Volar Plating of Distal Radius Fractures
DEFINITION
Distal radius fractures are defined by their involvement of the metaphysis of the distal radius. They are assessed on the basis of fracture pattern, alignment, and stability:Articular versus nonarticular Reducible versus irreducible Stable versus unstableIrreducible or unstable fractures require surgical reduction and stable fixation.Volar plating historically has been the method of choice for volar shear-type fractures.Fixed-angle plates have become the preferred method of fixation for most types of distal radius fractures.
ANATOMY
The distal radius serves as a buttress for the proximal carpus, transmitting 75% to 80% of its forces into the forearm.The remaining 20% to 25% of force is transmitted through the distal ulna and the triangular fibrocartilage complex (TFCC).Thickness of distal radius articular cartilage is 1 mm or less. 16 DorsallyThe distal radius is the origin for the dorsal radiocarpal ligament.It is the floor of the fibro-osseous extensor tendon compartments and includes Lister tubercle, assisting in extensor pollicis longus function ( FIG 1A).The extensor tendons are in immediate contact with the dorsal surface of the distal radius.VolarlyThe distal radius is the origin for volar extrinsic ligaments of the wrist, including the radioscaphocapitate ligament and long and short radiolunate ligaments.It also is the origin of the pronator quadratus.The flexor tendons are separated from the distal radius by the pronator quadratus.UlnarlyThe distal radius is the origin for the triangular fibrocartilage (see FIG 1A).It also contains the sigmoid notch, which articulates with the head of the distal ulna, allowing forearm rotation.DistallyThe surface is divided into a triangular scaphoid fossa and a square lunate fossa articulating with each respective carpal bone ( FIG 1B).The distal articular surface is inclined approximately 22 degrees ulnarly in the coronal plane and 11 degrees volarly in the sagittal plane ( FIG 1C,D).The metaphysis is defined by the distal radius within a length of the articular surface that is equivalent to the widest portion of the entire wrist.The dorsal cortical bone is less substantial than the volar cortical bone, contributing to the characteristic dorsal bending fracture pattern of distal radius fractures.
PATHOGENESIS
The mechanism of injury in a distal radius fracture is an axial force across the wrist, with the pattern of injury determined by bone density, the position of the wrist, and the magnitude and direction of force.Most distal radius fractures result from falls with the wrist extended and pronated, which places a dorsal bending moment across the distal radius.Relatively weaker, thinner dorsal bone collapses under compression, whereas stronger volar bone fails under tension, resulting in a characteristic “triangle” of bone comminution with the apex volar and greater comminution dorsal.Other possible mechanisms form a basis for some fracture classifications such as the one proposed by Jupiter and Fernandez. 6BendingAxial compression ShearAvulsion CombinationsArticular involvement and its severity are the basis of some fracture classifications, such as the AO Orthopaedic Trauma Association (AO/OTA) 10 and Melone12 classifications.Articular involvement splits the distal radius into distinct fragments separate from the radius shaft ( FIG 2):Scaphoid fossa fragmentLunate fossa fragment. With comminution of this fragment may be separated into two impacted articular fragments, involving the dorsal ulnar corner and the volar rim. 11
NATURAL HISTORY



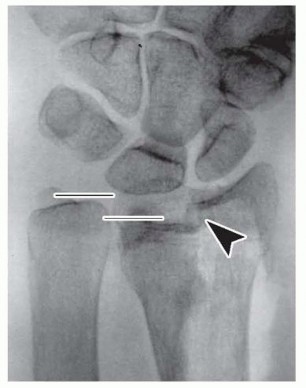
FIG 2 • Thearrowheadpoints to the articular split. Articular displacement of the scaphoid fossa fragment radially and the lunate fossa fragment ulnarly is apparent, as is significant shortening (ulnar positive variance) as outlined by thelines.By predicting the stability of a distal radius fracture, deformity and its complications can be minimized. Severalrisk factors have been suggested by LaFontaine et al 8 and others. The presence of three or more indicates instability:Dorsal (or volar apex) angulation greater than 20 degrees Dorsal comminutionIntra-articular extension Associated ulnar fracture Patient age older than 60 years
PATIENT HISTORY AND PHYSICAL FINDINGS
The mechanism of injury should be sought to assist in assessing the energy and level of trauma. Associated injuries are not uncommon and should be carefully ruled out.Injuries to the hand, carpus, and proximal arm, including other fractures or dislocations Injuries to other extremities or the head, neck, and torsoEstablish the patient's functional and occupational demands.Document coexisting medical conditions that may affect healing such as smoking or diabetes. Determine possible risk factors for anesthesia and surgery, such as cardiac disease.The physical examination should document the following:Condition of surrounding soft tissues (ie, skin and subcutaneous tissues)Quality of vascular perfusion and pulses Integrity of nerve functionSensory two-point discrimination or threshold sensory testingMotor function of intrinsic muscles, including thenar and hypothenar muscles, of the handP.304Examination of the distal ulna, TFCC, and distal radioulnar joint should rule out disruption and instability.Reliable physical examination of the carpus often is difficult, making radiographic review even more critical and follow-up examinations important.
