WRIST ARTHRODESIS AND ARTHROPLASTY: PRINCIPLES AND PARADIGMS
The reconstructive procedures available for an arthritic wrist joint represent a complex biomechanical compromise between motion preservation and absolute stability. The primary surgical options include partial arthrodesis, total wrist arthrodesis, and total wrist arthroplasty. The decision-making matrix for these procedures is heavily influenced by the underlying pathology—most commonly rheumatoid arthritis (RA), primary osteoarthritis (OA), or post-traumatic arthritis (e.g., scapholunate advanced collapse [SLAC] or scaphoid nonunion advanced collapse [SNAC]).
Whether wrist arthrodesis or arthroplasty is the superior choice, particularly in the context of rheumatoid arthritis, remains a subject of academic debate. Each procedure has distinct, evidence-based applications. Retention of wrist motion is highly desirable for activities of daily living (ADLs); however, wrist arthroplasty historically carries a higher percentage of late complications, such as aseptic loosening and subsidence, compared to arthrodesis. Conversely, arthrodesis provides a reliably painless and stable wrist once solid fusion is achieved.
Clinical Pearl: In patients with bilateral incapacitating wrist arthritis, a hybrid approach is often the most functional solution. Arthrodesing one wrist provides a stable pillar (crucial if the patient requires crutches or a walker), while performing an arthroplasty on the contralateral wrist preserves the motion necessary for personal hygiene and fine motor tasks.
Indications and Contraindications
Most orthopedic authors and hand surgeons consider Total Wrist Arthrodesis (TWA) the procedure of choice for:
* Marked flexion deformities of the wrist and fingers.
* Chronic carpal dislocation or severe subluxation.
* Painful wrists associated with multiple extensor tendon ruptures. This is especially critical for ruptures of the extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB), as these muscles are absolute prerequisites for dynamic wrist balance.
* High-demand patients (e.g., manual laborers) requiring absolute stability.
Total Wrist Arthroplasty (TWAp) is generally reserved for low-demand patients, typically older individuals with rheumatoid arthritis or low-demand osteoarthritis, who possess adequate bone stock and intact wrist extensors.
According to Carlson and Simmons, absolute and relative contraindications to total wrist arthroplasty include:
* Chronic, uncorrectable carpal subluxation.
* Poor or severely osteopenic bone stock.
* Prior deep joint infection.
* Impaired motor or neurological function.
* Dependence on a walker, cane, or crutches (which places excessive axial load on the implant).
* Impaired or ruptured wrist extensor tendons.
BIOMECHANICS AND PREOPERATIVE PLANNING
The Position of Fusion
The optimal position in which to fuse the wrist for maximal function is controversial and must be tailored to the individual patient. Recommended positions in the literature include:
* 10 to 30 degrees of dorsiflexion: Historically favored to maximize grip strength.
* Neutral position: Alignment of the axis of the third metacarpal coaxial with the axis of the radius in the lateral radiographic projection. This is increasingly preferred, especially if bilateral wrist fusions are planned, to facilitate perineal care and feeding.
Surgical Warning: Usually, both wrists should not be fused in extension. Fusing both wrists in extension makes it biomechanically impossible for the patient to reach their perineum, severely compromising personal hygiene. If bilateral fusions are mandatory, place the dominant wrist in slight extension (for grip) and the non-dominant wrist in slight flexion (for hygiene).
SURGICAL APPROACH: VOLAR DECOMPRESSION AND SYNOVECTOMY
In many rheumatoid patients, severe volar synovitis, flexor tendon compromise, and median nerve compression necessitate a comprehensive volar approach prior to, or in conjunction with, dorsal reconstructive procedures.
Step-by-Step Volar Technique
- Incision and Fascial Release: Make a longitudinal or slightly zig-zag volar incision, ending about 7.5 cm proximal to the wrist crease. Open the deep fascia proximally and identify the median nerve.
- Nerve Protection: Stay strictly on the ulnar side of the median nerve. Meticulously protect the palmar cutaneous branch (which branches radially proximal to the wrist crease) and the recurrent motor branch of the median nerve.
