UPPER EXTREMITY IN CEREBRAL PALSY: AN OVERVIEW
The management of the upper extremity in patients with cerebral palsy (CP) presents a complex clinical challenge that requires a profound understanding of neuro-orthopedic principles, upper limb biomechanics, and the natural history of spasticity. While a significant majority of patients with cerebral palsy—particularly those with spastic hemiplegia and quadriplegia—exhibit upper extremity involvement, only a highly select cohort (approximately 5%) are considered appropriate candidates for surgical intervention.
This stark contrast in surgical frequency compared to the lower extremity is rooted in the fundamental biomechanical goals of the respective limbs. In the lower extremity, the primary objective is to achieve painless, plantigrade stability to facilitate ambulation or transfers—a mechanical goal that is relatively straightforward to accomplish through tendon lengthenings, osteotomies, and arthrodeses. Conversely, the primary function of the upper extremity is dynamic: to position the hand in three-dimensional space to perform highly complex, fine-motor activities. Achieving functional mobility in a spastic, dyskinetic, or neurologically impaired upper limb is exponentially more difficult than achieving static stability in a lower limb.
The Role of Sensory Deficits and Neglect
A critical factor limiting the success of upper extremity surgery in cerebral palsy is the high prevalence of profound sensory deficits. The upper extremity movement disorder in CP is rarely an isolated motor phenomenon; it is frequently coupled with significant impairments in proprioception, stereognosis, barognosis, and light touch. Normal sensation in the affected hand is exceptionally rare.
Clinical Pearl: Motor function is inextricably linked to sensory feedback. A hand that lacks stereognosis and proprioception will often be functionally ignored by the patient, leading to a phenomenon known as "developmental disregard" or complete neglect of the affected extremity. Reconstructive motor surgery on a profoundly insensate, neglected hand will not yield functional improvement.
Patient Selection and Prognostic Indicators
The decision to proceed with surgical intervention must be highly individualized. Children who are most likely to benefit from upper extremity surgery generally fall into two distinct clinical categories:
- The Highly Functioning Patient: These are children with good volitional control who experience specific mechanical difficulties with activities of daily living (ADLs), such as dressing, feeding, and personal hygiene, secondary to spasticity or myostatic contractures.
- The Severely Involved Patient: These are non-ambulatory, often quadriplegic children with profound, fixed contractures and severe deformities. In this cohort, the goals are palliative rather than functional: alleviating pain, facilitating nursing care, and preventing or treating severe skin maceration and breakdown (particularly in the antecubital fossa and palmar creases).
Positive Predictors for Surgical Success:
* High intrinsic motivation and emotional stability.
* Reasonable cognitive intelligence to participate in postoperative rehabilitation.
* Absence of sensory neglect.
* Good voluntary motor control and baseline strength.
* Relatively preserved sensation (especially two-point discrimination and stereognosis).
Management of Severe Spasticity and Athetosis:
Children with severe spasticity, athetosis, and profound neglect are generally poor candidates for dynamic tendon transfers. However, they may still benefit significantly from static joint-stabilizing procedures, such as wrist or thumb arthrodesis, to correct severe positional deformities, improve hygiene, and reduce pain.
Surgical Warning: It is paramount to ensure that the patient's family and caregivers have realistic expectations regarding the goals of upper extremity surgery. The objective is rarely to create a "normal" limb, but rather to achieve specific, targeted improvements in function or care. Unrealistic expectations are the primary cause of postoperative dissatisfaction.
Preoperative Evaluation and Pathoanatomy
Comprehensive preoperative evaluation should include a multidisciplinary assessment. Ancillary studies, such as dynamic kinetic electromyography (EMG), are highly valuable in differentiating between muscles that are continuously spastic, those that fire out of phase, and those that are under volitional control. This distinction is critical when planning tendon transfers or lengthenings.
The most common upper extremity deformities in cerebral palsy are predictable deformities of position, driven by the predictable patterns of upper motor neuron spasticity:
* Shoulder: Internal rotation and adduction (driven by the pectoralis major, subscapularis, and latissimus dorsi).
* Elbow: Flexion (driven by the biceps brachii, brachialis, and brachioradialis).
* Forearm: Pronation (driven by the pronator teres and pronator quadratus).
* Wrist: Flexion (driven by the flexor carpi ulnaris and flexor carpi radialis).
* Thumb: Flexion and adduction ("thumb-in-palm" deformity).
* Fingers: Flexion deformities.
The overarching function of the upper extremity is to serve as a dynamic crane to position the hand in space. If the hand possesses functional capacity (grasp and release), proximal procedures to correct shoulder, elbow, and forearm deformities are highly useful in maximizing overall limb utility. Johnstone et al. demonstrated in a review of 84 limbs (64 patients) with an average 4-year follow-up that carefully selected patients experience statistically significant improvements in functional status, hygiene, and cosmetic appearance following upper extremity reconstructive surgery.