IMAGING AND OTHER DIAGNOSTIC STUDIES



DIFFERENTIAL DIAGNOSIS
Diagnosis is directly confirmed by radiographs.Associated and contributory injuries should always be considered.Pathologic fracture (eg, related to tumor, infection)Associated injuries to the carpus (eg, scaphoid fracture, scapholunate ligament injury)
NONOPERATIVE MANAGEMENT
Nonoperative treatment is reserved for distal radius fractures that are reducible and stable based on the criteria previously discussed.The goal of nonoperative treatment is to immobilize the wrist while maintaining acceptable alignment until the fracture is healed.Goals for treatment 9P.305Radial inclination greater than 10 degrees Ulnar variance less than 3-mm positivePalmar tilt less than 10 degrees dorsal or 20 degrees volar Articular congruity with less than a 2-mm gap or step-offPatients are immobilized in a short-arm cast for 6 weeks. Radiographic follow-up is performed on a weekly basis for the first 2 to 3 weeks to identify fracture displacement that may warrant reduction.
SURGICAL MANAGEMENT
The goal of operative treatment is to achieve acceptable alignment and stable fixation.Various methods of fixation are available: pins, external fixators, intramedullary devices, and plates (volar, dorsal, fragment specific).
PREOPERATIVE PLANNING
Preoperative medical and anesthesia evaluation are performed as required.Discontinue blood-thinning medications (anticoagulants and nonsteroidal anti-inflammatory drugs, especially acetylsalicylic acid).Request necessary equipment, including fluoroscopic and power equipment.Confirm the plate fixation system to be used, and check the equipment before beginning surgery for completeness (ie, all appropriate drills, plates, and screws).Have a contingency plan or additional fixation (external fixator, bone graft, or bone graft substitute). Review and have previous radiographic studies available.Consider use of a regional anesthetic for postoperative pain control.
POSITIONING
Place the patient in the supine position with the affected extremity on an arm table. Apply an upper arm tourniquet, preferably within the sterile field.Incorporate weights or a traction system to apply distraction across the fracture ( FIG 4).The surgeon is seated so that the elbow is pointing toward the patient's torso and the dominant hand works toward the fingers of the patients.The assistant is seated opposite the surgeon.The fluoroscopy unit is brought in from the end or corner of the table.
APPROACH


FIG 4 • Traction is applied over the arm table with finger traps and hanging weights. The surgeon sits on the volar side and the assistant on the dorsal side. Fluoroscopy can be brought in from any direction but preferably from the side adjacent or the opposite surgeon.