- Ligament Division: Divide the deep transverse carpal ligament to expose the flexor tendons. Note that its distal border extends further distally into the palm than is usually realized.
- Tenosynovectomy: Beginning proximally and proceeding distally—while keeping constantly in mind the location of the median nerve—dissect the hypertrophic synovium from each flexor tendon. Evaluate all flexor tendons for attritional ruptures and erosions.
- Capsular Inspection and Osteophyte Excision: Inspect the volar capsule and ligaments over the carpal bones. Look for eroded areas caused by prominent osteophytes, particularly on the volar pole of the scaphoid. Remove these osteophytes with a rongeur to prevent future flexor tendon rupture.
- Closure: Close the capsule-ligament layer over the carpal bones to provide a smooth gliding surface for the flexor tendons. Do not close the deep transverse carpal ligament.
- Hemostasis and Splinting: Release the tourniquet, obtain meticulous hemostasis, insert a closed-suction drain, and close the skin. Apply a compression dressing and a volar plaster splint from the proximal forearm to the distal palmar crease.
Postoperative Care: Keep the wrist extended for a minimum of 3 weeks. The postoperative care for this volar stage is identical to that of a dorsal synovectomy, focusing on immediate digital range of motion to prevent flexor tendon adhesions.
TOTAL WRIST ARTHROPLASTY (TWAp): IMPLANT EVOLUTION AND TECHNIQUE
The landscape of wrist arthroplasty has evolved significantly from early silicone spacers to modern, semi-constrained, anatomically designed implants. Adequate muscle balance and correctable wrist contractures are paramount requirements for any implant to be successful.
The Meuli III Prosthesis
Fernandez reported excellent results in 24 of 50 wrists treated for rheumatoid or traumatic arthritis with the Meuli III wrist prosthesis. This implant utilizes a ball-and-socket design. Despite excellent early functional results, aseptic loosening occurred in eight wrists, highlighting the biomechanical challenges of unconstrained designs in the wrist.

Correctly implanted Meuli III wrist prosthesis in a 55-year-old woman with rheumatoid arthritis. Note the reconstruction of carpal height and axial alignment. The prosthesis is firmly fixed in carpal bone stock with no palmar protrusion.
The Biaxial Total Wrist Implant
To address the shortcomings of earlier designs, Beckenbaugh and Linscheid developed the semi-constrained "biaxial" wrist implant. It features a porous coating to improve cementless biological fixation or to enhance the cement-bone interface.
Rettig and Beckenbaugh evaluated the use of the biaxial implant as a salvage procedure for failed total wrist arthroplasties, such as fractured Swanson Silastic implants. Although clinical improvement was achieved, loosening remained a persistent problem, especially in patients with aggressive rheumatoid disease. Takwale et al. found that out of 66 biaxial wrist replacements reviewed at an average of 52 months, five required revisions, yielding an 8-year survivorship probability of 83%.

Fracture of a Swanson Silastic implant (Preoperative radiographs) salvaged two years later with a biaxial total wrist arthroplasty.
The Universal Total Wrist Arthroplasty
Modern designs, such as the Universal total wrist implant, have shown promising results in early cohorts of patients with rheumatoid arthritis, as reported by Menon, Divelbiss, Sollerman, and Adams. These implants focus on anatomical center-of-rotation matching and minimal bone resection.
