DEFINITION
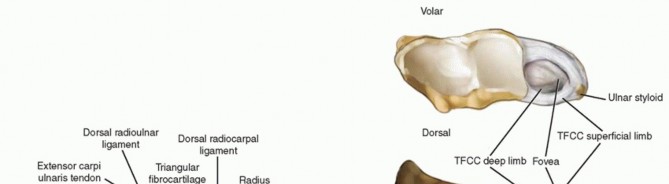
Ulnar impaction syndrome (ulnocarpal abutment) results from a chronic compressive overloading of the ulnocarpal articulation secondary to static or dynamic ulnar positive variance.Ulnar variance defines the relationship of the length of the ulna to that of the radius.Ulnar positive variance can be the result of a congenital anomaly; traumatic radial shortening from a distal radius, Essex-Lopresti, or Galeazzi fracture; injury to the distal radius physis; or a variant of normal anatomy.An ulnar shortening osteotomy is designed to decompress the ulnocarpal joint while simultaneously tightening the ulnocarpal and radioulnar marginal ligaments of the triangular fibrocartilage complex (TFCC).16Ulnar shortening osteotomy has been shown to be an effective alternative to TFCC repair in in the management of Palmer type IB tears.20Ulnar shortening osteotomy has been shown to be effective in reducing symptoms of isolated posttraumatic lunotriquetral ligament tears regardless of preoperative ulnar variance.13 FIG 1 • A. The soft tissue structures encompassing the TFCC of the wrist stabilizing the radioulnocarpal unit. The TFCC proper originates from the radius medially and attaches to the base of the ulnar styloid. Fibers originating from the subsheath of the ECU dorsally cross path with fibers originating from the ulnocarpal ligaments volarly and blend with the TFCC proper. B. DRUJ ligaments. (The disc component of the TFCC has been removed to show the deep limbs of the radioulnar ligaments.) The volar and dorsal radioulnar ligaments are the major soft tissue stabilizers of the DRUJ and insert onto the base of the ulnar styloid.R,radius;U, ulna.
ANATOMY
The distal radius has three articular surfaces: the scaphoid fossa, the lunate fossa, and the sigmoid notch.The radius articulates with and rotates around the ulnar head via the sigmoid notch. The sigmoid notch has welldefined dorsal, palmar, and distal margins, whereas the proximal margin is indistinct.The distal radioulnar joint (DRUJ) and ulnocarpal relationships are maintained by numerous ligamentous structures (FIG 1A).The interosseous membrane is a complex structure with a thickened central portion. It almost completely spans the radius and ulna, acting as a hinge for forearm rotation.The diaphysis of the distal half of the ulna is supplied by small segmental branches from the anterior and posterior interosseous arteries. These enter the ulna in 1- to 3-cm intervals from the direction of theinterosseous membrane and must be protected during the surgical approach.26P.1046The dorsal capsule of the DRUJ contains two ligaments: the proximal metaphyseal arcuate ligament and the distal radioulnar ligament. The palmar capsule is composed of a single radioulnar ligament.1The TFCC spans the ulnocarpal joint and connects the distal radius to the distal ulna (FIG 1B). The TFCC functions to cover the distal ulna, to partially dampen and transmit a portion of the axial load of the wrist through the ulna, to stabilize the DRUJ, and to provide support for the ulnar side of the carpus.The TFCC contains a central avascular articular disc composed of types I and II collagen. It is of variable thickness (average, 2 mm) and chiefly functions in load transmission between the ulnar head and ulnar carpus.The articular disc is connected to the peripheral palmar and dorsal radioulnar (marginal) ligaments, which originate on the medial border of the distal radius and insert into the base of the ulnar styloid at the fovea. These ligaments are composed of linear type I collagen and are stabilizers of the DRUJ.The ulnolunate and ulnotriquetral ligaments originate from the ulnar fovea and pass palmar to the palmar radioulnar ligament. They traverse the palmar surface of the TFCC to insert on their respective carpal bones. These ulnocarpal ligaments stabilize the ulnar side of the carpus relative to the ulna and resist carpal supination.The periphery of the TFCC is supplied by dorsal and palmar branches of the anterior interosseous artery and the ulnar artery. Because of this vascular distribution, injuries to the periphery of the TFCC are capable of healing and are often amenable to repair. Injuries to the central avascular portion of the articular disc do not heal in a predictable manner and are often treated with débridement.
