Vascularized Bone Grafting of Avascular Scaphoid Nonunions
DEFINITION
Scaphoid fractures account for 60% of carpal bone fractures.Nonunions occur in up to 15% of scaphoid fractures and often result from delayed treatment, inadequate immobilization, displacement of the fracture, or proximal pole involvement or in the setting of avascular necrosis (AVN).
ANATOMY
The blood supply to the scaphoid travels in a distal to proximal direction and emanates from the radial artery. Intraosseous vessels traverse the scaphoid to supply the proximal pole.In about 30% of scaphoids, there is either a single or no vascular channel found reaching the proximal pole.Studies of vascularity of the distal radius have identified several sources of vascularized bone graft available for nonunion treatment.Animal studies of vascularized bone grafts have documented a significant increase in blood flow present when compared to nonvascularized grafts.
PATHOGENESIS

FIG 1 • A. Tenderness at the anatomic snuffbox is a classic finding of scaphoid nonunion. B. The radial styloid-scaphoid interface is the earliest site of degenerative change in scaphoid nonunions, and patients will often display tenderness at that location. C. The distal pole of the scaphoid is palpable at the base of the thumb on the palmar aspect of the wrist. Tenderness at this region is usually found in cases of scaphoid nonunion.
NATURAL HISTORY
Nonunion of the scaphoid severely alters the normal carpal biomechanics and subjects the cartilage to shear forces detrimental to its survival.
PATIENT HISTORY AND PHYSICAL FINDINGS
Often, patients recall injuring their wrists several years before developing pain severe enough to seek medical attention.Patients usually complain of limited range of wrist motion and pain, often with grip or weight bearing. The patients have often significantly reduced their activity level due to persistent pain.In most cases, the patient will experience tenderness to palpation at the anatomic snuffbox (FIG 1A), the radial styloid-scaphoid joint (FIG 1B), or the distal pole of the scaphoid (FIG 1C), which is palpable on the palmar side of the wrist.Wrists with established scaphoid nonunions have an arc of motion that is significantly reduced from the uninvolved side, primarily in extension.
IMAGING AND OTHER DIAGNOSTIC STUDIES

FIG 2 • A. Early radiographic appearance of scaphoid nonunion before degenerative change. B. Development of degenerative changes at the radial styloid-scaphoid interface. C. Advanced changes involving the entire scaphoid fossa. Magnetic resonance imaging (MRI) is useful in evaluating the scaphoid for vascularity, although definitive determination of avascularity may be difficult. Although contrast-enhanced MRI has shown improved sensitivity over noncontrast studies in detecting AVN, it may not be effective in detected AVN in up to 25% of cases.
DIFFERENTIAL DIAGNOSIS
Ligamentous injury to the wrist Wrist synovitisIntraosseous ganglia Primary AVN of the scaphoid
NONOPERATIVE MANAGEMENT
Nonoperative treatment is of limited usefulness for established nonunions.Investigators have attempted the use of bone stimulators, which use either electrical stimulation or ultrasound.There is little evidence in the literature supporting the use of these units for treatment of established scaphoid nonunions with AVN.
SURGICAL MANAGEMENT
A vascularized distal radial bone graft is indicated for scaphoid nonunions with and without evidence of avascularity.Correction of a “humpback deformity” requires extensive mobilization of the pedicle when attempting the use of a dorsally sourced graft, and a palmar vascularized graft may be more appropriate.For significant collapse, a nonvascular iliac crest graft may be required to create a compression-resistant construct.When early degenerative changes are present, a radial styloidectomy should accompany the use of a vascularized distal radial graft.The presence of more advanced degenerative joint disease or carpal malalignment is a contraindication to performing surgery to obtain bony union.Although the use of a vascularized graft distal radius has been shown to achieve union in 71% to 96% of scaphoid nonunions, the success rate in patients with AVN has been reported in the 50% to 60% range.1,6,9
PREOPERATIVE PLANNING
Radiographs must be evaluated to rule out carpal instability or the degenerative changes frequently found in established nonunions. When there has been the development of dorsal intercalary segmental instability (DISI), over 50% of patients undergoing vascularized grafting will suffer failure to achieve union.
POSITIONING
The patient is placed supine on the operating table with the arm placed on an arm board. Surgery is performed under tourniquet control.
APPROACH
Vascularized grafting may be carried out through a dorsal or palmar approach. Anatomic studies have shown that the dorsal irrigating vessels are further from the articular surface than irrigating vessels on the palmarsurface of the radius.5,8,10 The palmar vessels have been shown in some anatomic studies to be of greater diameter.3P.357
TECHNIQUES
Vascularized Radius Bone Grafting Using the 1,2 Intercompartmental Supraretinacular Artery
Vascularized Radius Bone Grafting Using the 1,2 Intercompartmental Supraretinacular Artery
EXPOSURE


