Comprehensive Introduction and Patho-Epidemiology
Radiographic and clinical studies have unequivocally demonstrated a profound association between structural impingement deformities of the hip and the premature development of secondary osteoarthritis. Anterior femoroacetabular impingement (FAI) encompasses a discrete category of structural hip disorders characterized by the abnormal, pathologic abutment of the anterolateral femoral head–neck junction against the acetabular rim–labral complex during physiologic ranges of motion. Historically, many of these hips were categorized as "idiopathic" osteoarthritis; however, contemporary understanding dictates that the vast majority of these degenerative joints are the end-stage result of unrecognized and untreated mechanical impingement. While authentic, longitudinal natural history data spanning decades are still being compiled, the prevailing consensus within the orthopedic community is that the prognosis for symptomatic impingement disorders is exceptionally poor if left to its natural course.
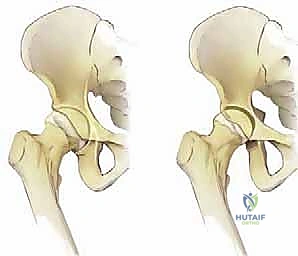
Structural impingement disease is broadly classified into three distinct pathoanatomic phenotypes: primarily femoral-based ("cam" impingement), primarily acetabular-based ("pincer" impingement), and combined cam-pincer impingement. Cam impingement is defined by an aspherical femoral head or reduced femoral head-neck offset, which forces a large-radius osseous prominence into the tight confines of the acetabulum during flexion. Pincer impingement occurs secondary to focal or global acetabular overcoverage, such as acetabular retroversion or coxa profunda, leading to a linear contact between the femoral neck and the acetabular rim. Combined cam and pincer impingement deformities are the most common clinical presentation, characterized by a synergistic abnormal anatomy of both the proximal femur and the acetabulum, compounding the mechanical insult to the joint.

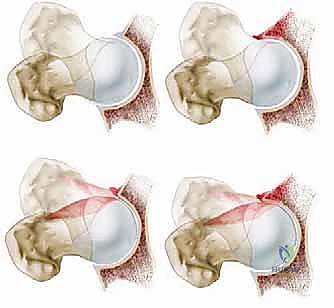
The pathogenesis of FAI initiates a highly destructive and predictable cascade of intra-articular biologic events. Repetitive anterolateral impingement, particularly pronounced during hip flexion and combined internal rotation, produces profound shear forces across the articular surface. In cam impingement, the aspherical head engages the acetabulum, leading to outside-in abrasion and eventual delamination of the adjacent acetabular articular cartilage, frequently leaving the labrum initially intact but detached from the subchondral bone. Conversely, pincer impingement primarily crushes the labrum between the femoral neck and the prominent acetabular rim, leading to intrasubstance labral degeneration and ossification, followed by a "contrecoup" chondral lesion in the posteroinferior acetabulum due to the levering of the femoral head.

Ultimately, this constellation of intra-articular disease worsens inexorably with time. The mechanical environment not only sustains but accelerates hip joint degeneration. Osseous impingement leads variously to profound delamination of the articular cartilage of the acetabular rim, progressive labral tearing and degeneration, and anterolateral femoral head–neck junction chondral disease. Future natural history studies, leveraging advanced imaging and long-term multi-center registries, will add substantially to our improved understanding of these disorders, allowing surgeons to better predict which asymptomatic deformities will inevitably progress to catastrophic joint failure.
Detailed Surgical Anatomy and Biomechanics
Understanding the intricate pathoanatomy and biomechanics of hip impingement disorders is absolutely essential to establishing an accurate diagnosis and selecting an optimal surgical treatment strategy. The proximal femur's anatomy dictates its clearance within the acetabulum. Deformities of the proximal femur that produce impingement disease include reduced femoral head–neck offset, an aspherical femoral head (frequently quantified by an elevated alpha angle), slipped capital femoral epiphysis (SCFE) deformities, Perthes-like morphological abnormalities, and femoral neck malunions secondary to prior trauma. A normal femoral head-neck junction possesses a concave contour that smoothly transitions into the acetabulum during terminal flexion; the loss of this concavity is the hallmark of the cam lesion.