TECHNIQUES
Volar Fixed-Angle Plate Fixation of the Distal Radius
Volar Fixed-Angle Plate Fixation of the Distal Radius
INCISION AND DISSECTION






FRACTURE REDUCTION AND PROVISIONAL FIXATION
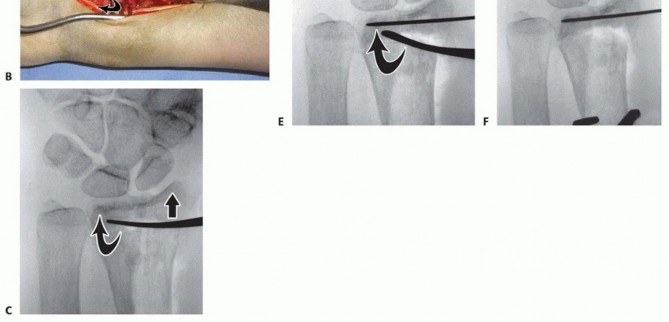
Apply a lobster claw clamp around the radius shaft at a perpendicular angle to the volar surface at the most proximal portion of the wound ( TECH FIG 2A).This allows for excellent control of the proximal shaft for rotation and translation, providing an excellent counterforce when correcting the dorsal angulation collapse.It also aids in soft tissue retraction.With the fracture now exposed, apply traction distally to distract and disimpact the fragments.Carefully clean the fracture of any interposed muscle, fascia, hematoma, or callus while maintaining the bony contours.In the case of significant volar comminution, reduce and provisionally stabilize the fragments with K-wires.Take plate positioning into account when placing these K-wires.The articular surface is first reduced, if necessary.Under fluoroscopic guidance, manipulate the articular fragments through the fracture with a periosteal elevator, osteotome, or K-wires ( TECH FIG 2B,C).Longitudinal traction is important during this reduction phase. It can be performed by an assistant or using crosstable weights and finger traps.A dorsal exposure is performed at this stage if there is significant articular impaction, particularly centrally, that cannot be corrected using the extra-articular technique described here.Place K-wires from the radial styloid fragment into the lunate fossa fragment to maintain the articularreduction ( TECH FIG 2D).The K-wires should be placed as close as possible to subchondral bone ( TECH FIG 2E,F).Once the distal articular reduction is complete, reduce the distal radius as a single unit to the radius shaft.Insert K-wires as required to maintain the provisional reduction between the distal fragments and the proximal shaft fragment.If radial collapse and translation are prominent, a large K-wire can be introduced into the radial portion of the fracture. By advancing it proximally and ulnarly, it behaves like an intrafocal pin, providing a radial buttress by pushing the distal fragment ulnarly.A similar technique can be applied through the dorsal fracture to assist in maintaining palmar tilt correction.
PLATE APPLICATION




DISTAL FRAGMENT REDUCTION
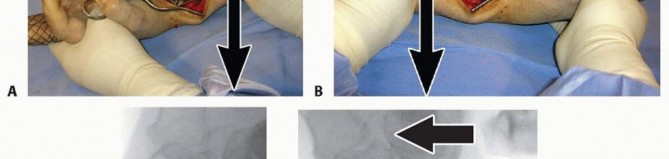
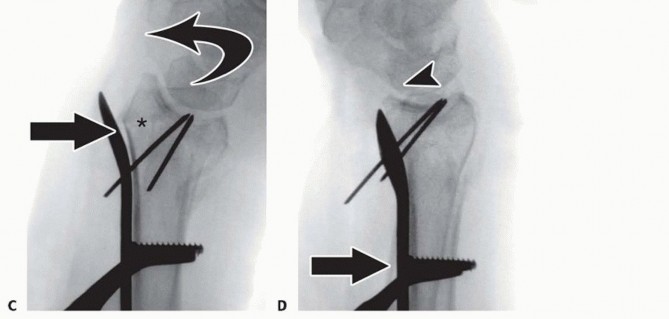
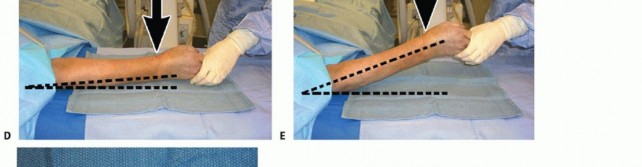
Once the plate has been secured proximally, execute any additionally needed reduction.A well-designed plate serves as an excellent buttress for correction of palmar tilt ( TECH FIG 4A).P.309Apply counterforce through the lobster claw clamp in a dorsal direction while the distal hand and wrist are translated palmarly and flexed ( TECH FIG 4B).This maneuver reduces the distal radius to the plate, effectively restoring volar tilt by pushing the lunate against the volar lip of the distal radius ( TECH FIG 4C,D).Additional distraction and ulnar deviation correct radial collapse and loss of radial inclination.