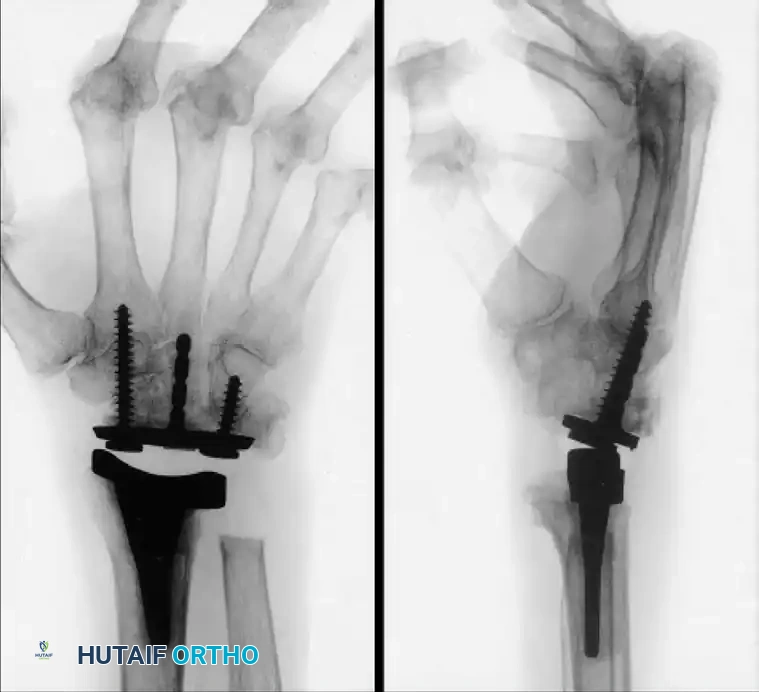
Long-standing rheumatoid disease and symptomatic wrist arthritis treated with a Universal total wrist arthroplasty, demonstrating excellent alignment and preservation of carpal height two years postoperatively.
Pitfall: Despite implant modifications, careful patient selection, close attention to meticulous surgical technique (especially soft-tissue balancing), and thoughtful consideration of salvage options (i.e., conversion to arthrodesis) are critical when implant arthroplasty is considered for a patient with incapacitating wrist arthritis.
TOTAL WRIST ARTHRODESIS (TWA): SURGICAL TECHNIQUES
Successful wrist arthrodesis reliably relieves pain, corrects deformity, and maintains stability. Several satisfactory techniques are available, most requiring robust internal fixation and autologous bone grafting (typically from the distal radius or iliac crest).
Fixation Modalities
Historically, fixation methods included:
* A Rush pin inserted between the second and third metacarpal shafts, driven through the carpus, and into the medullary canal of the radius, supplemented with a staple to prevent rotation.
* An intramedullary Steinmann pin combined with extensive bone grafting of the dorsum of the wrist.
* A Steinmann pin driven down the shaft of the third metacarpal with additional fixation by a staple or oblique pin. This specific technique permits concurrent operations on the metacarpophalangeal (MCP) joints, which is highly advantageous in the rheumatoid hand.
Note: While intramedullary pins are described historically, modern practice heavily favors dorsal spanning plate osteosynthesis (e.g., AO dynamic compression plates or specialized wrist fusion plates) due to superior biomechanical rigidity and higher union rates.
General Dorsal Approach for Arthrodesis
- Incision: A longitudinal dorsal incision is made centered over Lister's tubercle, extending from the distal third of the radius to the midshaft of the third metacarpal.
- Extensor Retinaculum: The third extensor compartment is opened, and the extensor pollicis longus (EPL) is transposed radially. The second and fourth compartments are elevated subperiosteally.
- Joint Preparation: The dorsal capsule is excised. The articular cartilage of the radiocarpal joint, midcarpal joint, and the carpometacarpal (CMC) joint of the third ray is meticulously denuded down to bleeding subchondral bone using a high-speed burr or osteotomes.
- Bone Grafting: Cancellous bone graft is packed into the decorticated spaces.
- Fixation: The chosen fixation device (pin or plate) is applied, ensuring the wrist is positioned in the pre-planned degree of extension or neutral alignment.
- Closure: The extensor retinaculum is repaired over the plate to protect the extensor tendons, leaving the EPL transposed in the subcutaneous tissue.
PARTIAL WRIST ARTHRODESIS
Partial arthrodesis (radiocarpal or midcarpal fusions) is highly useful to preserve motion in relatively uninvolved joints while stabilizing the wrist against pathological translation.
Radiocarpal Fusions
Radiocarpal fusions—such as radioscaphoid, radiolunate, or radioscapholunate fusions—are indicated when the midcarpal joint is spared. These procedures stabilize the radiocarpal joint against the ulnar translation commonly seen in rheumatoid arthritis.