MANAGEMENT OF THE SHOULDER
Contracture of the shoulder or spasticity of the glenohumeral musculature is usually not sufficiently disabling to justify isolated surgical intervention. The typical deformity is a combination of adduction and internal rotation. Because gravity assists with shoulder extension and adduction, patients can often compensate for these limitations better than they can for distal deformities.
When the internal rotation and adduction contracture is severe enough to impede hygiene, dressing, or the positioning of a functional hand, surgical intervention is indicated.
Surgical Options for the Shoulder:
* Soft Tissue Releases: Procedures such as the Fairbank operation, as modified by Sever, involve the release of the contracted internal rotators (subscapularis, pectoralis major) and adductors. These are conceptually similar to procedures performed for obstetrical brachial plexus palsy.
* Bony Procedures: In cases of fixed, severe internal rotation deformity where the joint capsule and bony architecture have adapted, a rotational osteotomy of the humerus performed at the level of the deltoid tubercle is highly effective. This extra-articular procedure reorients the functional arc of motion without sacrificing the stabilizing musculature of the rotator cuff.
MANAGEMENT OF THE ELBOW
Elbow flexion contractures are a hallmark of the spastic upper extremity. The constant hypertonia of the biceps brachii, brachialis, and brachioradialis eventually leads to myostatic contracture of the muscle-tendon units and secondary contracture of the anterior elbow capsule.
As previously noted, two distinct groups of patients benefit from surgical procedures around the elbow:
1. Highly Functioning Patients: Those with useful hand function whose elbow flexion contracture limits their forward reach, thereby restricting their "functional sphere."
2. Severely Involved Patients: Those with profound, fixed contractures leading to severe hygiene issues, recurrent fungal infections, and skin breakdown in the antecubital fossa.
Surgical Warning: The Neurovascular Tether
When releasing a severe, chronic flexion contracture around the elbow, the surgeon must absolutely avoid acutely extending the elbow fully on the operating table. The brachial artery and the median nerve, having been chronically positioned in a flexed posture, undergo adaptive shortening. Acute, forceful extension can result in catastrophic stretch-induced neuropraxia of the median nerve or intimal tear and thrombosis of the brachial artery. Extension must be achieved gradually through postoperative serial casting or splinting.
Release of Elbow Flexion Contracture (Mital Procedure)
Mital et al. established the benchmark for anterior elbow releases, reporting excellent outcomes in 32 procedures with zero neurovascular injuries and no recurrence of deformity.
Indications for the Mital Anterior Elbow Release:
* A fixed elbow flexion contracture of 45 degrees or greater.
* A functional flexion attitude of the elbow of 100 degrees (10 degrees above a right angle) that significantly interferes with the patient's ability to reach forward with a functional forearm and hand.
It should be noted that other procedures designed primarily to improve forearm supination and hand function—such as the fractional lengthening or release of the flexor-pronator muscle origins from the medial epicondyle—often result in a mild, secondary gain in elbow extension.
🔪 Surgical Technique: Mital Anterior Elbow Flexion Release
Positioning and Preparation:
* Place the patient in the supine position.
* The entire upper extremity is prepped and fully draped free to allow intraoperative assessment of the full arc of motion.
* A sterile pneumatic tourniquet is applied high on the arm. While the procedure can be performed without a tourniquet, its use is highly recommended to ensure meticulous visualization of the neurovascular structures in the antecubital fossa.
Incision and Superficial Dissection:
* Approach the antecubital space utilizing a gently curving S-shaped incision centered over the anterior flexor crease. Avoid straight incisions across the flexion crease to prevent postoperative hypertrophic scarring and secondary skin contractures.
* Carefully dissect through the subcutaneous tissue. Identify, isolate, and, if necessary, ligate the superficial veins (e.g., median cubital vein) that cross the operative field.
Deep Dissection and Tendon Isolation:
* Incise the deep fascia to expose the muscle belly of the biceps brachii proximally.
* Follow the biceps muscle distally to identify its tendinous insertion and the medially radiating lacertus fibrosus (bicipital aponeurosis).
* Isolate the lacertus fibrosus and resect it completely. This structure often acts as a significant secondary tether to extension and pronation.
* Neurovascular Protection: Identify the lateral antebrachial cutaneous nerve as it emerges between the biceps and the brachialis laterally. Protect this nerve and retract it laterally to prevent painful postoperative neuromas.
Tendon Lengthening:
* With the nerve protected, partially flex the elbow to relieve tension on the neurovascular bundle.
* Free the biceps tendon down to its insertion on the bicipital tuberosity of the proximal radius.
* Perform a formal Z-plasty lengthening of the biceps tendon.
