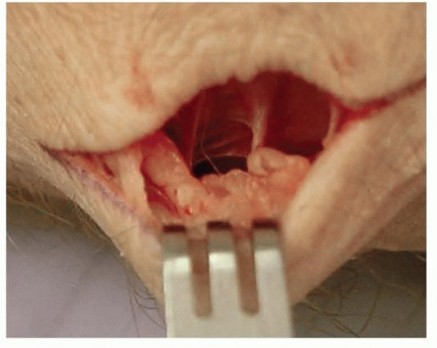
Image Integration:
An image depicting the palmar aspect or AIN identification would be suitable here:
Closure
- After meticulous hemostasis and confirmation of nerve resection, the tourniquet is deflated. Any bleeding points are addressed.
- The wound is closed in layers: subcutaneous tissue with absorbable sutures, and skin with non-absorbable sutures or staples.
-
A sterile dressing and a soft compressive dressing or splint (sugar tong or volar) are applied to immobilize the wrist in a functional position for initial healing.

Intraoperative Considerations
- Microscope vs. Loupes: While loupes are generally sufficient, an operating microscope can provide superior visualization, particularly for identifying the finer terminal branches and ensuring precise resection.
- Cystic Degeneration: In advanced arthrosis, ganglion cysts or synovial hypertrophy may obscure nerve branches; these should be carefully debrided to expose the underlying nerves.
- Variability: Anatomical variations exist, and the surgeon must be prepared to adapt the dissection based on intraoperative findings.
Complications & Management
While generally considered a safe procedure, wrist denervation is not without potential complications. Awareness of these complications and their appropriate management strategies is crucial for patient care.
Table of Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approximate) | Management Strategies |
|---|---|---|
| Persistent/Recurrent Pain | 15-40% (most common) | Initial: Non-opioid analgesics, physical therapy, activity modification. Diagnostic: Repeat diagnostic nerve blocks to identify missed/reinnervated branches. Surgical: Revision denervation (if missed branches are identified or reinnervation suspected); conversion to a definitive salvage procedure (e.g., partial or total wrist arthrodesis, proximal row carpectomy, wrist arthroplasty) if pain remains debilitating. |
| Neuroma Formation | 5-15% (can cause localized, sharp pain) | Initial: Local corticosteroid injection, topical analgesics (e.g., lidocaine patches), desensitization exercises. Surgical: Excision of neuroma with transposition of the nerve stump into a muscle belly or bone tunnel to prevent recurrence; nerve capping techniques. |
| Numbness/Dysesthesia | 10-25% (especially with dorsal sensory nerve resection) | Initial: Reassurance (often improves over time), gabapentin/pregabalin for neuropathic symptoms, topical desensitization. Persistent: Neuroma excision (if associated with a symptomatic neuroma), rarely requires further surgical intervention as symptoms usually diminish or become tolerable. |
| Infection (Superficial/Deep) | <5% | Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, intravenous antibiotics (guided by culture), irrigation, potentially hardware removal if present (rare in denervation). |
| Hematoma | <5% | Small: Observation, compression. Large/Expanding: Surgical drainage and meticulous hemostasis; re-evaluation for bleeding diathesis. |
| Stiffness/Reduced ROM | 5-10% | Initial: Aggressive physical and occupational therapy, dynamic splinting. Persistent: Manipulation under anesthesia, capsular release (rarely needed for isolated denervation unless concomitant procedures performed), though often the stiffness is related to the underlying arthrosis rather than the denervation procedure itself. |
| Progression of Arthrosis | Inevitable over time | Initial: Continue conservative management for arthritic symptoms; modify activity. Surgical: Conversion to a definitive salvage procedure (e.g., arthrodesis, PRC, arthroplasty) when pain becomes intolerable or mechanical function severely compromised. Denervation does not alter disease progression but can delay the need for more invasive procedures. |
| Injury to Adjacent Structures | Rare (tendons, vessels, main nerve trunks) | Tendons: Repair if major tendon involved; consider tenolysis if adhesions cause friction/pain. Vessels: Ligation of small vessels; repair of larger vessels if critical flow compromised. Main Nerve Trunks: Immediate repair (microsurgical), nerve grafting if defect too large for primary repair. Management similar to other iatrogenic nerve injuries. Prognosis variable. |
| Complex Regional Pain Syndrome (CRPS) | <1% | Multimodal approach: Physical therapy, pain management (neuropathic medications, nerve blocks), psychological support. Refer to pain specialist. Early recognition and aggressive treatment are key. |
Management Principles
- Early Recognition: Prompt identification of complications allows for timely and effective intervention.
