INTRODUCTION TO SOFT TISSUE INJURY MANAGEMENT
In the realm of operative orthopaedics, the ultimate functional outcome of any major musculoskeletal trauma is inextricably linked to the viability and meticulous management of the surrounding soft tissue envelope. The historical paradigm of prioritizing skeletal fixation over soft tissue preservation has long been abandoned in favor of an integrated, ortho-plastic approach.
Initial treatment of open wounds and severe closed soft tissue injuries must begin immediately at the scene of the accident or upon arrival at the emergency department, well before transport to a definitive surgical facility. The foundational tenets of this initial phase include direct pressure over the wound to control hemorrhage, rigid splinting of fractures to prevent secondary soft tissue trauma, and the immediate placement of sterile dressings to mitigate nosocomial contamination.
Clinical Pearl: Rapid transport to a definitive trauma center is critical; however, expedited transport should never supersede the fundamental principles of limb stabilization. Unsplinted fractures continue to inflict internal shearing forces, exacerbating muscle crush, disrupting microvascular networks, and significantly increasing the incidence of deep infection, skin necrosis, and subsequent wound breakdown.
PATHOPHYSIOLOGY OF THE MOREL-LAVALLÉE LESION
A Morel-Lavallée lesion is a severe, closed degloving injury characterized by the traumatic separation of the skin and subcutaneous tissue from the underlying deep fascia. This separation is driven by high-energy shearing forces, most commonly encountered in pelvic ring disruptions, acetabular fractures, and severe blunt trauma to the thigh.
When the hypodermis is violently sheared from the fascia, the trans-fascial perforating vessels and lymphatic channels are abruptly severed. This creates a dead space that rapidly fills with a mixture of blood, lymph, and liquefied necrotic fat, forming a highly expansile hemolymphatic collection. If left untreated, the peripheral margins of this collection undergo an inflammatory response, eventually forming a dense, fibrous pseudocapsule that prevents spontaneous resorption of the fluid, leading to chronic seromas, secondary infection, and massive skin necrosis.
Clinical Evaluation and Presentation
Patients typically present with a fluctuant, highly compressible mass, often accompanied by skin hypermobility, ecchymosis, and decreased cutaneous sensation over the affected area due to the avulsion of cutaneous nerve branches.

FIGURE 53-11A: Clinical appearance of a large Morel-Lavallée lesion in the anterior thigh following a high-energy pelvic fracture. Note the massive swelling and loss of normal topographic landmarks.

FIGURE 53-11B: Posterior view of the same patient, demonstrating the circumferential nature of the fluid collection and the dependent pooling of the hemolymphatic fluid.

FIGURE 53-11C: Appearance of a large, neglected Morel-Lavallée lesion in the buttock. The delayed presentation has led to profound skin necrosis and full-thickness eschar formation, necessitating extensive open débridement.
Vascular Anatomy and the Risk of Skin Necrosis
The integument of the thigh and pelvic region is particularly vulnerable to ischemic necrosis following a degloving injury due to the erratic and delicate course of its blood supply. The cutaneous perfusion relies heavily on musculocutaneous and septocutaneous perforators that traverse the deep fascia.
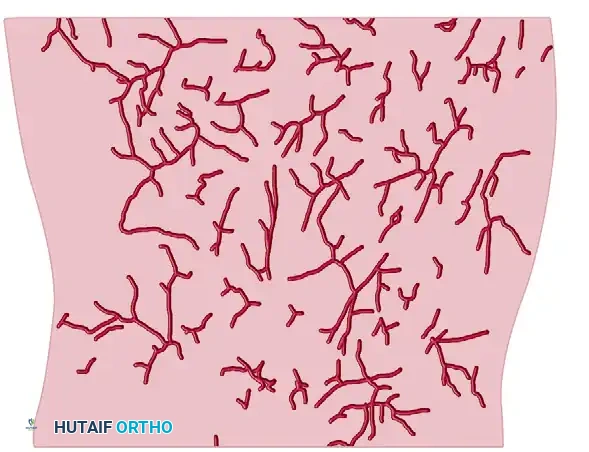
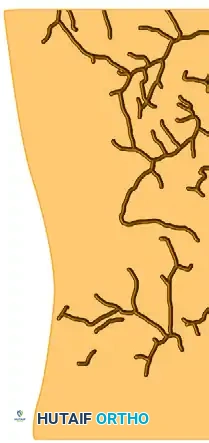

