Vascularized Bone Grafting and Capitate Shortening Osteotomy for Treatment of Kienböck Disease


VASCULARIZED BONE GRAFTING
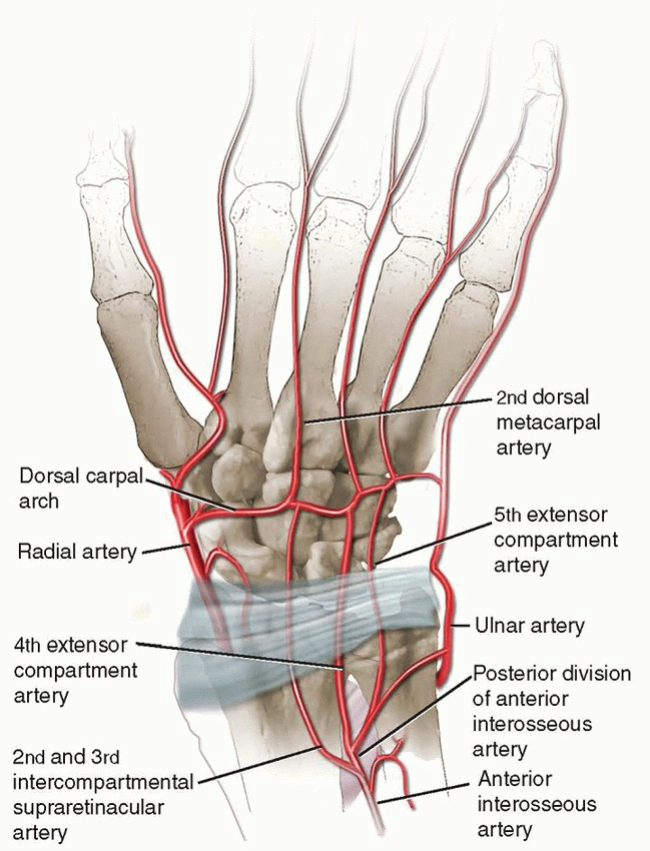
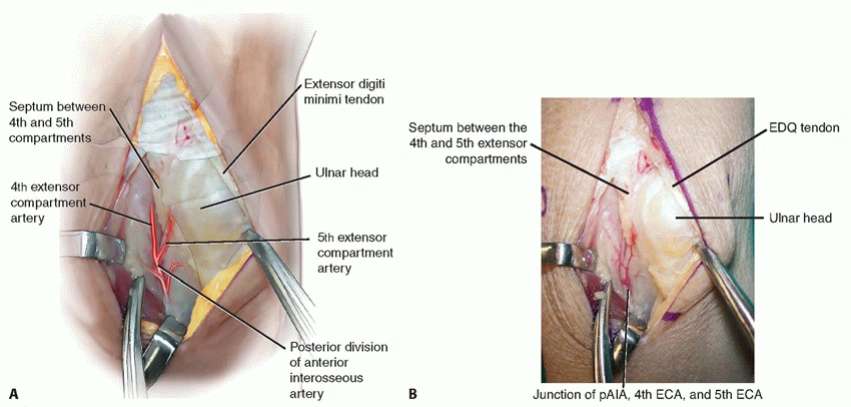
Exposure and Identification of the Fourth and Fifth Extensor Compartment Arteries1. Make a 5- to 6-cm longitudinal skin incision between fourth and fifth extensor compartments, ending distally between the third and fourth metacarpal bases.2. Incise the fifth extensor compartment.3. Identify the fifth ECA and its venae comitantes on the radial aspect of the compartment lying adjacent to or partially within the septum and separating the fourth and fifth extensor compartments (TECH FIG 1).7. Trace the fifth ECA proximally to its origin from the posterior division of the anterior interosseous artery as it emerges from the interosseous membrane.
TECHNIQUES
TECHNIQUES
TECHNIQUES
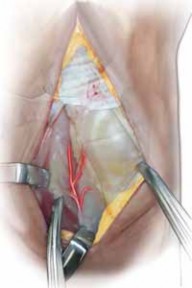
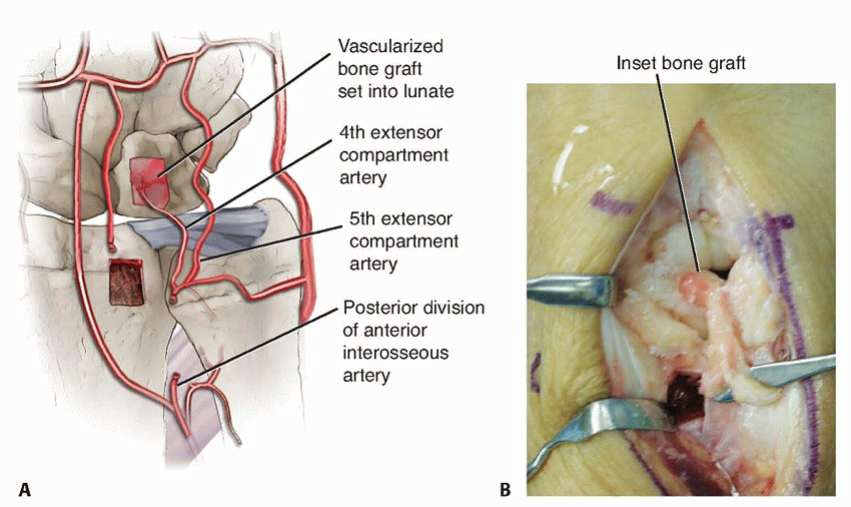
A BTECH FIG 3 • A, B. Drawing and corresponding clinical picture showing inset of the vascularized bone graft into the prepared lunate. Note the proximal–distal orientation of the cortex. (B: Copyright Thomas R. Hunt, III, MD.)