- Conservative First: Many minor complications, especially sensory changes, can be managed conservatively with reassurance, medication, and therapy.
- Referral: For complex issues like persistent neuropathic pain or CRPS, referral to a pain specialist or neurologist is appropriate.
- Patient Education: Ongoing communication with the patient regarding their symptoms, the natural history of complications, and potential management options is paramount.
- Salvage: It is crucial to remember that denervation is often a palliative procedure. If it fails or pain recurs, definitive salvage procedures remain viable options and should be discussed with the patient.
Post-Operative Rehabilitation Protocols
A structured and progressive post-operative rehabilitation protocol is integral to maximizing the functional outcome after wrist denervation. The primary goals are to manage pain, minimize stiffness, restore functional range of motion, and promote a gradual return to activities. Since denervation does not involve bone fixation or significant soft tissue repair that alters joint mechanics, rehabilitation can often progress more rapidly than after reconstructive wrist surgeries.
Phase I: Initial Protection and Pain Management (Days 0-2 Weeks)
- Immobilization: The wrist is typically immobilized in a removable sugar tong splint or a volar wrist splint, often in slight extension (10-20 degrees) to provide comfort and protect the surgical site. This is typically maintained for 1-2 weeks.
- Pain Management: Oral analgesics (NSAIDs, acetaminophen, short-course opioids if necessary) are prescribed. Regional blocks from surgery usually provide initial relief.
- Edema Control: Elevation of the hand and wrist (above heart level), and regular application of ice packs (over dressings) are encouraged to minimize swelling.
-
Early Motion:
- Finger ROM: Active range of motion exercises for the fingers (flexion and extension) are initiated immediately to prevent stiffness and promote fluid circulation.
- Elbow/Shoulder ROM: Full active range of motion exercises for the elbow and shoulder are encouraged to prevent shoulder-hand syndrome.
- Wound Care: Maintain clean and dry dressings. Suture removal usually occurs at 10-14 days post-op.
Phase II: Early Mobilization and Scar Management (Weeks 2-6)
- Discontinue Immobilization: The splint is typically discontinued at 1-2 weeks, and the patient transitions to active range of motion exercises for the wrist.
-
Wrist ROM:
- Active Range of Motion (AROM): Gentle, pain-free active flexion, extension, radial deviation, and ulnar deviation of the wrist are initiated.
- Passive Range of Motion (PROM): As pain allows, gentle passive stretching can be introduced by a therapist or through self-stretching exercises. The goal is to regain functional wrist motion.
- Scar Management: Once the wound is fully closed, scar massage, silicone gel sheeting, or other scar modulation techniques are initiated to minimize adhesion formation and improve scar pliability.
- Light Strengthening (as tolerated): Very gentle isometric wrist strengthening exercises can be introduced, avoiding resistance that causes pain. Grip strengthening with soft putty or a sponge.
- Activities of Daily Living (ADLs): Encourage use of the hand for light ADLs, respecting pain limits. Avoid heavy lifting or repetitive forceful gripping.
Phase III: Progressive Strengthening and Functional Recovery (Weeks 6-12+)
-
Advanced Strengthening:
- Progressive resistive exercises for wrist flexion, extension, radial/ulnar deviation (e.g., light weights, resistance bands).
- Continued and progressive grip strengthening exercises.
- Forearm pronation/supination strengthening.
- Endurance Training: Repetitive, lower-resistance exercises to build endurance.
- Neuromuscular Re-education: Activities to improve proprioception and coordination of the wrist and hand.
- Functional Activities: Gradually increase the intensity and duration of functional tasks, including work-specific tasks, hobbies, and recreational activities.
-
Return to Activity:
- Light Work: Return to light duty or sedentary work often possible by 6-8 weeks.
- Heavy Manual Labor/Sport: Gradual return to more demanding activities and sports by 12 weeks or beyond, guided by pain levels and functional capacity.
- Patient Education: Reinforce the importance of listening to the body, avoiding activities that cause sharp pain, and understanding that full benefits may not be realized for several months.
Expected Outcomes and Timeframe
- Pain Reduction: Patients should experience a noticeable reduction in pain, often within the first few weeks, with continued improvement over 3-6 months. Complete pain elimination is rare.
- Functional Improvement: Improved ability to perform ADLs and potentially return to desired recreational activities due to decreased pain.
- Range of Motion: Generally, range of motion is preserved or even slightly improved due to the reduction of pain-induced guarding.