PATHOGENESIS
Normal ulnar variance ranges from neutral to plus or minus 2 mm. The average axial load transmitted across the TFCC and subsequently the ulna is 20% if ulnar variance is neutral. An ulnar positive variance of 2.5 mm increases the load across the distal ulna to 42.7%, whereas an ulnar variance of −2.5 mm decreases the ulnarload to 3.1% (Table 1).19Congenital or acquired ulnar positive variance (FIG 2) can lead to degenerative wear of the TFCC and surrounding structures.The Palmer classification divides TFCC lesions into traumatic (type I) or degenerative (type II).18 Type II lesions are associated with ulnocarpal impaction and are further subdivided based on the severity and the other structures involved. Type II TFCC tears are generally not amenable to direct repair.Type IIA: TFCC wearType IIB: TFCC wear plus lunate or ulnar head chondromalaciaType IIC: TFCC perforation plus lunate or ulnar head chondromalaciaType IID: TFCC perforation plus lunate or ulnar head chondromalacia plus lunotriquetral ligament perforationType IIE: TFCC perforation plus lunate or ulnar head chondromalacia plus lunotriquetral ligament perforation plus ulnocarpal arthritisUlnar Length (mm)|Amount Removed of the Articular Disc of the Triangular Fibrocartilage Complex—|—None 1/3 2/3aAlla****Neutral|17.6%|16.1%|13.4%|8.0%---------−2.5|3.1%|2.7%|2.4%|2.3%+2.5|42.7%|41.9%|36.1%|26.3% Table 1 Percentage of Force Transmitted through the Ulna (Nine Arms) aRemoval of two-thirds or more of the horizontal portion of the triangular fibrocartilage complex statisticallydecreased the percentage of force through the nine ulnas tested. (Adapted from Palmer AK, Werner FW. The triangular fibrocartilage complex of the wrist—anatomy and function. J Hand Surg Am 1981;6[2]:153-162.)
NATURAL HISTORY
Defining the natural history of ulnocarpal impaction syndrome is at best challenging.The Palmer classification provides an accurate anatomic description of the degenerative changes seen in the ulnocarpal structures, but it does not dictate treatment, suggest prognosis, or indicate timing of progression.Deterioration of the ulnocarpal structures is very common regardless of ulnar variance. Numerous cadaveric studies have found TFCC perforations and chondromalacia of the ulnar head, lunate, and triquetrum in up to 70% of “normal specimens.”12,19Ulnar positive variance and persistent heavy demand across the ulnocarpal joint can hasten the development of the disease.An individual’s ability to unload the ulnar side of the wrist with conservative measures and change of lifestyle may slow or even prevent progression.