On the acetabular side, the spatial orientation and depth of the socket are paramount. Common impingement deformities include acetabular retroversion, coxa profunda, and protrusio acetabuli. Normal acetabular version is characterized by an anteverted orientation, allowing clearance for the anterior femoral neck during flexion. In retroversion, the anterior wall projects further laterally than the posterior wall at the cranial aspect of the joint, creating a "crossover sign" on a well-centered anteroposterior (AP) radiograph. This focal anterior overcoverage acts as a mechanical block, prematurely engaging the femoral neck and initiating the pincer impingement cascade.
Biomechanically, the hip joint is subjected to extraordinary forces, often exceeding several times body weight during routine daily activities and athletic endeavors. Mechanical impingement is most pronounced with hip flexion alone, or the combination of hip flexion, adduction, and internal rotation (FADIR). During these maneuvers, the cam lesion acts as a cam-lobe mechanism, forcefully peeling the labrum away from the articular cartilage at the chondrolabral junction. The transition zone between the fibrocartilaginous labrum and the hyaline cartilage is particularly vulnerable to these shear forces, explaining the high prevalence of chondrolabral separation observed surgically.

The surgical anatomy relevant to the anterior approach for FAI treatment requires a meticulous understanding of the anterior soft-tissue envelope and the neurovascular structures. The anterior approach (often a modified Smith-Petersen or Hueter interval) exploits the internervous plane between the tensor fasciae latae (superior gluteal nerve) and the sartorius/rectus femoris (femoral nerve). The ascending branches of the lateral femoral circumflex artery (LFCA) consistently cross this operative field and must be meticulously ligated to prevent postoperative hematoma. Furthermore, preserving the integrity of the medial circumflex femoral artery (MCFA) and its terminal retinacular branches, which course posterosuperiorly along the femoral neck, is critical during capsulotomy and osteochondroplasty to avert iatrogenic avascular necrosis (AVN) of the femoral head.
Exhaustive Indications and Contraindications
Patients with anterior femoroacetabular impingement commonly present with insidious, activity-related anterior inguinal (groin) pain, frequently described by the patient forming a "C" with their hand around the hip (the "C-sign"). Associated lateral trochanteric and deep posterior gluteal pain are also common, often representing compensatory muscular fatigue or referred pain patterns. Symptoms are highly variable and may include a combination of deep, dull aching pain exacerbated by prolonged sitting, with intermittent episodes of sharp or stabbing pain during pivoting or twisting motions. High-demand athletic activities, including running, cutting, pivoting, and repetitive hip flexion (e.g., soccer, hockey, martial arts), invariably exacerbate symptoms and are often the catalyst for seeking medical evaluation.

A comprehensive physical examination is critical. The gait pattern over short distances and abductor strength usually are normal in the early stages of the disease. However, mechanical symptoms of locking, catching, and clicking may be problematic, presumably emanating from unstable labral tears or displaced articular cartilage flaps. As labral disease and joint degeneration progress, a visible Trendelenburg limp and mild abductor weakness may develop. Hip range-of-motion testing must be performed carefully with stabilization of the pelvis to accurately define true capsular motion endpoints. Passive hip flexion motion and internal rotation at 90 degrees of flexion are characteristically restricted. The anterior impingement test (FADIR) and Patrick’s test (FABER) are highly sensitive provocative maneuvers designed to detect intrinsic hip disease and usually reproduce the patient's exact concordant hip symptoms.

Nonoperative management for the treatment of anterior FAI has not been rigorously proven to alter the natural history of the structural deformity. While activity restrictions, targeted physical therapy (avoiding aggressive flexion/internal rotation stretches), non-steroidal anti-inflammatory drugs (NSAIDs), and intra-articular corticosteroid injections can be considered as temporizing measures, they do not address the underlying pathomechanics. The benefit of nonoperative treatment has not been established for joints that are relatively healthy but structurally abnormal. Patients with symptomatic FAI who desire to maintain high activity levels almost universally fail nonoperative management and require surgical intervention to prevent progressive chondral destruction.