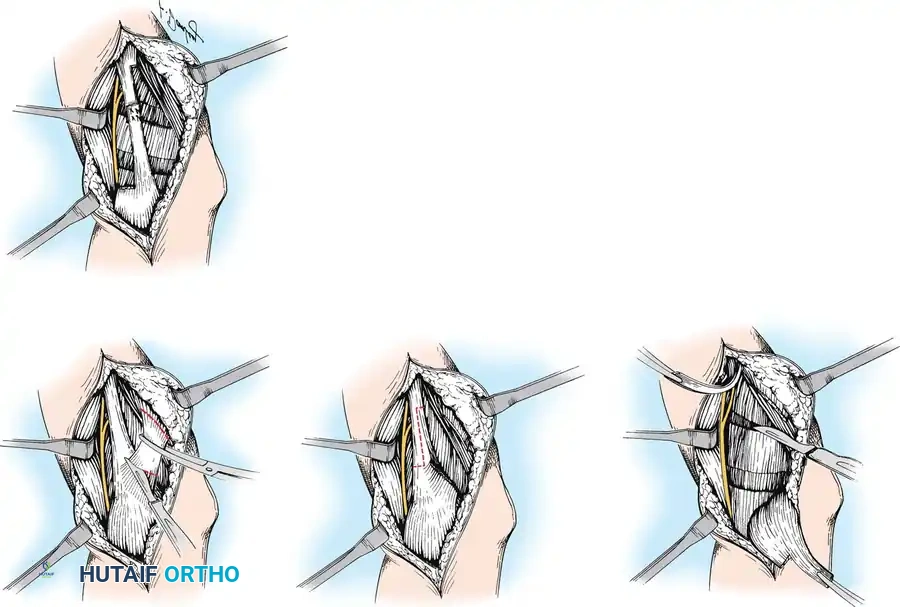
- Once the biceps tendon is divided, the musculofascial surface of the underlying brachialis muscle is exposed.
- Critical Anatomy: The radial nerve lies lateral to the brachialis muscle, while the brachial artery and median nerve lie medial to it. These structures must be definitively identified and protected with blunt retractors.
- Extend the elbow maximally (within safe limits). Circumferentially incise the aponeurotic tendinous fibers of the brachialis muscle at its distal end. This fractional lengthening should be performed at one or two levels, allowing the muscle to stretch while maintaining continuity of the underlying muscle fibers.
Capsulotomy and Closure:
* Assess the degree of extension. If a rigid, bony-like block remains, perform an anterior elbow capsulotomy.
* Hemostasis Check: Deflate the tourniquet before closure. Secure meticulous hemostasis. This is critical, as a postoperative hematoma in the antecubital fossa can lead to severe scarring or compartment syndrome.
* With the elbow extended to its new, safe maximum, repair the previously divided biceps tendon using the Z-plasty limbs.
* Perform a final, direct visual inspection to ensure the integrity and lack of undue tension on the median nerve and brachial artery.
* Close only the subcutaneous tissue and the skin. Do not close the deep fascia.
* Immobilize the arm in a well-padded, long-arm cast. The elbow should be positioned in maximal—but strictly not forceful—extension, with the forearm fully supinated.
* Bivalve the cast immediately in the operating room to accommodate postoperative swelling.
Postoperative Protocol and Rehabilitation
The success of the Mital release relies heavily on strict adherence to the postoperative rehabilitation protocol.
- Days 1-2: The arm is strictly elevated for 48 hours to minimize edema. Active and passive finger motion is encouraged immediately to promote venous return and prevent distal stiffness. The bivalved cast must be loosened immediately if any signs of excessive swelling or neurovascular compromise occur.
- Day 4: The initial surgical dressing is taken down and changed. Wound healing is assessed.
- Day 5: Active and active-assisted flexion and extension exercises are initiated out of the cast.
- Weeks 1-6: For the first 6 weeks postoperatively, the arm is replaced in the bivalved cast (or a custom-molded thermoplastic splint) in maximal extension whenever the patient is not actively performing their exercise regimen.
- Week 3: Pronation and supination exercises are formally added to the therapy protocol.
- Months 1-6: Nighttime extension splinting is mandatory and must be continued for a minimum of 6 months. The spastic drive of the flexors remains, and without prolonged splinting, recurrence of the contracture is highly likely.
- Expected Outcome: Maximal functional elbow extension is typically achieved between 3 to 5 months postoperatively, provided the patient and family are compliant with the splinting and therapy regimens.
FOREARM, WRIST, AND HAND
Deformities distal to the elbow—specifically pronation contractures of the forearm, flexion/ulnar deviation of the wrist, and complex spastic deformities of the hand (such as the swan-neck deformity, thumb-in-palm deformity, and intrinsic plus posturing)—require highly specialized assessment. The intricate balance of the extrinsic and intrinsic musculature of the hand in the spastic patient dictates a unique set of surgical principles, including fractional lengthenings, selective motor neurectomies, and complex tendon transfers.