PATIENT HISTORY AND PHYSICAL FINDINGS

FIG 2 • Radiograph of Madelung deformity showing congenital ulnar positive variance. P.1047Analysis of whether the pain was caused by an acute injury or brought on by repetitive motion activitiesA distal radius or radial head fracture can lead to ulnocarpal impaction, as can a chronic distal radius physeal injury (ie, the gymnast’s wrist).Characterization of the painDescription of the location, duration, and radiation of the pain as well as any associated swelling, burning or tingling sensations, or sounds (clicks, etc.)Aggravating and alleviating factorsThe physical examination should always begin with inspection.The wrist and elbow should be examined for surgical scars.Prominence of the ulna either palmarly or dorsally may indicate instability of the DRUJ. A palmar sag and a supination posture of the wrist may indicate the capsuloligamentous instability that occurs in rheumatoid arthritis.Swelling, bruising, perforations of the skin, or obvious dislocations may indicate trauma. Intrinsic atrophy and clawing may indicate ulnar nerve pathology.Splinter hemorrhages beneath the nails and decreased turgor in the volar digital pads suggest vascular insufficiency.Single-finger palpation should proceed in a systematic fashion by isolating anatomic structures. The examination should be performed with the patient’s elbow resting on a table, the hand pointing toward the ceiling, and the forearm in a neutral position.Tenderness over any anatomic structure suggests a specific clinical diagnosis.Active and passive range-of-motion (ROM) maneuvers may illicit pain, suggesting pathology. Limitations of ROM may be the result of swelling or obstruction (blocking). The examiner should listen for sounds of pathology throughout ROM.Specific provocative tests should be performed in an attempt to further define the injured structure(s).Piano key test: A positive result is characterized by painful laxity in the affected wrist compared with the contralateral wrist, suggesting DRUJ synovitis.Ulnar compression test: A positive test is exacerbation of pain, which suggests arthritis or instability; dorsal or palmar subluxation may be noted.Lunotriquetral ballottement test: Used to elicit laxity associated with pain and crepitus in the presence of lunotriquetral instabilityReagan shuck test: Positive if pain and clicking at the lunotriquetral joint is present, suggesting lunotriquetral ligament perforation or disruption
IMAGING AND OTHER DIAGNOSTIC STUDIES
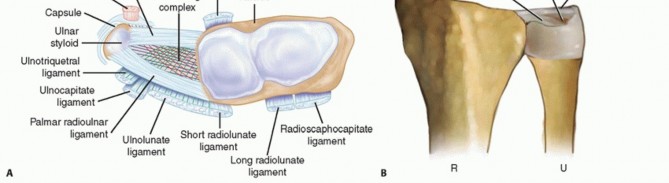
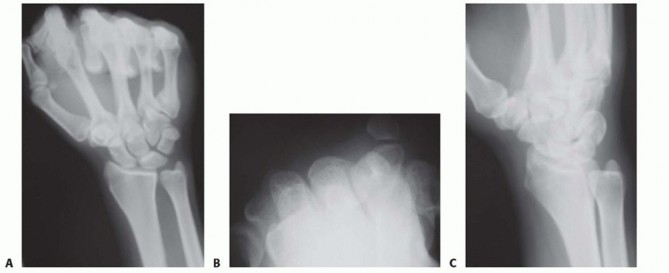
Plain radiographic views should include neutral rotation posteroanterior and lateral projections of both wrists. These are obtained with the patient seated and the elbow flexed at 90 degrees and the shoulder abducted at 90 degrees.The contralateral wrist films may be used as a template for reconstruction.Radiographic assessment of ulnar variance has used a neutral rotation radiographic view of the wrist that provides an image of the radioulnar length with the wrist unloaded. Such views may underestimate variancein wrists in which power grip and pronation result in significant proximal migration of the radius. Tomaino25 found that ulnar variance increased an average of 2.5 mm using the pronated grip view and ranged from an increase of 1 to 4 mm (FIG 3A).Other plain views may be obtained based on clinical suspicion.The carpal tunnel (FIG 3B) view visualizes the hook of the hamate and the pisotriquetral joint. An oblique view in 30 degrees of pronation (FIG 3C) allows evaluation of the dorsoulnar wrist.The reverse oblique view (30 degrees of supination) (FIG 3D) allows evaluation of the palmar ulnar wrist with a profile of the pisotriquetral joint.An ulnar deviation posteroanterior view (FIG 3E) may reveal lunotriquetral instability or evidence of ulnocarpal abutment. If ulnocarpal abutment is suspected, it is often useful to obtain a posteroanterior radiograph with the forearm in pronation and the fist clenched (see FIG 3A), which increases ulnar variance.Videofluoroscopy is useful for evaluating dynamic ligament instabilities. The wrist should be examined through an entire active and passive ROM as well as with provocative maneuvers in an attempt to demonstrate pathology while reproducing symptoms.Arthrography may demonstrate a TFCC defect or interosseous ligament disruption if contrast material injected into one compartment leaks into an adjacent space.Magnetic resonance imaging (MRI) can aid in the detection of soft tissue and osseous lesions, including interosseous and extrinsic ligament tears, TFCC defects, tumors, avascular necrosis, and occult fractures (FIG 3F).Sensitivity of the MRI increases if it is combined with arthrography. The ability to show marrow changes in the ulnar portion of the lunate and simultaneous central TFCC pathology is very helpful in confirming a diagnosis of ulnocarpal impaction.Arthroscopy can confirm a diagnosis suggested by findings from other diagnostic modalities.This is the most sensitive tool for diagnosis of chondral and ligamentous pathology.It has therapeutic applications in the management of ulnar abutment, TFCC defects, interosseous ligament tears, chondral defects, loose bodies, synovitis, and degenerative arthritis.Bone scan, ultrasonography, and computed tomography serve a very limited role in the diagnosis of ulnar impaction syndrome.