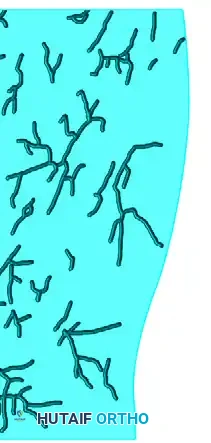
FIGURE 53-12: Tracings of the thigh vessels (internal diameter ≥ 0.25 mm) demonstrating the anterolateral (AL), posterior (P), and anteromedial (AM) vascular networks. The erratic distribution of these perforators highlights why shearing forces so easily devascularize the overlying skin flap.
Surgical Warning: Traditional open surgical approaches to drain a Morel-Lavallée lesion carry a profound risk of further devascularizing the already compromised skin flap. Extensive incisions disrupt the few remaining intact collateral vessels, frequently converting a closed degloving injury into a massive open wound with full-thickness tissue loss.
SURGICAL MANAGEMENT OF MOREL-LAVALLÉE LESIONS
The management of Morel-Lavallée lesions has evolved significantly. While we have historical experience with simple percutaneous aspiration, this method is fraught with unacceptably high recurrence rates because it fails to address the necrotic fat and the ongoing lymphatic leak within the cavity.
Currently, these lesions should be treated aggressively, ideally at the time of internal fixation of the underlying fracture, or within the first few days of admission.
The Percutaneous Drainage Technique (Tseng and Tornetta)
More recently, Tseng and Tornetta described excellent clinical results in 19 patients with Morel-Lavallée lesions utilizing a targeted percutaneous drainage technique performed within 3 days of admission. This minimally invasive approach effectively evacuates the hematoma and débrides the cavity while preserving the fragile cutaneous blood supply.
Step-by-Step Surgical Technique:
1. Incision and Access: Small (1-2 cm) incisions are made at the most dependent portions of the fluctuant collection.
2. Evacuation: A rigid suction tip is introduced to evacuate the gross hematoma and map the full anatomical extent of the cavity.
3. Mechanical Débridement: A sterile surgical brush (often referred to as a "bottle brush") is introduced through the percutaneous portals. The brush is vigorously passed throughout the cavity to mechanically disrupt the pseudocapsule and débride the loose, necrotic, liquefied fat that acts as a nidus for infection.
4. Irrigation: Copious low-pressure irrigation with normal saline is performed until the effluent is entirely clear.
5. Drain Placement: Closed suction drains are placed through the incisions and tunneled throughout the extent of the cavity.
6. Compression: A robust, uniform compression bandage is applied externally to obliterate the dead space and encourage the skin flap to adhere to the underlying fascia.

FIGURE 53-13A: Percutaneous drainage of a Morel-Lavallée lesion. The extent of the lesion is carefully determined and evacuated using a rigid suction tip.

FIGURE 53-13B: A sterile surgical brush is utilized percutaneously to aggressively débride loose, necrotic fat and disrupt the fibrinous cavity lining.
Postoperative Protocol and Outcomes:
In the Tseng and Tornetta series, which included six acetabular surgeries and two pelvic ring surgeries, there was a mandatory delay of at least 24 hours before the drains were removed to ensure output had ceased. Only three of the 19 patients had a positive bacterial culture at the time of drainage, and only one required subsequent open exploration for persistent drainage. Notably, there were zero deep infections at the 6-month follow-up, underscoring the efficacy and safety of this percutaneous approach.
Open Débridement for Refractory Lesions
In cases of delayed presentation where a thick, mature pseudocapsule has formed, or where frank skin necrosis has already occurred, percutaneous methods are contraindicated. These patients require formal open débridement.

FIGURE 53-11D: Operative exposure of a chronic Morel-Lavallée lesion. The image demonstrates the profound depth of the lesion and the necessity for radical excision of the fibrotic pseudocapsule and nonviable tissue to achieve a healthy, bleeding wound bed.
PRINCIPLES OF ORTHOPAEDIC DÉBRIDEMENT
When managing open fractures or severe soft tissue trauma requiring surgical exploration, meticulous débridement is the cornerstone of preventing deep infection and osteomyelitis. Individual patient characteristics—such as peripheral vascular disease, diabetes mellitus, and smoking status—must be carefully considered when determining the exact extent of débridement necessary, as these factors severely compromise wound healing potential.
Skin Débridement
The primary objective of skin débridement is to excise all crushed, contaminated, and ischemic tissue. Generally, the skin margins should be sharply débrided until a healthy, bleeding edge is encountered.
Surgical Warning: Skin débridement should never be performed under tourniquet control. The application of a tourniquet completely obscures capillary bleeding, making it impossible for the surgeon to accurately assess the true viability and perfusion of the skin edges.
Muscle Débridement: The Four "C's"
Muscle tissue is highly sensitive to ischemia and crush injury. Retained necrotic muscle serves as an ideal culture medium for catastrophic anaerobic infections, including clostridial myonecrosis (gas gangrene). Muscle débridement must be radical, removing all nonviable tissue that is noncontractile or grossly contaminated.
During surgical exploration, the viability of skeletal muscle is strictly evaluated using the universally recognized Four "C's":
- Consistency: Normal muscle is firm, resilient, and rebounds when grasped with forceps. Nonviable muscle is friable, mushy, and often described as having a "waxy" or "stewed" texture that falls apart under minimal tension.
- Color: Healthy muscle exhibits a bright, beefy red appearance. Muscle that is dark, purple, pale, or gray is ischemic and must be excised.
- Contractility: This is the most reliable indicator of muscle viability. Normal muscle will visibly twitch and contract when mechanically pinched with forceps or stimulated with a low-voltage electrocautery device (Bovie). Lack of contractility mandates excision.
- Circulation: Healthy muscle will bleed briskly when incised. A lack of punctate capillary bleeding upon sharp dissection indicates irreversible ischemia.
Management of Tendons and Fascia
The management of tendinous structures requires a nuanced approach. Completely severed tendon ends that are highly contaminated, frayed, and crushed may require sharp excision to prevent deep infection. However, this becomes a much more questionable practice if the overall musculotendinous unit remains intact and functional.
Whenever possible, removal of surface contamination with preservation of the tendon itself should be attempted through meticulous mechanical cleaning and low-pressure irrigation.
Clinical Pearl: Tendons are inherently avascular structures that rely heavily on their surrounding paratenon and ambient moisture for survival. Care must be taken to maintain continuous moisture around such structures during prolonged surgeries. Once a tendon becomes desiccated (dried out), it undergoes irreversible necrosis and subsequent excision will be absolutely necessary.
To prevent desiccation of these delicate tissues during staged reconstructions, early flap placement, the use of saline-soaked gauze, or the application of a sealed Negative Pressure Wound Therapy (NPWT) dressing is highly recommended. These modalities maintain a physiologic, moist environment, promote angiogenesis, and protect the preserved tendinous and neurovascular structures until definitive soft tissue coverage can be achieved.
