DEFINITION
As with any synovial joint, the distal radioulnar joint (DRUJ) can degenerate due to osteoarthritis, inflammatory arthritis, chronic instability, infection, and trauma.4Standard treatments such as partial (“matched resection”) or complete (Darrach procedure) distal ulnar resection have the potential to destabilize the forearm axis and cause painful forearm rotation.The normal compressive muscle forces acting between the radius and ulna help stabilize the DRUJ.1When the distal ulna has been resected and the forearm is rotated under such a compressive load, a palpable grinding between the ulnar stump and the radius may develop; this is referred to asulnarimpingement.6 This may progress from minor irritation to painful erosion of the radius. These patients present with pain on stress loading of the upper extremity, weakness in grip strength, decreasedforearm rotation, and difficulty with lifting.2Ulnar head implant arthroplasty is designed to maintain the DRUJ, thereby avoiding ulnar impingement. An adequate soft tissue envelope repaired over the implant provides stability.The first prosthesis used was a silicone cap designed to provide a soft end to the ulnar stump. These prostheses understandably failed under loading.Newer designs aim to restore the ulnar head using a metallic prosthesis to articulate with the sigmoid notch.
ANATOMY
See Chapters 26, 63, 64, 65, 111, 112, and 115.
PATHOGENESIS
See Chapters 111 and 112.
NATURAL HISTORY
See Chapters 111 and 112.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients who have had an ulnar head resection complain of painful forearm rotation, often associated with instability of the forearm axis, decreased strength, and joint grinding.In addition to recording the range and fluidity of DRUJ motion, the examiner must determine the stability of the joint and the contribution of ulnar impingement to the patient's pain.Radioulnar compression creates radioulnar impingement by external passive compression.The examiner should encircle the patient's distal forearm with his or her hands and apply firm compression. A positive sign is reproduction of the patient's pain.Active radioulnar impingement is reproduced by active muscle contraction, specifically the brachialis.The patient has pain lifting a load of 2 pounds with the forearm in neutral position.Ulnar stump instability results from compromised soft tissue stabilizers of the distal stump, which tends to fall away from the radius as the forearm is rotated.The patient is asked to actively rotate the forearm. Dorsal and palmar subluxation of the ulnar stump is visible.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Standard posteroanterior, lateral, and oblique radiographs of the wristThese x-rays demonstrate scalloping of the ulnar cortex of the radial metaphysis and some corresponding pencilling of the distal ulnar stump.Posteroanterior stress-loaded radiographsMay demonstrate impingement between the radius and ulnaThe patient stands with the involved forearm facing the x-ray tube. The wrist is stress-loaded by asking the patient to hold a 2.2-kg lead cylinder with the shoulder adducted, the elbow flexed to 90 degrees, and the forearm in the position of neutral rotation.The forearm rests on the x-ray cassette and the radiograph is then taken with the beam aligned in the coronal plane, creating a posteroanterior view of the neutral forearm.Radiographs are obtained before and after stress-loading.Computed tomography (CT) scanningIn patients with osteoarthritis of the DRUJ, axial scans are essential for evaluation of the extent of degenerative changes in the ulnar head and the need for total or partial replacement.CT scanning is also essential for evaluation of the sigmoid notch for osteophytes and erosion in patients with painful ulnar head replacement.CT scanning with forearm in pronation and supination is also useful in detecting radioulnar instability if clinical examination is equivocal.
DIFFERENTIAL DIAGNOSIS
In addition to radioulnar impingement, a patient who has pain at the DRUJ after resection of the ulnar head may have pain due to the following conditions:Ulnar neuropathyPainful surgical scar due to sensory nerve injury or scarring Radiocarpal or midcarpal arthritis
NONOPERATIVE MANAGEMENT
Activity modification to minimize forearm rotatory movements will diminish pain.A Russe splint is partially helpful for patients with instability of the distal ulnar stump but is of no help in preventing radioulnar impingement pain.