GRAFT HARVEST


B. Kirschner wire placement is percutaneous, from distal to proximal. The 1,2 IC SRA is not dissected free; rather, it is left as part of the retinacular septum.The tourniquet is deflated, and perfusion of the vascularized bone graft is evaluated (TECH FIG 2C).
GRAFT PLACEMENT
The joint capsule is incised in the distal portion of the incision, and the scaphoid nonunion is identified.A radial styloidectomy greatly increases the exposure of the scaphoid and reduces the possibility of bone graft impingement.Intervening fibrous tissue and sclerotic bone are removed from the nonunion site using rongeurs and curettes to prepare the scaphoid for graft placement.Cancellous bone graft from the distal radius is packed proximally and distally to fill voids created by débriding sclerotic bone.The carefully contoured vascularized graft is then rotated into the nonunion site and press-fit into position, taking care to avoid torsion of the vascular pedicle (TECH FIG 3A).Kirschner wires are advanced from the distal pole of the scaphoid to the proximal pole to secure the graft in place (TECH FIG 3B).The radial capsule is closed loosely with absorbable suture, and the skin is closed in a routine fashion.The pedicle must not be compressed.The patient is placed in a short-arm thumb spica splint.2. Vascularized Distal Radial Bone Graft Using the Palmar Carpal Artery
EXPOSURE


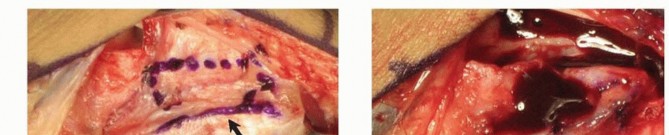
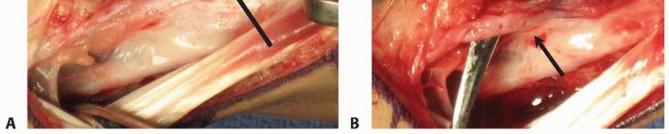
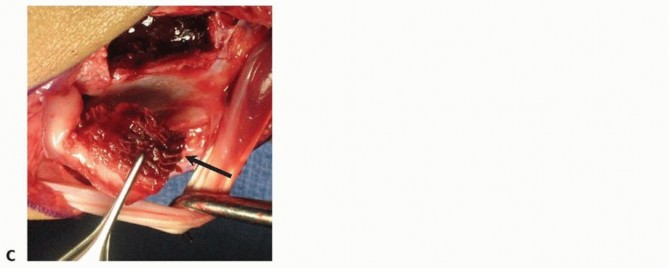
TECH FIG 4 • A. The palmar distal radius graft is harvested through the distal portion of the Henry approach to the distal forearm. B. The palmar carpal artery is exposed distal to superficial aponeurosis of the pronator quadratus. (continued)