Careful patient selection requires differentiating FAI from isolated intra-articular hip disease (e.g., synovial chondromatosis, isolated loose bodies) in the absence of an impingement disorder, mild hip dysplasia (where osseous resection would exacerbate instability), and extra-articular disorders (e.g., lumbar radiculopathy, athletic pubalgia, inguinal hernia). Contraindications to joint-preserving FAI surgery must be strictly observed to avoid early catastrophic failure.
| Clinical Parameter | Indications for Joint Preservation | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Radiographic OA | Tönnis Grade 0 or 1 | Tönnis Grade 3 | Tönnis Grade 2 |
| Joint Space | > 2.5 mm | < 2.0 mm globally | 2.0 - 2.5 mm focally |
| Age | Skeletally mature to 45 years | > 60 years | 45 - 60 years |
| Morphology | Focal Cam/Pincer deformity | Severe Dysplasia (LCEA < 20°) | Mild Dysplasia (LCEA 20-25°) |
| Clinical Status | Failed 3+ months conservative care | Active intra-articular infection | Chronic pain syndromes (CRPS) |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning begins with an exhaustive review of the patient's history, physical examination findings, and assessment of overall health, conditioning, and body habitus. Previous surgical scars must be inspected to clarify the nature of previous procedures and to anticipate altered surgical planes. A standardized, high-quality radiographic series is mandatory. Plain radiographs must include a well-centered supine AP view of the pelvis (to assess pelvic tilt and rotation), a cross-table lateral view with the extremity in 15 degrees of internal rotation (to profile the anterior head-neck junction), and a frog-leg lateral view.

The structural parameters of the hip are meticulously assessed on all radiographic views. Acetabular inclination, lateral center-edge angle (LCEA), and acetabular version are determined from the AP view. The presence of a crossover sign, prominent ischial spine sign, or posterior wall sign must be documented. Joint space narrowing, periarticular cysts, and labral ossification are noted as indicators of advanced disease. The lateral views are examined specifically to assess femoral head sphericity, calculate the alpha angle, and measure the anterior femoral head–neck offset. Hip flexion is commonly restricted to 100 degrees or less, and internal rotation in flexion is frequently restricted to 0 to 10 degrees in these patients; these clinical parameters should be correlated with the radiographic deformities.

Advanced imaging is utilized routinely to define the extent of soft tissue and osseous pathology. An MR arthrogram (MRA) of the hip is obtained on all patients with suspected impingement. The MRA is invaluable for assessing the contour of the femoral head–neck junction, detailing labral tears, identifying chondrolabral delamination, and excluding other uncommon disorders such as stress fractures, osteonecrosis, neoplasm, and infection. Furthermore, a fine-cut CT scan with 3D reconstructions can be exceptionally useful in identifying and characterizing the complex, three-dimensional extent of osseous impingement lesions, particularly in cases of severe or combined deformities. This allows the surgeon to mentally map the exact volume and location of bone requiring resection.

Patient Positioning and Operating Room Setup
Proper patient positioning is critical for the success of a combined arthroscopic and limited open anterior approach. Spinal or general anesthesia with profound muscle relaxation is preferred to facilitate joint distraction. The patient is positioned supine on a radiolucent fracture table equipped with lower-extremity traction attachments. The feet and ankles must be meticulously padded and firmly stabilized within the traction boots to prevent pressure necrosis. The perineal post is heavily padded and positioned slightly laterally against the medial thigh of the operative leg to direct the traction vector appropriately and prevent devastating pudendal nerve palsy.