SURGICAL MANAGEMENT
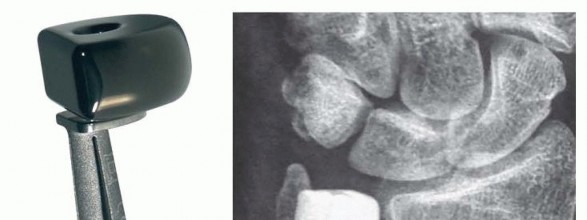
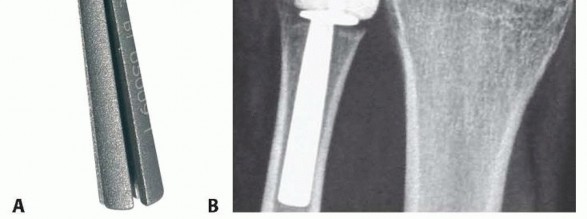
FIG 1 • The Eclypse partial ulnar head replacement (Tornier Surgical Implants, Tornier, Inc., Rodborough Road, FR) consists of an expandable titanium stem with a mobile pyrocarbon spacer (A). When implanted, the prosthesis preserves the ulnar styloid and attachment of the TFCC (B).

FIG 2 • The Stability total ulnar head arthroplasty system (Small Bone Innovations, Inc., Morrisville, PA ) consists of a metal ulnar head component that articulates with a metal-backed polyethylene sigmoid notch. The ulnar head component can be used individually as a hemiarthroplasty.
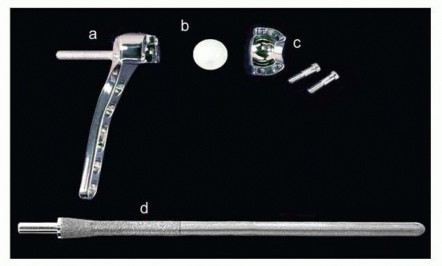
FIG 3 • The Aptis system (Aptis Medical, Louisville, KY) replaces the entire DRUJ with a constrained articulation. The components include (a) radial plate with socket, (b) polyethylene ball, (c) hemisocket with screws, and (d) ulnar stem with peg.The radial component consists of a plate with a polyethylene-lined metal sphere affixed to the interosseous surface of the radius.The ulnar stem has a protruding peg that is captured and rotates within the polyethylene liner. The stem has limited freedom of proximodistal and limited dorsopalmar motion, simulating normal DRUJ mechanics.
PREOPERATIVE PLANNING
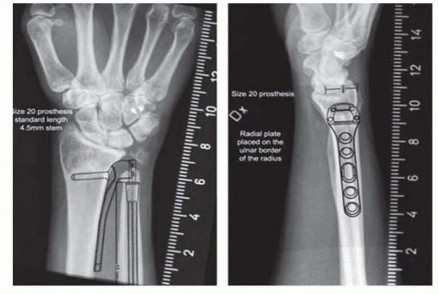
FIG 4 • Preoperative templating for the Aptis system is done in the frontal and lateral planes to determine the appropriate size of implants to be used at surgery.
POSITIONING
Standard positioning and tourniquet application are used.
APPROACH
An incision is made along the ulnar border of the shaft of the distal ulna in line with the ulnar styloid. The interval between the flexor carpi ulnaris (FCU) and extensor carpi ulnaris (ECU) tendons is developed for access to the ulna.A dorsal approach is an alternative and is indicated for partial head replacement. Access to the articular portion of the ulnar head is gained through the floor of the fifth extensor compartment.
