INTRODUCTION TO BENIGN LESIONS OF THE HAND AND WRIST
The evaluation and management of benign osseous and soft tissue lesions of the hand require a meticulous understanding of complex regional anatomy, biomechanics, and pathology. While these lesions—ranging from reactive bone formations to metabolic deposits—are non-malignant, their presence within the tightly constrained compartments of the hand frequently leads to significant functional impairment. Mechanical impingement on extensor mechanisms, compression of neurovascular bundles, and severe inflammatory cascades are common clinical presentations.
This comprehensive guide details the pathophysiology, clinical evaluation, and precise surgical management of specific benign entities: Turret exostosis, reactive calcinosis, and the carpometacarpal (CMC) boss, alongside critical considerations for peripheral nerve hypertrophies encountered during surgical exploration.
TURRET EXOSTOSIS
Pathophysiology and Clinical Presentation
A turret exostosis is a smooth, dome-shaped, extracortical mass of mature bone that typically develops beneath the extensor apparatus on the dorsal aspect of the middle or proximal phalanx of a digit.
The etiology is almost exclusively traumatic. A direct blow to the dorsum of the phalanx results in a subperiosteal hematoma. If the hematoma fails to resorb, it undergoes organization and subsequent endochondral ossification, forming a rigid osseous prominence. Clinically, patients present with a firm, painful dorsal mass that restricts the excursion of the extensor mechanism, leading to a localized extension lag or pain during active flexion as the extensor hood is stretched over the exostosis.
Clinical Pearl:
Turret exostosis must be differentiated from an osteochondroma. Unlike an osteochondroma, a turret exostosis does not possess a cartilage cap and does not exhibit continuity with the medullary canal of the underlying phalanx on radiographic evaluation.
Surgical Management: Excision Technique
Surgical excision is indicated when the exostosis causes persistent pain, limits the range of motion, or threatens the integrity of the overlying extensor tendon.
Positioning and Preparation:
The patient is positioned supine with the arm extended on a hand table. A well-padded proximal tourniquet is applied, and the limb is exsanguinated to ensure a bloodless surgical field. Loupe magnification is highly recommended.
Surgical Approach:
1. Incision: A midlateral incision is utilized rather than a direct dorsal approach. A direct dorsal incision places the surgical scar directly over the extensor tendon, significantly increasing the risk of postoperative adhesions and restricted tendon gliding.
2. Exposure: The skin and subcutaneous tissues are carefully elevated. The extensor apparatus is identified and gently retracted dorsally and contralaterally to expose the underlying pathology.
3. Periosteal Dissection: The periosteum is incised laterally along the border of the exostosis. It is meticulously elevated from the underlying abnormal bone.
4. Excision: Using a fine rongeur or a sharp micro-osteotome, the dome-shaped exostosis is resected flush with the normal diaphyseal cortex of the phalanx.
Surgical Warning:
Extreme care must be taken not to tear or resect the dorsal periosteum. Preserving a smooth, continuous periosteal surface over the resection site is critical; it provides a frictionless gliding layer for the extensor apparatus. Failure to preserve this layer will result in severe tenodesis to the raw cancellous bone bed.
- Closure: The periosteal sleeve is meticulously closed over the defect using fine absorbable sutures (e.g., 5-0 Vicryl). The extensor mechanism is allowed to fall back into its anatomic position, and the skin is closed routinely.
Postoperative Protocol
The digit is immobilized in a bulky soft dressing with a dorsal blocking splint for 3 to 5 days to allow for initial wound healing. Early active range of motion (AROM) is initiated by postoperative day 5 under the guidance of a hand therapist to prevent extensor tendon adhesions.
PERIPHERAL NERVE HYPERTROPHY: DÉJÉRINE-SOTTAS AND LIPOFIBROMATOUS HAMARTOMA
During the surgical exploration of undiagnosed volar or palmar hand masses, the surgeon may unexpectedly encounter severe enlargement of the median nerve. The raw clinical picture of a space-occupying lesion in the hand can occasionally be caused by infiltration of the nerve by various fatty tumors or hypertrophic neuropathies.
Pathology and Presentation
Conditions such as Déjérine-Sottas disease (a severe, early-onset hereditary motor and sensory neuropathy) or lipofibromatous hamartoma (fibrofatty infiltration of the epineurium and perineurium) present with massive, fusiform enlargement of the median nerve. These lesions are frequently associated with macrodactyly (nerve-territory overgrowth) and can cause severe compressive neuropathy within the carpal tunnel.