VASCULAR BUNDLE IMPLANTATION
Incision and Approach1. Make an extensive dorsoradial incision extending from the second metacarpophalangeal joint to a point about 4 cm proximal to the wrist, which gently slopes ulnarly around the tubercle of Lister.1. Visualize and protect the dorsal sensory branch of the radial nerve.2. Incise the extensor retinaculum over the third compartment and transpose the extensor pollicis longus into a subcutaneous position.3. Retract the contents of the fourth extensor compartment ulnarly and the second extensor compartment radially.4. Use fluoroscopy to confirm the lunate’s location.5. Perform a standard ligament-splitting capsulotomy.1. Take care to avoid injury to the transverse basal dorsal metacarpal arch from which the vascular pedicle arises.6. Inspect the lunate and surrounding joints. Perform a syn-ovectomy as required.Elevation of the Second Dorsal Metacarpal Vascular Pedicle7. In the interval between the second and third metacarpals, incise the interosseous muscle fascia from proximal to distal.1. The vessels lie underneath the aponeurosis that covers the interosseous muscles.8. Elevate the artery and venae comitantes along with a thin layer of surrounding perivascular areolar tissue fromthe second dorsal web space to the dorsal carpal arch (TECH FIG 4A).9. Identify and coagulate all branches off this main metacarpal artery.21. Ligate the vessel at its most distal location.1. This should provide a 5- to 6-cm vessel of adequate length to reach the dorsal lunate.Lunate Preparation and Implantation of the Vascular Bundle22. Curette and expand the lunate as discussed earlier.23. Pack autogenous cancellous bone graft into the lunate.24. Use a 2.7-mm bit and drill from dorsal to volar through the body of the lunate.25. Sew a 5-0 monofilament suture to the end of the mobilized vessel, then place the suture ends through the eye of a straight needle.26. Feed the vessel into the avascular portion of the lunate by passing the needle from dorsal to volar through the previously drilled hole, exiting the palmar skin just ulnar to the flexor carpi radialis tendon (TECH FIG 4B).27. Make a small skin incision over the needle and tie the suture over the palmar antebrachial fascia.28. Release the tourniquet to assess vessel patency.29. Achieve hemostasis and close the capsule, retinaculum, and skin in the manner described earlier.30. Apply a nonocclusive dressing and a volar, below-elbow splint.
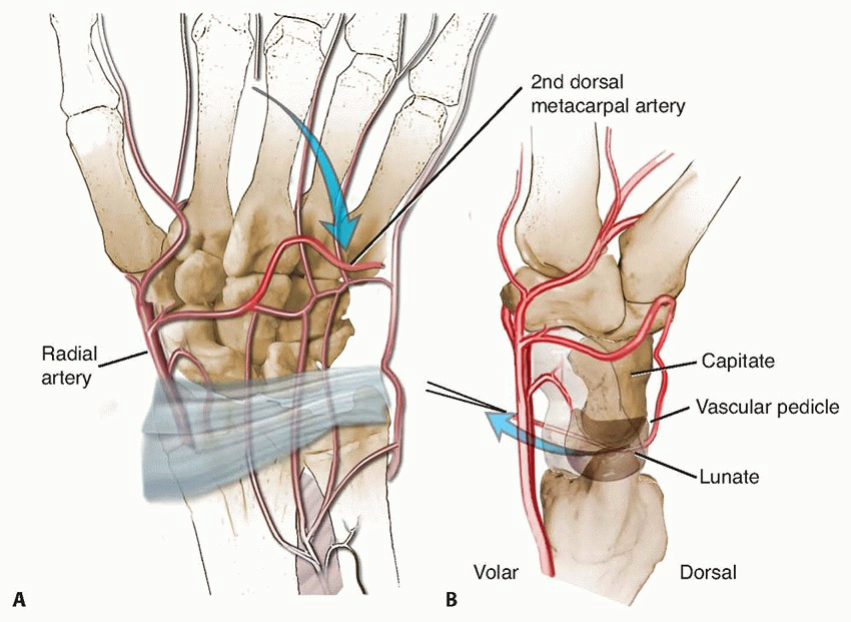
TECH FIG 4 • A. The artery has been ligated distally and mobilized proximally along with its perivascular tissue. B. Fine suture is sewn to the edge of the vessel lumen and placed into a straight Keith needle for insertion into the lunate from a dorsal to volar direction.
CAPITATE SHORTENING OSTEOTOMY
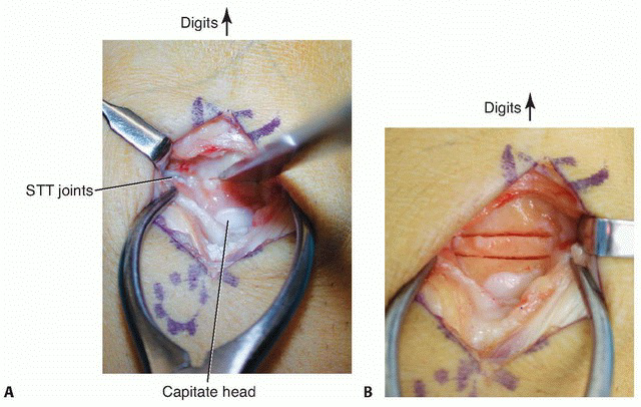
TECHNIQUES