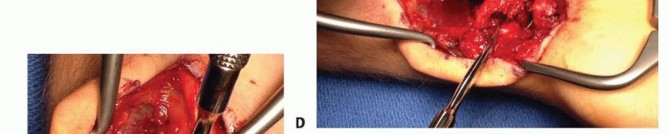

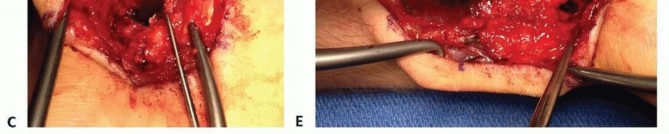
TECH FIG 4 • (continued) C. The scaphoid nonunion site (at tip of Freer elevator) is débrided to remove fibrous tissue. D. The palmar corticocancellous graft (in forceps) is rotated into the nonunion site. E. The graft is press-fit into the nonunion site and secured with internal fixation.
GRAFT HARVEST
Periosteum on either side of the palmar carpal artery is incised, and the artery is gently mobilized laterallyto the radial artery.Bone graft harvest from the ulnar half of the distal radius is initiated by periosteal incision with a scalpel, followed by osteotomy and elevation with small osteotomes.Incision through the radioscaphocapitate ligament exposes the scaphoid nonunion site and allow for removal of fibrous tissue (TECH FIG 4C).
GRAFT PLACEMENT
The graft is rotated and fitted into the nonunion site placing the cortical bone along the palmar surface (TECH FIG 4D).The graft is press-fit between the scaphoid proximal and distal portions while avoiding the vascular pedicle. Internal fixation is used to secure the bony elements (TECH FIG 4E).Repair of the radioscaphocapitate ligament is performed prior to final soft tissue closure.Avoid compression screw fixation.1. Graft fracture often will occur.2. Kirschner wire removal facilitates imaging studies.Perform a radial styloidectomy with the dorsal approach.1. Improves exposure and reducesthe chance of graft impingementDo not exsanguinate before tourniquet inflation.1. Visibility of the irrigating artery isenhanced with blood present in the vessels.The retinaculum should be opened over the radial side of thefirst compartment and the ulnar side of the second compartment when using the 1,2 IC SRA.1. This diminishes chances ofdamaging the irrigating artery.2. Graft is harvested from the radius just distal and dorsal to the brachioradialis insertion.The palmar carpal artery lies close to the articular surface ofthe distal radius.1. Care must be taken to avoid jointviolation with graft harvest.
PEARLS AND PITFALLS
P.360
POSTOPERATIVE CARE
Kirschner wires are removed when healing is observed, usually 4 to 6 weeks after surgery.CT scanning may be required to document complete healing before the patient resumes risky activities.MRI may be useful in evaluating the scaphoid for vascularity and may be done after Kirschner wire removal.
OUTCOMES
Recent reports have found successful union rates of 71% to 96% with the use of vascularized grafts from the distal radius. In cases with AVN, union rates have been reported in the 50% to 60% range.Previous reports have shown that patients with MRI evidence of AVN or loss of trabecular bone pattern noted on CT have a decreased level of success with reconstructive surgery. Treatment is rarely successful when both findings are present.A recent study has identified risk factors for failure: proximal pole AVN, radiographic degenerative changes, loss of carpal alignment, inadequate fracture fixation, tobacco use, advanced age, and female gender.4
COMPLICATIONS
Failure to gain unionProgressive degenerative changes Impingement of bone on radial styloid Infection
REFERENCES
- Chang MA, Bishop AT, Moran SL, et al. The outcomes and complications of 1,2-intercompartmental supraretinacular artery pedicled vascularized bone grafting of scaphoid nonunions. J Hand Surg 2006;31(3):387-396.
- Gras M, Mathoulin C. Vascularized bone graft pedicled on the volar carpal artery from the volar distal radius as primary procedure for scaphoid non-union. Orthop Traumatol Surg Res 2011;97:800-806.
- Haerle M, Schaller HE, Mathoulin C. Vascular anatomy of the palmar surfaces of the distal radius and ulna: its relevance to pedicled bone grafts at the distal palmar forearm. J Hand Surg Br 2003;28(2): 131-136.
- Hankins CL, Budoff JE. Analysis of wrist motion following vascularized bone graft to the proximal scaphoid. J Hand Surg 2011;36(4): 583-586.
- Sheetz KK, Bishop AT, Berger RA. The arterial blood supply of the distal radius and ulna and its potential use in vascularized pedicled bone grafts. J Hand Surg Am 1995;20(6):902-914.
- Shin AY, Bishop AT. Pedicled vascularized bone grafts for disorders of the carpus: scaphoid nonunion and Kienbock's disease. J Am Acad Orthop Surg 2002;10:210-216.
- Steinmann SP, Bishop AT, Berger RA. Use of the 1,2 intercompartmental supraretinacular artery as a vascularized pedicle bone graft for difficult scaphoid nonunion. J Hand Surg 2002;27(3):391-401.
- Waitayawinyu T, Robertson C, Chin SH, et al. The detailed anatomy of the 1,2 intercompartmental supraretinacular artery for vascularized bone grafting of scaphoid nonunions. J Hand Surg Am 2008;33(2):168-
- Waters PM, Stewart SL. Surgical treatment of nonunion and avascular necrosis of the proximal part of the scaphoid in adolescents. J Bone Joint Surg Am 2002;84-A(6):915-920.
- Zaidemberg C, Siebert JW, Angrigiani C. A new vascularized bone graft for scaphoid nonunion. J Hand Surg 1991;16(3):474-478.