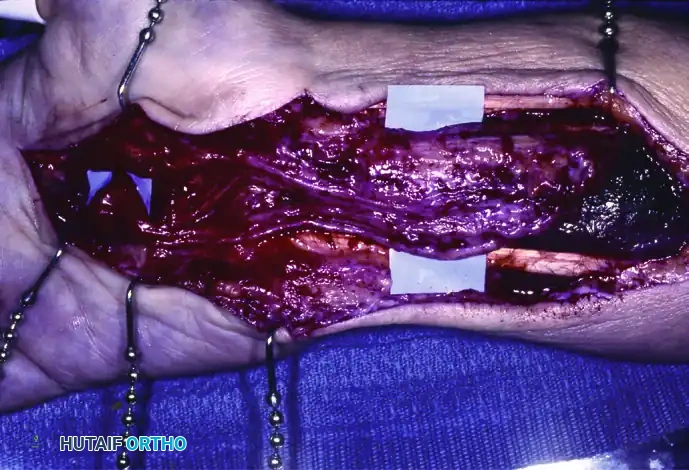
Extensive involvement of the median nerve coursing from the distal third of the forearm into the palm, demonstrating massive fibrofatty hypertrophy.
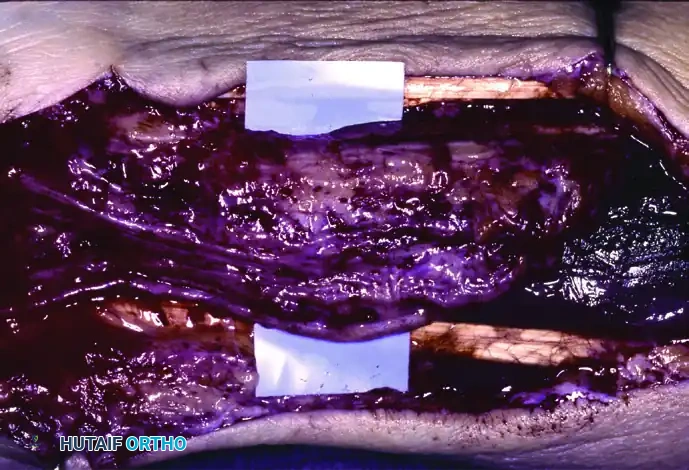
A closer intraoperative view of severe enlargement of the median nerve. Note the loss of normal fascicular architecture due to infiltration.
Surgical Considerations
When an enlarged, infiltrated median nerve is encountered, the surgical strategy must immediately shift from excision to decompression.
Surgical Warning:
An infiltrated, hypertrophic median nerve cannot be excised without resecting the nerve itself, which definitely should not be done. Resection results in catastrophic loss of motor function (thenar intrinsic muscles) and devastating sensory loss to the radial three-and-a-half digits.
Management Strategy:
1. Decompression: Dividing the transverse carpal ligament (carpal tunnel release) is the primary surgical intervention. This helps to relieve pain, restores microvascular perfusion to the compressed nerve, and occasionally decreases the size of the nerve distally by relieving the mechanical bottleneck.
2. Observation: The swelling and localized pain occasionally subside spontaneously after decompressive surgery.
3. Biopsy (Proceed with Caution): If a biopsy is deemed absolutely necessary to rule out malignancy, it must be limited to the epineurium or a clinically silent, non-functional fascicle under high-power microscopic magnification.
CALCINOSIS AND CALCIUM DEPOSITION DISORDERS
Etiology and Pathogenesis
The exact etiology of reactive calcium deposits in the hand remains unknown. The prevailing theory suggests that they result from localized connective tissue degeneration or microtrauma, which lowers the local tissue pH and creates a nidus for secondary amorphous calcium deposition. Approximately one-third of patients report a distinct history of antecedent trauma.
While calcium deposits occur much less frequently in the hand compared to the shoulder (calcific tendinitis of the rotator cuff) or hip, their presentation in the hand is significantly more alarming due to the tight fascial compartments.
Clinical Presentation
Patients typically present with an acute onset of severe pain, localized tenderness, dramatic swelling, and erythema.
Clinical Pearl:
The intense inflammatory reaction surrounding acute calcinosis in the hand can easily be confused with an acute bacterial infection, such as septic tenosynovitis, cellulitis, or a localized abscess. A high index of suspicion and careful radiographic evaluation are required to avoid unnecessary surgical incision and drainage.
Radiographic Evaluation
Radiographs taken very early in the onset of symptoms may show only a faint, ill-defined "light cloud" in the soft tissues, suggesting an early deposit. As the lesion matures, the calcium consolidates, and the radiographic picture becomes definitively diagnostic, showing a dense, homogenous, amorphous radiopacity.

Radiograph demonstrating a dense calcium deposit near the flexor carpi ulnaris (FCU) insertion into the pisiform, the most common site of occurrence in the wrist.
Common Anatomical Sites:
* Flexor Carpi Ulnaris (FCU): Deposits near the FCU insertion into the pisiform are the most common, accounting for about two-thirds of reported wrist cases.
* Collateral Ligaments: Frequently seen in the collateral ligaments of the fingers and thumb.
