DEFINITION
Enchondromas are benign cartilaginous neoplasms that are commonly seen in the medullary cavity of phalanges and metacarpals and less commonly in the radius and ulna. Enchondroma is the most common neoplasm of bone arising in the hand.Unicameral bone cysts are benign endothelial-lined fluid-filled cavities arising in metaphyseal bone; they are occasionally seen in the distal radius and rarely seen in the hand.Giant cell tumor of bone is an uncommon neoplasm of bone, which is locally aggressive and can metastasize. Although its histology suggests a benign process, is behaves as a lowgrade malignancy.
ANATOMY

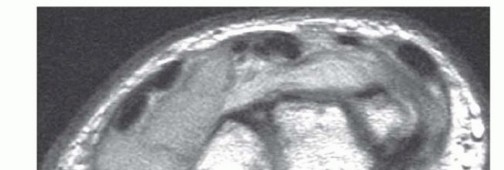
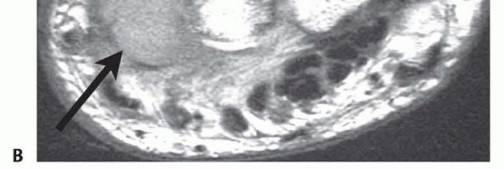
FIG 1 • A. Enchondroma of the proximal phalanx. B. Unicameral bone cyst of the distal radius. C. Giant cell tumor of the distal radius.
PATHOGENESIS
The pathogenesis of enchondroma, unicameral bone cyst, and giant cell tumor of bone is uncertain. Enchondroma and unicameral bone cysts may be associated with bone development and growth.Enchondroma, unicameral bone cyst, and giant cell tumor of bone can weaken the bone and predispose the patient to pathologic fracture.
NATURAL HISTORY
Enchondromas are most commonly identified incidentally during unrelated evaluation. They also can present after pathologic fracture. On occasion, a patient may complain of painful swelling in the bone.Enchondromas found incidentally and not causing considerable mechanical weakness may be observed if typical radiographic findings are seen.Enchondromas causing substantial fracture risk and those presenting after pathologic fracture can be treated surgically with a low risk of recurrence.7Enchondromas can extremely rarely transform to chondrosarcomas.Unicameral bone cysts are most commonly seen during adolescence or childhood. They are most commonly identified after pathologic fracture. Proximal humerus lesions may be seen.Unicameral bone cysts with a low risk of fracture may be observed with activity modification.Unicameral bone cysts causing substantial weakness and fracture risk may be treated with surgery or injection.Suspected unicameral bone cysts in the bones of the hand are sufficiently rare that strong consideration should be given to biopsy when this lesion is suspected.P.1331Giant cell tumor of bone is locally aggressive. Patients may present with pain and swelling or after pathologic fracture.Giant cell tumor of bone metastasizes 2% to 10% of the time, with metastasis more frequently seen with distal radius and hand lesions.1,2,4,5,6 Metastasis most frequently occurs concurrent with or after a local recurrence.Patients with giant cell tumor of bone require systemic staging, treatment, and long-term surveillance, as recurrence may be seen late.
PATIENT HISTORY AND PHYSICAL FINDINGS
Enchondroma is most often an incidental finding and is asymptomatic. Pain and deformity can be seen after pathologic fracture. On occasion, there will be bone distention and tenderness with palpation.Unicameral bone cysts are most commonly seen after pathologic fracture. On occasion, there will be swelling and tenderness.Giant cell tumor of bone may cause swelling, pain, tenderness, and a sense of weakness. Loss of range of motion is common, as these lesions are typically periarticular. Pathologic fracture may be seen.
IMAGING AND OTHER DIAGNOSTIC STUDIES

DIFFERENTIAL DIAGNOSIS
Enchondroma Chondromyxoid fibroma Chondrosarcoma Unicameral bone cyst InfectionAneurysmal bone cyst Giant cell tumor of bonePrimary malignant bone neoplasms Acrometastasis
NONOPERATIVE MANAGEMENT
Enchondromas and unicameral bone cysts may be observed provided radiographic assessment is diagnostic or the differential diagnoses are limited to benign, nonaggressive lesions with an indolent natural history. The assessment of risk of pathologic fracture is paramount. Lesions with a substantial risk of pathologic fracture in the context of the patient's activity level are best treated operatively.The rare risk of malignant degeneration of enchondromas should be considered and discussed with the patient.Suspected giant cell tumor of bone requires biopsy. Rarely, these can be treated with radiation alone; however, this approach is the exception and should not be considered first-line treatment. Radiation is associated with a risk of subsequent true malignant degeneration to a highly malignant giant cell tumor of bone.