DIFFERENTIAL DIAGNOSIS
NONOPERATIVE MANAGEMENT
Rest and avoidance of any aggravating maneuvers are the mainstay of nonoperative management for ulnar impaction syndrome.The success of this treatment lies with the patient’s ability to change the way he or she does any number ofroutine tasks and may involve a change of employment.Ice and elevation may help to reduce any swelling associated with overuse or aggravation of a previous injury. Nonsteroidal anti-inflammatory medications will also reduce swelling and provide some analgesia.Neutral splinting provides support for the wrist and may help to prevent aggravating maneuvers.Injection of a steroid and local anesthetic mixture into the wrist may provide some temporary relief of symptoms and decrease swelling.An intra-articular injection may also help differentiate intra- and extra-articular disorders.A combination of hand therapy modalities (ie, ultrasound, iontophoresis) and patient education may alleviate some symptoms.
SURGICAL MANAGEMENT
Surgical treatment of ulnar impaction syndrome is indicated for patients who fail to respond to conservative modalities or those who cannot avoid aggravating maneuvers.Patients undergoing ulnar shortening osteotomy must be good surgical candidates, with a high likelihood of healing the osteotomy site.Otherwise, an alternative surgical procedure, such as a wafer resection osteotomy, should be considered.Wrist arthroscopy is frequently used to document physical findings consistent with ulnar impaction syndrome before performing a shortening osteotomy, especially in cases of diagnostic uncertainty even after nonoperative management and injections discussed earlier. Commercial Devices for Ulnar Shortening Osteotomy P.1049Plates and jigs to assist with ulnar osteotomy are commercially available.15 These offer features such as low-profile plate design, locking screws, simplicity of use, decreased surgical time, and improved accuracy of the osteotomy cuts.The surgeon must consider whether the potential advantages of these systems justify the additional expense.22
PREOPERATIVE PLANNING
Neutral rotation posteroanterior and lateral radiographs of both wrists demonstrate ulnar variance and the morphology of the DRUJ, helping to determine the degree of shortening required to unload the joint and still provide a congruent articulation.In principle, a long ulna should be shortened to neutral or 1 mm of negative variance. If there is ulnar neutral variance as a baseline, 2 mm of bone should be removed.8Care must be taken to prevent excessive shortening of the ulna, as this has the potential to increase pressures across the DRUJ articular surface12 and can lead to limitation of forearm rotation.The absolute amount of possible shortening is limited by the marginal ligaments of an intact TFCC. This is reportedly 15 mm in the setting of posttraumatic ulnar impaction syndrome.7DRUJ anomalies, congenital disorders, or arthritis should be ruled out.DRUJ stability is best assessed with examination under anesthesia.
POSITIONING
Preoperative antibiotics with a coverage spectrum for skin flora are given intravenously about 30 minutes before the skin incision.The patient is positioned supine on the operating table with the upper extremity on an arm board.A single-bladder brachial tourniquet is placed over Webril in the upper brachial region and the arm is prepared and draped to the midbrachial level.Extremity exsanguination is achieved with an elastic bandage wrap from the distal fingertips to midbrachial region, and then the tourniquet is inflated to about 250 mm Hg (the pressure may have to be increased in hypertensive patients).Unobstructed access to the elbow during the procedure is crucial to accurately evaluate pronation and supination.Intraoperative fluoroscopy helps the surgeon to discern the degree of correction in ulnar variance after the osteotomy.