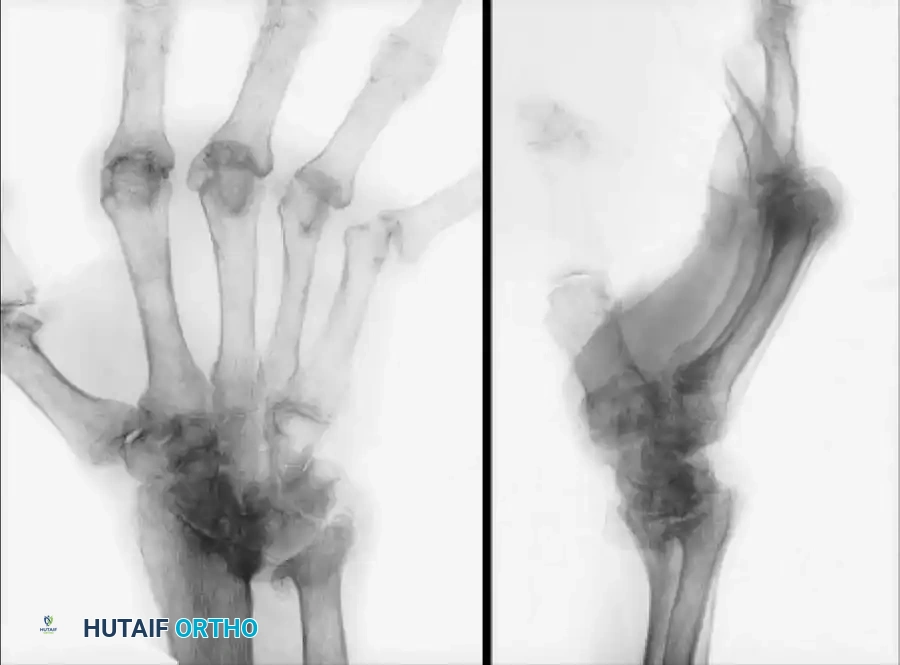
The Radiolunate (Chamay) Fusion:
This procedure is particularly effective for isolated radiolunate arthritis or to halt ulnar slide in the rheumatoid wrist while preserving the midcarpal articulation (capitolunate joint) for flexion and extension.


Ulnar subluxation in a 54-year-old woman with rheumatoid arthritis (Left), successfully stabilized and realigned after a radiolunate (Chamay) fusion (Right).
By fusing only the affected radiocarpal segment, the surgeon maintains the kinematic dart-thrower's motion arc, which is essential for many occupational and daily activities.
POSTOPERATIVE REHABILITATION AND OUTCOMES
Arthrodesis Protocol
- Immobilization: Following total wrist arthrodesis, the wrist is immobilized in a short-arm cast or rigid splint for 4 to 6 weeks, depending on the rigidity of the internal fixation.
- Therapy: Digital range of motion (ROM) is initiated immediately postoperatively to prevent tendon adhesions. Forearm rotation (pronation/supination) is permitted early if the distal radioulnar joint (DRUJ) is not involved.
- Radiographic Follow-up: Clinical and radiographic union is typically observed between 8 and 12 weeks, at which point strengthening exercises may commence.
Arthroplasty Protocol
- Immobilization: The wrist is placed in a bulky dressing and volar splint in neutral alignment.
- Therapy: At 10 to 14 days, sutures are removed, and a custom thermoplastic splint is fabricated. Gentle, active ROM of the wrist is initiated under the guidance of a certified hand therapist.
- Restrictions: Patients are permanently restricted from heavy lifting (typically >10 lbs) and impact loading to prevent premature implant wear, subsidence, or aseptic loosening.
In conclusion, the surgical management of the arthritic wrist demands a profound understanding of carpal kinematics, meticulous soft-tissue handling, and rigorous patient selection. Whether employing a motion-preserving arthroplasty or a definitive arthrodesis, the ultimate goal remains the restoration of a functional, pain-free hand capable of meeting the patient's daily demands.