SURGICAL MANAGEMENT
All suspected giant cell tumors of bone and those enchondromas and unicameral bone cysts with a high risk of fracture are best treated surgically.
PREOPERATIVE PLANNING
The radiographic extent of disease must be assessed.The approach will vary depending on the anatomic location. Bone graft source (autologous or allograft) must be considered.Precautions to prevent donor site cross-contamination must be considered and reviewed with the operating room team.The surgeon must determine the anticipated need for frozen section and discuss this with the pathologist and review radiographs before any anticipated frozen section.The surgeon must secure and confirm the availability of any necessary grafting materials, instruments, implants, or adjuvants (ie, liquid nitrogen).P.1332The surgeon must confirm the availability of intraoperative imaging. Radiographs will give better resolutionthan fluoroscopy.
POSITIONING
Surgery is typically done in the supine position with the arm extended on a radiolucent arm board. Proximal humerus lesions may be approached in a modified beach-chair position.
APPROACH
Phalanx lesions may be approached from the dorsal or lateral approach. Metacarpal lesions are best approached dorsally in most instances.Carpal lesions are usually best approached dorsally.Distal radius lesions may be approached at the tubercle of Lister or at the interval between the radial border of the pronator quadratus and the first dorsal compartment, proximal to the radial styloid.Ulnar lesions are usually best approached dorsally or ulnarly.Proximal humerus lesions are best approached just lateral to the deltopectoral interval.Biopsy must always take into consideration the potential for malignancy. It must be done in a way that does not compromise the potential need for a subsequent limb-sparing procedure.
TECHNIQUE
Curettage and Excision of Proximal Phalangeal Enchondroma
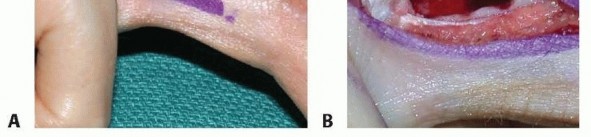
The midaxial approach from the ulnar side is preferred whenever possible (TECH FIG 1A).
After making the incision under tourniquet control, identify the lateral band and retract it dorsally.
Curettage and Excision of Proximal Phalangeal Enchondroma TECH FIG 1 • A. Midaxial approach to proximal phalanx enchondroma. B. The lateral band is retracted and a bone window is created before curettage.



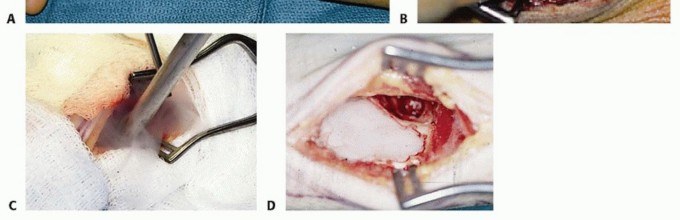
TECH FIG 3 • A. Dorsal exposure of the distal radius and ulna with transection of the radius and ulna proximally. B. The radius and ulna are everted into the dorsal wound to allow palmar exposure and dissection of palmar soft tissues. C. The resection specimen, demonstrating the midcarpal articulation of the proximal carpal row. D. Reconstruction is by means of an osteoseptocutaneous vascularized fibula graft for intercalary arthrodesis. A spanning 3.5-mm compression plate is used for fixation.
PEARLS AND PITFALLS




POSTOPERATIVE CARE
Phalanx or metacarpal enchondromaBulky protective dressings are applied and range of motion is initiated at the first dressing change, usually 8 to 10 days postoperatively.Protective splinting is continued for 6 weeks after surgery. High-risk activities are restricted for 12 to 16 weeks.Periodic surveillance continues for 3 to 5 years.Curettage, cryosurgery, and cementation of distal radius giant cell tumor of boneDressings are changed 10 days postoperatively. Sutures are removed and the patient is fitted with a removable splint.Active range-of-motion exercises are initiated. Active-assisted and passive range-of-motion exercises are added at week 6.P.1335Activities are gradually increased, with high-risk activities being restricted for up to 2 years due to cryonecrosis of bone caused by cryosurgery.Wide en bloc extra-articular distal radius resectionPatients are dressed in a bulky compressive dressing, most commonly with a volar splint. Elevation is encouraged for the first 48 hours, and digit range of motion is encouraged.Formal supervised therapy is initiated at the first dressing change, typically 8 to 10 days after surgery.At that time, bandages are removed and sutures can be removed.Most commonly, active and active-assisted range-of-motion exercises are initiated. When not exercising, patients are asked to use a protective splint for an additional month. Activities are progressively increased as soft tissue and bone healing allows.Range-of-motion exercises are initiated no later than 10 days after surgery.Protective splinting continues a total of 6 weeks minimum after intralesional procedures and until bone healing is confirmed after arthrodesis.Sporting activities are typically restricted for 12 to 18 weeks. High-risk activities are avoided for longer periods.Surveillance for local recurrence should continue for 5 years for benign lesions and 10 years for giant cell tumor of bone.