APPROACH
An 8- to 10-cm midaxial incision is made over the distal third of the ulnar diaphysis, ending at, or just proximal to, the distal ulnar metaphysis.The interval between the ECU and the flexor carpi ulnaris is developed to expose the ulnar periosteum.Although it is unlikely to be encountered, the location of the dorsal sensory branch of the ulnar nerve must be considered and protected.It takes off from the ulnar nerve an average of 6.4 cm proximal to the distal aspect of the head of the ulna and runs along the subcutaneous border of the ulna for about 5 cm proximal to the pisiform.The dorsal sensory branch typically courses along the medial border of the ulnar head with the forearm supinated and runs in a more palmar position with the forearm pronated.2Circumferential subperiosteal dissection is avoided to prevent injury to the segmental blood supply to the distal ulnar diaphysis, with the exception of a 1-cm zone at the site of the planned osteotomy.26
TECHNIQUES
Authors' Preferred Technique for Ulnar Shortening Osteotomy
Authors’ Preferred Technique for Ulnar Shortening Osteotomy
EXPOSURE
Make an 8- to 10-cm incision over the subcutaneous border of the ulna as previously described (TECH FIG 1A).Elevate the ECU muscle-tendon from the distal dorsal aspect of the ulna to allow sufficient room for a six-or seven-hole AO dynamic compression plate (Synthes LC-DCP, Synthes, Paoli, PA) (TECH FIG 1B).Take care to avoid disrupting the ECU subsheath distally.
OSTEOTOMY



TECH FIG 1 • A. An 8- to 10-cm incision over the subcutaneous border of the ulna. B. Six-hole AO-type dynamic compression plate (DCP) (Synthes). Avoid interfering with the osteotomy when placing the pins by referring to the line drawn at the proposed osteotomy site.Place the pins palmar enough to allow the plate to be securely seated over the dorsal surface of the ulna.
ULNAR OSTEOTOMY


TECH FIG 2 • A. Dorsal compression plate in dorsal position. Proposed osteotomy drawn. The oblique osteotomy angle is about 45 to 60 degrees and it is typically 5 to 6 cm proximal to the ulnar styloid. B. Synthes small distractor apparatus secured along the ulnarmost border with four 2.5-mm threaded Kirschner wires. The kerf (amount of bone resected by the saw blade itself) must be taken into account when planning the site of the second osteotomy cut to determine accurately the total amount of bone removed.Kerf thickness varies based on the specific blade used and can be obtained from the manufacturer.7Make the second parallel osteotomy cut proximal to the first, using a freehand technique, and remove the wafer of bone.Distract the osteotomy site and inspect it to ensure that there are no bony excrescences or residual uncut bone margins, which could interfere with apposition of the fragments.