- Maximal Benefit: The full extent of pain relief and functional improvement may take up to 6 months to a year. Regular follow-up appointments are crucial to monitor progress and adjust the rehabilitation plan as needed.
Summary of Key Literature / Guidelines
Wrist denervation has evolved over decades, from early empirical approaches to more anatomically precise techniques. The body of literature generally supports its role as a viable, motion-preserving option for selected patients with chronic wrist pain secondary to arthrosis.
Evidence-Based Practice
- Level of Evidence: Much of the literature supporting wrist denervation consists of retrospective case series and observational studies, primarily Level IV evidence. However, consistent positive outcomes across multiple centers lend credibility to its efficacy. High-level prospective, randomized controlled trials comparing denervation to other salvage procedures or sham surgery are scarce due to ethical and practical challenges.
-
Key Findings:
- Pain Reduction: Studies consistently report significant pain reduction (often 50-80%) in the majority of patients undergoing wrist denervation. This pain relief can last for several years.
- Functional Improvement: Patients often demonstrate improved grip strength and functional scores (e.g., DASH, PRWE) post-operatively, correlating with reduced pain.
- Motion Preservation: A key advantage is the preservation of wrist range of motion, which remains comparable to pre-operative levels.
- Salvage Procedure: Denervation does not preclude future, more definitive reconstructive or salvage procedures like arthrodesis or proximal row carpectomy. It is often viewed as an intermediate step to delay these more invasive options.
Historical Context and Key Publications
- Wilhelm (1966): Often credited with popularizing the concept of wrist denervation, focusing on selective resection of sensory branches of the radial and ulnar nerves.
- Dartey and Millesi (1987): Described the technique of complete wrist denervation, targeting the PIN, AIN, and dorsal branches of the radial and ulnar nerves. Their comprehensive anatomical studies laid the groundwork for modern approaches.
- Berger and Rizzo (1998, 2002): Published on the anatomy and clinical outcomes of PIN and AIN denervation, highlighting the consistency of the technique for pain relief in wrist arthrosis.
- Ho PC et al. (2014) and other systematic reviews: Several systematic reviews and meta-analyses have pooled data from various studies, generally concluding that wrist denervation provides effective and durable pain relief with an acceptable complication profile for appropriately selected patients. These reviews emphasize the importance of meticulous surgical technique and patient selection.
Comparison to Other Treatments
- Arthrodesis (Fusion): Offers definitive pain relief and stability but at the cost of complete loss of motion. Denervation is a motion-preserving alternative, particularly for those unwilling to accept fusion.
- Proximal Row Carpectomy (PRC): Preserves some motion and provides good pain relief by removing the proximal carpal row. It requires good articular cartilage on the capitate and distal radius. Denervation is less invasive and has a faster recovery, often considered before PRC in cases of early arthrosis or if PRC is contraindicated.
- Partial Wrist Fusions: Stabilize specific carpal joints, reducing pain while preserving some motion. Examples include four-corner fusion or scapho-trapezio-trapezoid (STT) fusion. Denervation is less invasive and avoids the risks associated with bone healing (nonunion) and hardware.
- Wrist Arthroplasty: Provides motion and pain relief but has specific indications, limited lifespan, and potential for complications (loosening, infection, wear). Denervation is a much simpler procedure and can be performed as a bridge or if arthroplasty is not suitable.
Current Guidelines and Future Directions
Current practice generally advocates for wrist denervation as a reliable intermediate procedure for chronic wrist pain due to arthrosis, especially when conservative treatments fail, and patients prioritize motion preservation over definitive joint alteration.
*
Selective vs. Complete Denervation:
While "complete" denervation (targeting all four primary nerve groups) aims for maximal pain relief, selective denervation guided by diagnostic blocks may be sufficient for localized pain, potentially reducing surgical morbidity.
*
Targeted Denervation:
Ongoing research explores more precise methods of denervation, including cryodenervation or radiofrequency ablation, which are less invasive and may offer comparable results, though long-term data are still emerging.
*
Reinnervation:
The potential for nerve regeneration and reinnervation remains a limitation, contributing to recurrent pain over time. Techniques to minimize this, such as more extensive segmental resection or burying nerve stumps, are continuously refined.
In conclusion, wrist denervation remains an important, technically straightforward, and effective option for addressing chronic nociceptive wrist pain in the context of arthrosis, offering a favorable balance between pain relief and motion preservation. Its success hinges on accurate diagnosis, meticulous surgical technique, and realistic patient expectations.
Clinical & Radiographic Imaging