OUTCOMES
Local recurrenceThe local recurrence rate after curettage and bone grafting of enchondromas is about 5%. Whenrecurrence is seen, the question of malignant transformation should be considered.7The local recurrence rate after curettage and bone grafting of giant cell tumor of bone in the distal radius is about 50% and adjuvants such as liquid nitrogen can lower this to about 20%. Intralesional treatment (curettage) is best reserved for lesions without soft tissue extension or extension limited to asingle plane of palmar perforation bound by pronator quadratus (grade 1 and 2 lesions).4,5,6 Wide excision of distal radius lesions is associated with local recurrence rates of less than 10%;however, reconstruction in the form of articular allograft or intercalary arthrodesis results in inferiorfunction, motion, and strength and higher levels of pain.4,5,6,9The local recurrence rate after curettage and bone grafting of giant cell tumor of bones of the hand is about 80%. Isolated curettage without the use of adjuvants cannot be advocated in this setting. There are several successful examples of curettage, cryosurgery, and cementation of giant cell tumor of thesmall bones of the hand. This type of procedure is best done at a tumor referral center.1,2Wide excision or amputation has been advocated for giant cell tumor of bone when it arises in the phalanges or metacarpals. Local recurrence may still be seen, but the rate is probably less than 10%.1,2The local recurrence rate after curettage of enchondromas arising in the hand is about 5%.7The local recurrence rate after wide excision or amputation for giant cell tumor of the bones of the hand is less than 10%.The local recurrence rate after curettage, cryosurgery, and cementation of distal radius giant cell tumor of bone is about 20% to 25% and correlates with soft tissue extension.4,6The local recurrence rate after wide excision of distal radius giant cell tumor of bone is likely less than 10%.8MetastasisBenign giant cell tumor of bone metastasizes in 2% to 8% in general case series.1,2,5 Motion and strengthRange of digit motion is typically excellent after curettage for enchondroma.Range of motion of the wrist may be slightly diminished after curettage of enchondromas in the distal radius.Grip strength is reduced to 60% of normal after wide excision of the distal radius for giant cell tumor with intercalary segmental arthrodesis. Forearm rotation is typically preserved.
COMPLICATIONS
Infection, hematoma, nerve injury, intraoperative fracture, postoperative fracture, nonunion, limited range of motion, and tendon gliding problems may be seen after treatment of enchondroma or giant cell tumor of bone when arising in the upper extremity.Delayed complications include extensor tendon rupture due to prominent residual ulna, nonunion, and fracture after hardware removal.
REFERENCES
- Athanasian EA, Wold LE, Amadio PC. Giant cell tumors of the bones of the hand. J Hand Surg Am 1997;22(1):91-98.
- Averill RA, Smith RJ, Campbell CJ. Giant-cell tumors of the bones of the hand. J Hand Surg Am 1980;5(1):39-50.
- Campanacci M, Laus M, Boriani S. Resection of the distal end of the radius. Ital J Orthop Traumatol 1979;5:145-152.
- Kang L, Manoso MW, Boland PJ, et al. Features of grade 3 giant cell tumors of the distal radius associated with successful intralesional treatment. J Hand Surg Am 2010;35(11):1850-1857.
- O'Donnell RJ, Springfield DS, Motwani HK, et al. Recurrence of giant-cell tumors of the long bones after curettage and packing with cement. J Bone Joint Surg Am 1994;76(12):1827-1833.
- Sheth DS, Healey JH, Sobel M, et al. Giant cell tumor of the distal radius. J Hand Surg Am 1995;20(3):432-440.
- Takigawa K. Chondroma of the bones of the hand. A review of 110 cases. J Bone Joint Surg Am 1971;53(8):1591-1600.
- Vander Griend RA, Funderburk CH. The treatment of giant-cell tumors of the distal part of the radius. J Bone Joint Surg Am 1993;75(6):899-908.
- Weiland AJ, Kleinert HE, Kutz JE, et al. Free vascularized bone grafts in surgery of the upper extremity. J Hand Surg Am 1979;4(2): 129-144.