ALTERNATIVE OSTEOTOMY TECHNIQUE


TECH FIG 3 • Oblique osteotomy created. Using a single-cut technique, reproducible ulnar shortening with precision within 0.2 mm of the exact desired ulnar variance has been reported.A relatively steep angled cut (60 degrees) using stacked blades with a kerf thickness of 4.45 mm can allow for up to 9 mm of shortening with a single cut.Cuts may be made at lesser angles and with lesser kerf thicknesses to allow for lesser degrees of shortening.7
REDUCTION AND STABILIZATION
Dial down the small distractor apparatus to achieve compression at the osteotomy site and bone-to-bone abutment (TECH FIG 4A).A reduction clamp is valuable in guiding and then securing the fragments as compression is applied.Examine the radioulnar relationship under fluoroscopy to ensure adequate correction of ulnar variance and DRUJ congruence.Additional bone resection followed by repeat reduction and compression can be easily achieved if necessary.Again, place the Synthes nonlocking LC-DCP on the dorsum of the ulna, and drill screw holes using a compression or neutral drill guide.With the exception of the interfragmentary lag screw hole, directly over the osteotomy site, all screw holes in the plate are drilled using a 2.5-mm drill followed by a 3.5-mm tap (unless self-tapping screws are used).First, secure the plate with static screws to the fragment with the acute angle (point) on the side away from the plate (palmar in this case, using a dorsal plate).Reduce and secure the osteotomy, and then place compression screws in the other fragment, the one with the acute angle (point) adjacent to the plate.Place the first compression screw in the second hole away from the osteotomy. Fill the remaining more proximal holes with either compression or static screws.As a final step, insert an interfragmentary lag screw through the osteotomy via the hole in the plate directly over the osteotomy (TECH FIG 4B).Pass a 3.5-mm drill only through the near cortex, followed by a 2.5-mm drill through the far cortex. Tap this hole and fill it with a 3.5-mm bone screw.Once proximal and distal stabilization has been achieved, it may be necessary to remove the 2.5-mm pins to fill the remaining screw holes.
COMPLETION




TECH FIG 4 • A. Osteotomy compression. B. An interfragmentary lag screw is placed through the plate.


TECH FIG 5 • A. Posteroanterior (PA) wrist radiograph showing ulnar positive variance. B,C. PA and lateral radiographs after ulnar shortening osteotomy. The interfragmentary lag screw compresses the osteotomy site.
Ulnar Shortening Osteotomy Using an AO Compression Device

TECH FIG 6 • The proposed site of the osteotomy is marked on the ulna. This will allow for compression of the osteotomy when using a DCP and placement of an interfragmentary lag screw. (Courtesy of Thomas R. Hunt III, MD.)


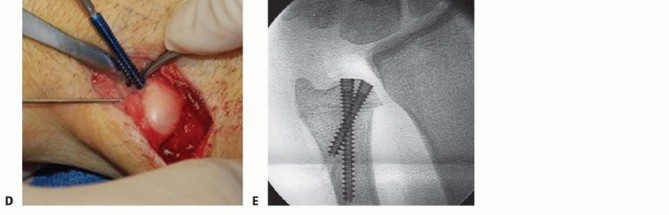
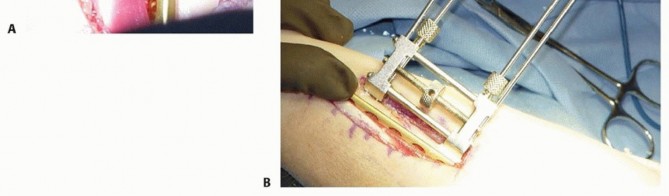
TECH FIG 7 • A. Fluoroscopic image of distal osteotomy, proximal to the sigmoid notch. B. Completion of radial wedge osteotomy. Bone wedge is removed using an osteotome. C. Fluoroscopic image of completed radial wedge osteotomy. D. Placement of headless compression screw over Kirschner wire. E. Radiograph after screw placement showing osteotomy compression. (From Slade JF III, Gillon TJ. Osteochondral shortening osteotomy for the treatment of ulnar impaction syndrome: a new technique. Tech Hand Up Extrem Surg 2007;11:74-82.)Based on preoperative determinations, resect a 3- to 5-mm wafer of bone using a microsagittal saw at the level of the proximal margin of the DRUJ.Leave the distal ulnar articular surface and the TFCC foveal attachments intact (TECH FIG 7A-C).Reduce and compress the osteotomy with a hemostat and a Kirschner wire placed for temporary stabilization.Intraoperative fluoroscopy is used to confirm the adequacy of resection and osteotomy reduction. More bone can be removed if necessary, up to 5 mm total.Excessive bony resection could lead to DRUJ instability or impingement.Thread a cannulated headless compression screw over the previously inserted Kirschner wire while manual compression is maintained (TECH FIG 7D,E).Remove the Kirschner wire and irrigate the wounds.Repair the dorsal capsule with interrupted nonabsorbable sutures.Transpose the extensor digiti quinti tendon out of the fifth compartment as the capsule is repaired.Close the skin incision with a nonabsorbable monofilament suture, and inject all incisions, as well as the wrist, with a local anesthetic.Place the wrist in a bulky dressing with a volar splint.P.1054
PEARLS AND PITFALLS

FIG 4 • Ulnar impaction syndrome in a 73-year-old woman after distal radius fracture nonunion and subsequent collapse. She underwent open reduction and internal fixation of the radius fracture as well as ulnar shortening osteotomy to correct the posttraumatic ulnar positive variance. Severe osteopenia prevented stable fixation of the ulnar osteotomy with the standard plate and necessitated a longer eight-hole DCP.