PLATE FIXATION

CLOSURE


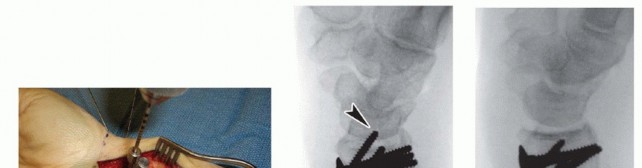
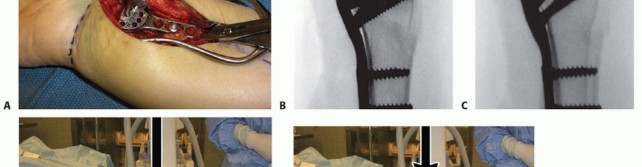
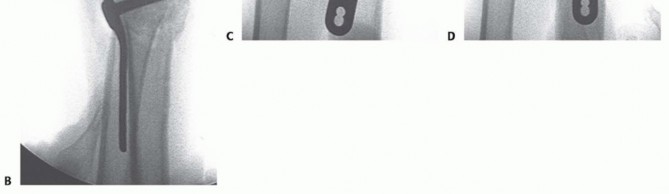
TECH FIG 7 • A. The volar plate is applied with the distal screws placed first (parallel to distal articular surface).(continued) P.312 TECH FIG 7 •(continued)B. Reducing the plate to the diaphysis proximally accomplishes the reduction. C. The plate is applied at approximately a 20-degree angle relative to the distal articular surface or to the amount of angulation that is estimated. D. By reducing the plate to the diaphysis, the distal angulation is corrected.

|Preoperative ▪ Obtain multiple radiographs in different positions (eg, several oblique views), planning especially in the setting of comminution or articular involvement.1.Obtain a CT scan if assessing the pattern of fracture when radiographs alone are difficult or uncertain.Surgical ▪ Avoid crossing the distal flexion creases of the wrist. approach ▪ Avoid ulnar exposure to the midline of the flexor carpi radialis.2.Use extra care with deep dissection in the presence of hematoma or significant swelling.Fracture ▪ Employ traction across the wrist with a device or weights.reduction ▪ Use a lobster claw clamp on the proximal radius shaft for control of the forearm and as a reference for the lateral margins.3.Use instruments to disimpact and reduce articular fragments through the fracture itself, either volarly, dorsally, or both.4.Employ a temporary K-wire to stabilize the reduction before placement of the plate.Plate ▪ Confirm appropriate radial-ulnar positioning of the proximal plate using a true AP radiograph (ie, forearm in supination with open view of the distal radioulnar joint).|Postoperative ▪ Closure of the pronator quadratus is not critical and should be reserved for more substantial muscles with limited trauma.1.Begin immediate ROM to digits with edema.1.Use K-wires to fix the plate provisionally to the proximal radius.2.The initial “oblong hole” screw should be slightly longer than the measured length to ensure better initial fixation.Plate fixation1.Confirm proper distal plate position on a true lateral view (ie, forearm 20 degrees off the table).2.Place the plate as distal as possible, up to the volar teardrop (watershed line) of the distal radius, if possible.3.Evaluate the screws for possible joint penetration using 360-degree fluoroscopic images.alignmentP.313
POSTOPERATIVE CARE
The wrist is splinted in a neutral position, leaving the digits free.If the fracture is particularly tenuous or there is injury to the ulnar wrist, a long-arm or sugar-tong (Munster) splint is applied.Vitamin C 500 to 1500 mg per day for 6 weeks is recommended to reduce the incidence of complex regional pain syndrome. 22The patient is instructed to perform active ROM exercises for the digits every hour and to engage in strict elevation for at least 3 days.It is critical to emphasize edema prevention and immediate ROM of the digits.At 1 week postoperatively, the splint is removed and the wound is examined.If swelling permits, the therapist fabricates a molded Orthoplast splint (Johnson & Johnson Orthopedics, New Brunswick, NJ) to be worn at all times.Active ROM exercises of the wrist are implemented 1 week postoperatively. At 4 to 6 weeks, putty and grip exercises are added.At 6 to 8 weeks, the splint is discontinued, and progressive strengthening exercises are advanced. If necessary, progressive passive ROM can begin, including use of dynamic splints.At 10 to 12 weeks, the patient usually can be discharged to all activities as tolerated.Elderly patients with distal radius fractures are at increased risk of sustaining other osteoporosis-related fractures. A referral to an osteoporosis clinic is advised.