TECHNIQUES
PARTIAL ULNAR HEAD REPLACEMENT ARTHROPLASTY


TECH FIG 1 • A,B. Preoperative radiographs of a patient with rheumatoid arthritis and previous radiolunate fusion who treat with First Choice partial ulnar head arthroplasty (Integra LifeSciences, Plainsboro, NJ).(continued)
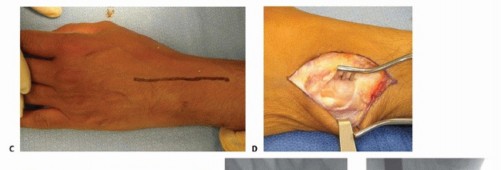

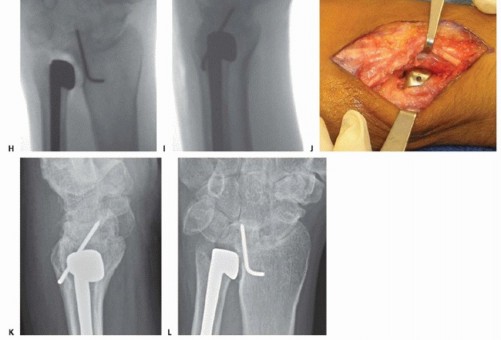
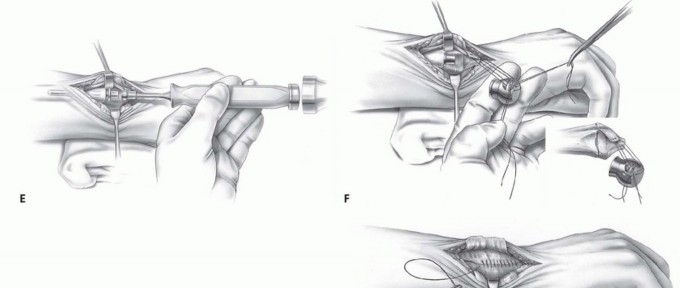
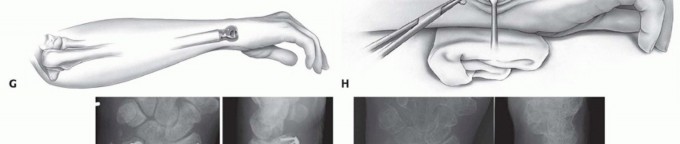
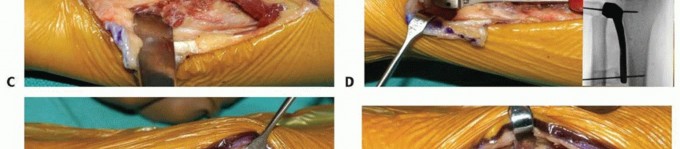
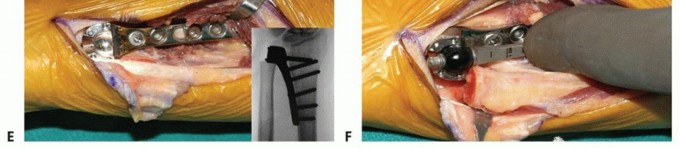
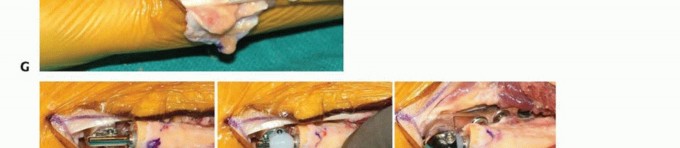
TECH FIG 1 •(continued)C. Longitudinal dorsal incision made to expose ulnar head and elevate ulnar-based flap of capsule. D. Reflected extensor retinaculum with preserved ECU. E. Resected ulnar head measured to match partial ulnar head prosthesis. F,G. Intraoperative Fluoroscan demonstrating partial ulnar head resection. H,I. Intraoperative Fluoroscan images following placement of implant and soft tissue used to stabilize the prosthesis during closure. J. The ulnar medullary canal is reamed. K,L. Postoperative radiographs of partial ulnar head prosthesis.