POSTOPERATIVE CARE
Short-arm below-elbow splint immediately postoperatively Ice and elevation to assist with swelling controlElbow and finger ROM is encouraged immediately. Sutures are removed at 10 to 14 days.A removable splint is applied and protected ROM is started at 6 to 8 weeks, depending on the radiographicappearance of healing.More aggressive ROM exercises are started with hand therapy after 8 to 10 weeks if necessary.
OUTCOMES
Chun and Palmer6 reviewed their series of 30 wrists in 27 patients with an average follow-up of 51 months. Wrists were graded preoperatively and postoperatively according to the Gartland and Werley wrist system. Preoperative wrists graded as poor (28) and fair (2) improved to excellent (24), good (4), fair (1), and poor(1) after ulnar shortening osteotomy. They reported no ulnar nonunions, and complications were rare.Loh et al11 evaluated 23 wrists at a mean follow-up of 33 months. A statistically significant reduction in pain intensity by visual analog scale assessment was seen in 77% of patients. Preoperative versus postoperative change in ROM was not statistically significant, and postoperative wrist function and grip strength also failed to show a statistically significant improvement. Sixty-eight percent of patients complained of local irritation secondary to prominent hardware and 32% eventually had the implant removed.P.1055We do not think that the use of specialized equipment is necessary to achieve accurate cuts and stable fixation for an ulnar shortening osteotomy.Sunil et al24 reported no significant differences in duration of surgery, relief of pain, return to work, postoperative complications, time elapsed between surgery and return to work, or osteotomy union in patients undergoing ulnar shortening osteotomy using the Rayhack device versus those undergoing freehand osteotomies.Braun3 reported a $650 increase in cost with use of the Rayhack device compared to performing the technique freehand.Our preferred technique is simple, it does not require specialized equipment (Synthes Small External Fixation and Small Fragment Bone Fixation Systems); it provides for rotational control of the distal segment; it provides compression of the osteotomy site; and it uses only one size of drill bit, tap, and screw except for the single interfragmentary hole at the osteotomy site.
COMPLICATIONS
Wound infection and osteomyelitis (rare) Hardware fracture (rare with 3.5-mm plate) Hardware failure with very osteopenic boneDelayed union rates in smokers (7.1 months for smokers vs. 4.1 months for nonsmokers)4Painful, prominent hardware: It is generally not necessary to remove hardware, but 3.5-mm compression plates seem to be removable at 6 to 9 months in symptomatic patients with a low risk for refracture whensequential sets of radiographs confirm healing of the osteotomy site.21
REFERENCES
- Berger RA. The ligaments of the wrist. A current overview of anatomy with considerations of their potentialfunctions. Hand Clin 1997;13:63-82.
- Botte MJ, Cohen MS, Lavernia CJ, et al. The dorsal branch of the ulnar nerve: an anatomic study. J Hand Surg Am 1990;15(4):603-607.
- Braun RM. A comparative study of ulnar-shortening osteotomy by the freehand technique versus the Rayhack technique [letter to the editor]. J Hand Surg Am 2006;31(8):1411-1412.
- Chen F, Osterman AL, Mahony K. Smoking and bony union after ulna-shortening osteotomy. Am J Orthop 2001;30:486-489.