OUTCOMES
Overall good to excellent results can be expected in over 80% of patients with ROM, strength, and outcomes scoring. 13,14,19,21Studies comparing volar fixation to other forms of fixation (eg, external fixators, pins, and dorsal plating) have revealed similar if not superior results.Results appear to be superior in the early recovery period, with the final outcome yielding equivalent results among all fixation groups.Some studies suggest better maintenance in overall reduction compared to other forms of fixation.
COMPLICATIONS
Complication rates as high as 27% have been reported.Complications can be categorized into those involving hardware, fracture, soft tissues, nerves, and tendons. 2Failures of hardware, such as plate or screw breakage, can occur but are rare. Usually, such failures are an indication of other problems, such as nonunion.The hardware becomes unacceptably prominent in a minority of patients.This complication may become evident only after some time has elapsed, as swelling of fibrous tissue subsides and bone remodels.The most common sites include the dorsal wrist, when screws have been inserted, and the radial wrist, when a plate has been used.It can be avoided with careful screw and plate placement and radiographic verification of their position.Nonunion and delayed union are unusual. Consider a diagnosis of osteomyelitis or other risk factors such as smoking.Loss of fracture reduction and fixation can occur and is most common in patients with osteopenic bone or comminuted and articular fractures.This can be avoided with frequent and early follow-up with repeat radiographs. If instability is suspected, the fracture can be casted.In the operating room, if instability is suspected, additional fixation should be considered (eg, external fixator, pins, bone graft).Soft tissue complications are proportional to the energy of the initial injury. Open wounds usually can be addressed with local measures.Significant swelling must be addressed with early and aggressive modalities. Swelling can lead to other complications, such as joint stiffness and tendon adhesions.Nerve injuries can be the result of initial trauma or subsequent surgical trauma.Assess and document neurologic status before surgery.Avoid further injury to nerves with careful placement of retractors.The palmar cutaneous branch of the median nerve can be injured during incision and exposure. Postoperative neuromas can cause pain and sensitivity along scar.Avoid the nerve with a well-placed incision radial to the flexor carpi radialis and careful deep dissection.Postoperative swelling also can lead to median neuropathy. Carpal tunnel release should be performed if there is any suspected compression neuropathy or if this is to be anticipated as a result of postoperative swelling.Tendon complications include adhesions and ruptures.Most tendon adhesions involve the dorsal extensor tendons resulting in extrinsic extensor tightness. Flexor tendon adhesions are uncommon and involve primarily the flexor pollicis longus.Tendon ruptures have been described, especially involving the flexor pollicis longus and the extensor pollicis longus, as a result of plate and screw prominence, respectively.The distal screws must not be left prominent, and caution must be applied when drilling.The sagittal and coronal profiles of the plate being used must be taken into consideration—some plates are very prominent and extend far radially.