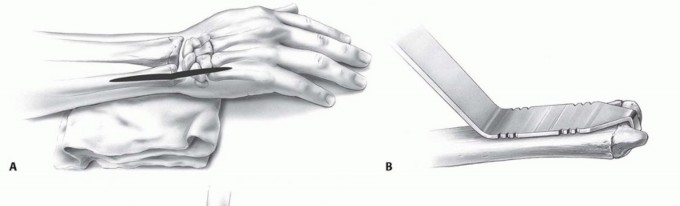
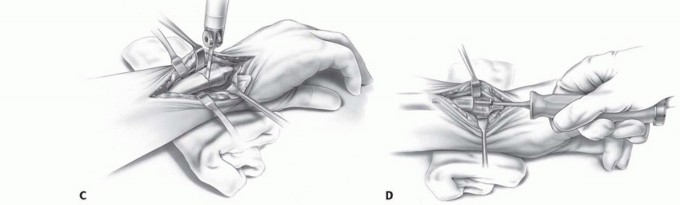
TECH FIG 2 • A. A longitudinal incision is made between the FCU and ECU tendons on the ulnar border of the distal forearm and wrist. B. The cutting guide helps determine the level of resection of the ulnar head. The distal notches are for use with the three head sizes and standard stem, and the proximal notches are for use with a collared stem in cases of previous resection or resorption of the distal ulna. C. An oscillating saw is used to resect the ulnar head at the determined level. D. The ulnar medullary cavity is reamed using broaches.(continued)




TECH FIG 3 • A,B. Preoperative posteroanterior (PA) and oblique radiographs demonstrating previous
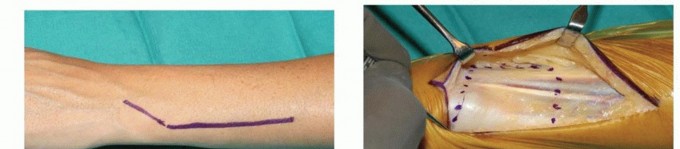
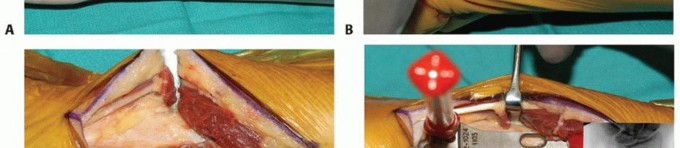
TECH FIG 4 • A. Intraoperative photograph of implantation with the Aptis system. The dorsoulnar skin incision is placed between the fifth and sixth extensor compartments. B. A large ulnar-based flap of retinaculum is raised for later interposition between the ECU tendon and the implant. C. The ulna is displaced volarly with retractors to expose the interosseous surface of the radius and the sigmoid notch.


PEARLS AND PITFALLS
Scarsensitivity or tenderness1. Identify and protect the sensory branch of the ulnar nerve.Intraoperative ▪ Broach the distal ulna with caution. In hard cortical bone, use a drill to enlargefracture of the cavity before impacting a broach in the ulna. the distalulnaIncorrectulnar variance1. Before making the ulnar osteotomy, identify the correct level of the DRUJ usingradiographs or along the distal edge of the sigmoid notch.Loosening ofprosthesis1. Rule out metal allergy, infection.2. Revision options include (1) explanting prosthesis, (2) conversion to interposition arthroplasty with Achilles tendon allograft, (3) conversion to total linked distal DRUJ arthroplasty, or (4) conversion to a one-bone forearm.Instability ofthe prosthesis1. Correct soft tissue insufficiency prior to prosthesis implantation.2. Raise a thick and large flap of soft tissue when exposing the distal ulna. This tissue can be imbricated to stabilize the prosthesis if needed. Alternatively, a distally based strip of the FCU can be wound around the prosthesis to provide volar stability.3. Stability of the implant may not be to demonstrate intraoperatively until the soft tissue envelope is closed over the prosthesis.
POSTOPERATIVE CARE
The forearm is immobilized in neutral rotation and held in a supportive long-arm or Muenster-type splint or cast for 3 weeks.Active range of motion of the wrist and forearm is initiated at 3 weeks.A removable splint is required between therapy sessions for 3 weeks.Therapy is advanced as tolerated after 6 weeks, with strengthening starting only after functional wrist and forearm motion has been obtained.For a patient with rheumatoid arthritis, poor-quality soft tissue coverage, or mild instability intraoperatively, immobilization in supination for up to 6 weeks must be considered.Postoperative radiographs should be obtained at 6 weeks, 6 months, and then yearly.