- Chen NC, Wolfe SW. Ulna shortening osteotomy using a compression device. J Hand Surg Am 2003;28(1):88-93.
- Chun S, Palmer AK. The ulnar impaction syndrome: follow-up of ulnar shortening osteotomy. J Hand Surg Am 1993;18(1):46-53.
- Fricker R, Pfeiffer KM, Troeger H. Ulnar shortening osteotomy in posttraumatic ulnar impaction syndrome. Arch Orthop Trauma Surg 1996;115:158-161.
- Friedman SL, Palmer AK. The ulnar impaction syndrome. Hand Clin 1991;7:295-310.
- Hammert WC, Williams RB, Greenberg JA. Distal metaphyseal ulnar-shortening osteotomy: surgical technique. J Hand Surg Am 2012;37(5):1071-1077.
- Labosky DA, Waggy CA. Oblique ulnar shortening osteotomy by a single saw cut. J Hand Surg Am 1996;21(1):48-59.
- Loh YC, Van Den Abbeele K, Stanley JK, et al. The results of ulnar shortening for ulnar impaction syndrome. J Hand Surg Br 1999;24(3):316-320.
- Mikić ZD. Age changes in the triangular fibrocartilage of the wrist joint. J Anat 1978;126:367-384.
- Mirza A, Mirza JB, Shin AY, et al. Isolated lunotriquetral ligament tears treated with ulnar shortening osteotomy. J Hand Surg Am 2013;38(8):1492-1497.
- Miura T, Firoozbakhsh K, Cheema T, et al. Dynamic effects of jointleveling procedure on pressure at the distal radioulnar joint. J Hand Surg Am 2005;30(4):711-718.
- Mizuseki T, Tsuge K, Ikuta Y. Precise ulna-shortening osteotomy with a new device. J Hand Surg Am 2001;26(5):931-939.
- Nishiwaki M, Nakamura T, Nakao Y, et al. Ulnar shortening effect on distal radioulnar joint stability: a biomechanical study. J Hand Surg Am 2005;30(4):719-726.
- Nunez FA Jr, Barnwell J, Li Z, et al. Metaphyseal ulnar shortening osteotomy for the treatment of ulnocarpal abutment syndrome using distal ulna hook plate: case series. J Hand Surg Am 2012;37(8):1574-1579.
- Palmer AK, Werner FW. The triangular fibrocartilage complex of the wrist—anatomy and function. J Hand Surg Am 1981;6(2):153-162.
- Palmer AK, Werner FW, Glisson RR, et al. Partial excision of the triangular fibrocartilage complex. J Hand Surg Am 1988;13(3):391-394.
- Papapetropoulos PA, Wartinbee DA, Richard MJ, et al. Management of peripheral triangular fibrocartilage complex tears in the ulnar positive patient: arthroscopic repair versus ulnar shortening osteotomy. J Hand Surg Am 2010;35(10):1607-1613.
- Pomerance J. Plate removal after ulnar-shortening osteotomy. J Hand Surg Am 2005;30(5):949-953.
- Rayhack JM. Ulnar shortening. Tech Hand Up Extrem Surg 2003;7:52-60.
- Slade JF III, Gillon TJ. Osteochondral shortening osteotomy for the treatment of ulnar impaction syndrome: a new technique. Tech Hand Up Extrem Surg 2007;11:74-82.
- Sunil TM, Wolff TW, Scheker LR, et al. A comparative study of ulnarshortening osteotomy by the freehand technique versus the Rayhack technique. J Hand Surg Am 2006;31(2):252-257.
- Tomaino MM. The importance of the pronated grip x-ray view in evaluating ulnar variance. J Hand Surg Am 2000;25(2):352-357.
- Wright TW, Glowczewskie F. Vascular anatomy of the ulna. J Hand Surg Am 1998;23(5):800-804.
- Yin HW, Qui YQ, Shen YD, et al. Arthroscopic distal metaphyseal ulnar shortening osteotomy: a different technique. J Hand Surg Am 2013;38(11):2257-2262.