REFERENCES
- Aro HT, Koivunen T. Minor axial shortening of the radius affects outcome of Colles' fracture treatment. J Hand Surg Am 1991;16(3): 392-398.
- Arora R, Lutz M, Hennerbichler A, et al. Complications following internal fixation of unstable distal radius fracture with a palmar lockingplate. J Orthop Trauma 2007;21(5):316-322.
- Fernandez JJ, Gruen GS, Herndon JH. Outcome of distal radius fractures using the short form 36 health survey. Clin Orthop Relat Res 1997;(341):36-41.
- Geissler WB, Freeland AE, Savoie FH, et al. Intracarpal soft-tissue lesions associated with an intra-articular fracture of the distal end of the radius. J Bone Joint Surg Am 1996;78(3):357-365.
- Joseph SJ, Harvey JN. The dorsal horizon view: detecting screw protrusion at the distal radius. J Hand Surg Am 2011;36(10):1691-1693.
- Jupiter JB, Fernandez DL. Comparative classification for fractures of the distal end of the radius. J Hand Surg Am 1997;22(4):563-571.P.314
- Knirk JL, Jupiter JB. Intra-articular fractures of the distal end of the radius in young adults. J Bone Joint Surg Am 1986;68(5):647-659.
- Lafontaine M, Hardy D, Delince P. Stability assessment of distal radius fractures. Injury 1989;20(4):208-210.
- Lichtman DM, Bindra RR, Boyer MI, et al. American Academy of Orthopaedic Surgeons clinical practice guideline on: the treatment of distal radius fractures. J Bone Joint Surg Am 2011;93(8):775-778.
- Marsh JL, Slongo TF, Agel J, et al. Fracture and dislocation classification compendium-2007: Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma 2007;21 (10 suppl):S1-S133.
- Medoff RJ. Essential radiographic evaluation for distal radius fractures. Hand Clin 2005;21(3):279-288.
- Melone CP Jr. Articular fractures of the distal radius. Orthop Clin North Am 1984;15(2):217-236.
- Musgrave DS, Idler RS. Volar fixation of dorsally displaced distal radius fractures using the 2.4-mm locking compression plates. J Hand Surg Am 2005;30(4):743-749.
- Orbay JL, Fernandez DL. Volar fixed-angle plate fixation for unstable distal radius fractures in the elderly patient. J Hand Surg Am 2004;29(1):96-102.
- Pogue DJ, Viegas SF, Patterson RM, et al. Effects of distal radius fracture malunion on wrist joint mechanics. J Hand Surg Am 1990;15(5):721-727.
- Pollock J, O'Toole RV, Nowicki SD, et al. Articular cartilage thickness at the distal radius: a cadaveric study. J Hand Surg Am 2013;38(8):1477-1481.
- Porter M, Stockley I. Fractures of the distal radius. Intermediate and end results in relation to radiologic parameters. Clin Orthop Relat Res 1987;(220):241-252.
- Richards RS, Bennett JD, Roth JH, et al. Arthroscopic diagnosis of intra-articular soft tissue injuries associated with distal radial fractures. J Hand Surg Am 1997;22(5):772-776.
- Rozental TD, Blazar PE, Franko OI, et al. Functional outcomes for unstable distal radial fractures treated with open reduction and internal fixation or closed reduction and percutaneous fixation. A prospective randomized trial. J Bone Joint Surg Am 2009;91(8): 1837-1846.
- Short WH, Palmer AK, Werner FW, et al. A biomechanical study of distal radial fractures. J Hand Surg Am 1987;12(4): 529-534.
- Wright TW, Horodyski M, Smith DW. Functional outcome of unstable distal radius fractures: ORIF with a volar fixed-angle tine plate versus external fixation. J Hand Surg Am 2005;30(2):289-299.
- Zollinger PE, Tuinebreijer WE, Breederveld RS, et al. Can vitamin C prevent complex regional pain syndrome in patients with wrist fractures? A randomized, controlled, multicenter dose-response study. J Bone Joint Surg Am 2007;89(7):1424-1431.