OUTCOMES
Outcomes vary with the indication and type of prosthesis used.3The pain of radioulnar impingement is relieved in patients with previous excision arthroplasty and stability is restored.9The range of motion of the forearm after prosthetic replacement remains largely unchanged, as it depends on previous scarring.Grip strength recovered depends on the underlying problem, but in patients with severe pain and weakness preoperatively, final grip averages about 60% of the opposite side.Long-term results are limited and variable.One study reported 6-year survival of implant as 83%.7Implant failure was associated with a history of previous surgery, use of an extended collar, lucency greater than 2 mm around the implant stem, and pedestal formation at the tip of the implant.7Continued pain relief and no deterioration or revision requirements were seen in other small, longer term followup studies.10,11
COMPLICATIONS
Immediate- or short-term complicationsInfection and wound breakdown, especially in revision cases with poor soft tissue cover Injury to the dorsal sensory branch of the ulnar nerve, leading to tender neuroma Fracture of the distal ulna during reaming or impaction of the prosthesisDislocation of the prosthesis from the DRUJ postoperatively Long-term complicationsProgressive degeneration of the sigmoid notch Implant looseningTenosynovitis of the ECU tendonErosion of the radius sigmoid notch with pain Ectopic bone formation around the distal ulna Stress shielding and resorption of distal ulna Prosthetic fracture
ACKNOWLEDGMENTS
The authors thank Small Bone Innovations for permission to use their illustrations for demonstration of operative technique, Dr. Luis Scheker for the images of the Aptis system and Dr. Marc Garcia-Elias for the images of the Eclypse prosthesis.
REFERENCES
- Berger RA. Implant arthroplasty for treatment of ulnar head resectionrelated instability. Hand Clin 2013;29:103-111.
- Berger RA, Cooney WP III. Use of an ulnar head endoprosthesis for treatment of an unstable distal ulnar resection: review of mechanics, indications, and surgical technique. Hand Clin 2005;21:603-620.
- Bizimungu R, Dodds S. Objective outcomes following semiconstrained total distal radioulnar joint arthroplasty. J Wrist Surg 2013;2:319-323.
- Conaway DA, Kuhl TL, Adams BD. Comparison of the native ulnar head and a partial ulnar head resurfacing implant. J Hand Surg Am 2009;34(6):1056-1062.P.1035
- Garcia-Elias M. Eclypse: partial ulnar head replacement for isolated DRUJ arthrosis. Tech Hand Upper Extrem Surg 2007;11:121-128.
- Gordon KD, Roth SE, Dunning CE, et al. An anthropometric study of the distal ulna: Implications for implant design. J Hand Surg Am 2002;27(1):57-60.
- Kakar S, Swann P, Perry KI, et al. Functional and radiographic outcomes following distal ulna implant arthroplasty. J Hand Surg Am 2012;37:1364-1371.
- Scheker LR, Babb BA, Killion PE. Distal ulnar prosthetic replacement. Orthop Clin North Am 2001;32:365-376.
- Van Schoonhoven J, Fernandez DL, Bowers WH, et al. Salvage of failed resection arthroplasties of the distal radioulnar joint using a new ulnar head prosthesis. J Hand Surg Am 2000;25(3):438-446.
- Van Schoonhoven J, Muhldorfer-Fodor M, Fernandez DL, et al. Salvage of failed resection arthroplasties of the distal radioulnar joint using an ulnar head prosthesis: long-term results. J Hand Surg Am 2012;37:1372-1380.
- Yen SN, Dion GR, Bowers WH. Ulnar head implant arthroplasty: an intermediate term review of 1 surgeon's experience. Tech Hand Up Extrem Surg 2009;13:160-164.