* Tendons: Extensor tendons of the thumb and the tendons of the intrinsic hand muscles.
* Rarely, multiple deposits may present simultaneously.
Conservative and Surgical Management
Conservative Treatment:
The vast majority of calcific deposits are self-limiting and will undergo spontaneous rupture into adjacent soft tissues followed by gradual macrophage-mediated absorption.
* Immobilization: Rest and splinting of the affected joint.
* Therapy: Application of local heat.
* Injections: Injection of a local anesthetic (e.g., Lidocaine) with or without a corticosteroid preparation provides rapid symptomatic relief and reduces the inflammatory cascade.
* Aspiration: If the deposit is in the acute, "toothpaste-like" phase, direct aspiration with a large-bore needle (18-gauge) may decompress the lesion and give immediate relief.
Surgical Treatment:
Surgical excision is strictly reserved for large, chronic deposits that cause persistent mechanical block, intractable pain, or threaten to erode through the overlying skin. The surgical approach is dictated by the anatomical location, ensuring the protection of adjacent neurovascular structures.
Calcinosis Circumscripta
It is vital to differentiate isolated reactive calcinosis from Calcinosis Circumscripta. The latter is a systemic manifestation strongly associated with collagen vascular and autoimmune diseases. It is frequently seen in patients with systemic lupus erythematosus (SLE), rheumatoid arthritis, dermatomyositis, and especially scleroderma (often as part of the CREST syndrome: Calcinosis, Raynaud's, Esophageal dysmotility, Sclerodactyly, Telangiectasia). Management of calcinosis circumscripta is primarily medical, targeting the underlying systemic disease.
CARPOMETACARPAL (CMC) BOSS
Anatomy and Biomechanics
A carpometacarpal (CMC) boss, or carpe bossu, is a fixed, benign dorsal osteophyte protuberance located at the mating surfaces of the CMC joints. It most commonly affects the quadrangular articulation involving the bases of the second and third metacarpals and their respective articulations with the trapezoid and capitate.
Clinical Evaluation
Patients typically present with a hard, bony prominence on the dorsal aspect of the wrist.
* Cosmesis: Most lesions are relatively asymptomatic and constitute only a cosmetic concern.
* Mechanical Pain: The extensor tendons—specifically the extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB)—occasionally sublux over the dome of the osteophyte during wrist motion, causing a painful snapping sensation or tenosynovitis.
* Impingement: Pain can also be elicited by direct local pressure over the lesion or by forced wrist extension, which compresses the dorsal capsule against the osteophyte.
Imaging:
Standard posteroanterior and lateral radiographs may obscure the lesion due to bony overlap. A specific tangential radiograph (the carpal boss view)—taken with the wrist in 30 degrees of supination and slight ulnar deviation—is required to profile the dorsal osteophyte. This radiographic feature definitively distinguishes a CMC boss from a dorsal carpal ganglion cyst, though the two conditions can occasionally coexist.
Surgical Management
Surgical excision is indicated for patients with refractory pain, severe tendon snapping, or functional limitation that has failed conservative management (splinting, NSAIDs, corticosteroid injections).
Surgical Technique:
1. Incision: A transverse or longitudinal incision is made directly over the prominence.
2. Dissection: The extensor retinaculum is incised, and the extensor tendons (ECRL, ECRB, and Extensor Digitorum Communis) are identified and carefully retracted.
3. Tendon Protection:
Surgical Warning:
Meticulous care must be taken to identify and protect the insertions of the radial wrist extensor tendons. The ECRL inserts into the base of the second metacarpal, and the ECRB inserts into the base of the third metacarpal. Iatrogenic detachment of these tendons will result in severe wrist extension weakness.
4. Excision: The dorsal capsule is incised longitudinally. The osteophyte is exposed subperiosteally. Using a sharp osteotome or a high-speed burr, the boss is resected flush with the normal dorsal cortex of the metacarpals and carpal bones.
5. Joint Inspection: The CMC joint space should be inspected. If a ganglion stalk is present, it must be excised.
Management of Recurrence:
Recurrence after simple excision is a significant clinical concern, often resulting from incomplete resection or ongoing micromotion and degenerative changes at the CMC joint. If a patient presents with a painful recurrence after a primary excision, repeat simple excision is generally contraindicated. Repeat surgery for recurrence warrants a formal carpometacarpal joint arthrodesis (fusion) of the affected 2nd or 3rd CMC joint to eliminate the motion driving the osteophyte formation.
Postoperative Care
Following simple excision, the wrist is immobilized in a volar splint in slight extension for 2 weeks to allow capsular healing. Gradual range of motion exercises are then initiated. If a CMC arthrodesis is performed, rigid immobilization or internal fixation (using plates or K-wires) is maintained for 6 to 8 weeks until radiographic union is confirmed.