The operative hip is initially positioned in neutral flexion–extension and slight (0 to 10 degrees) abduction. The operative lower extremity is internally rotated 15 to 20 degrees to bring the femoral neck parallel to the floor, optimizing the AP fluoroscopic view. Traction is applied to the operative hip to achieve 8 to 10 mm of joint distraction, breaking the suction seal of the joint, which is confirmed with fluoroscopy. Traction is temporarily released during the preparation and draping of the hip to minimize total traction time. The contralateral hip is flexed approximately 15 degrees and abducted 10 to 20 degrees, and minor traction is applied to stabilize the pelvis and prevent pelvic obliquity during the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The fundamental goal of surgery, independent of the specific technique selected, is to definitively address the structural osseous impingement lesions and meticulously manage the associated intra-articular disease elements (e.g., labral tears, articular cartilage delamination). For hips with focal, cam-type anterior femoroacetabular impingement, less-invasive surgical techniques offer distinct advantages regarding morbidity and recovery. In such cases, a combined approach is highly efficacious: hip arthroscopy is utilized to precisely address the intra-articular disease, followed immediately by a limited open osteochondroplasty through an anterior incision to correct the femoral-sided impingement deformity under direct visualization.

The Arthroscopic Phase
Hip arthroscopy is performed first via standard anterior, anterolateral, and posterolateral portals with the patient in the supine position under traction. The central compartment is accessed, and a comprehensive diagnostic arthroscopy is performed. The labrum is probed for instability, and the adjacent acetabular cartilage is assessed for the classic "wave sign" indicative of delamination. If a pincer lesion is present, the labrum is carefully detached from the rim, the overhanging acetabular bone is trimmed using a motorized burr under fluoroscopic guidance, and the labrum is securely refixed using suture anchors. Once the central compartment work is complete, traction is released, and the peripheral compartment is inspected.

The Limited Open Anterior Approach
Following the arthroscopic phase, the limited open osteochondroplasty is initiated. A longitudinal incision of approximately 6 to 8 centimeters is made extending distally from the anterior superior iliac spine (ASIS), following the interval between the tensor fasciae latae (TFL) laterally and the sartorius medially. The superficial fascia is incised, and the internervous plane is bluntly developed. Care must be taken to identify and protect the lateral femoral cutaneous nerve (LFCN), which typically courses over the sartorius muscle but exhibits significant anatomic variability.

Deep dissection proceeds by retracting the rectus femoris medially and the gluteus medius laterally. The ascending branches of the lateral femoral circumflex artery are consistently encountered crossing this field; they must be isolated, clamped, and electrocoagulated or ligated to prevent postoperative hematoma. The anterior capsule of the hip joint is now exposed. An I-shaped or T-shaped capsulotomy is performed. The transverse limb of the capsulotomy is made parallel to the acetabular rim, while the longitudinal limb extends distally along the axis of the femoral neck. Stay sutures are placed in the capsular flaps to facilitate exposure.

Osteochondroplasty of the Femoral Head-Neck Junction
With the capsule retracted, the cam deformity at the anterolateral femoral head-neck junction is directly visualized. The extent of the lesion is correlated with preoperative templating and intraoperative fluoroscopy. Using a high-speed spherical burr or curved osteotomes, the abnormal bone is methodically resected. The goal is to recreate a normal, concave femoral head-neck offset. Resection must be precise; over-resection dramatically increases the risk of iatrogenic femoral neck fracture, while under-resection leads to persistent impingement and surgical failure. The widely accepted "30% rule" dictates that no more than 30% of the cross-sectional diameter of the femoral neck should be resected.

Crucially, the resection must not extend posterosuperiorly into the retinacular vessels (branches of the MCFA) that provide the primary blood supply to the femoral head. Disruption of these vessels will result in devastating avascular necrosis. Once the osteochondroplasty is complete, dynamic intraoperative testing is mandatory. The hip is taken through a full range of motion, specifically maximizing flexion and internal rotation, to visually and tactilely confirm that impingement-free motion has been achieved and that the femoral neck clears the acetabular rim.

Following confirmation of adequate decompression, the joint is thoroughly irrigated to remove all osseous debris, which could otherwise act as a nidus for heterotopic ossification or third-body wear. The capsule is then meticulously repaired using heavy, non-absorbable sutures. Capsular closure is paramount to restore the native biomechanics of the iliofemoral ligament, prevent iatrogenic microinstability, and minimize the risk of postoperative subluxation. The deep and superficial fascial layers are closed in a standard layered fashion.

Complications, Incidence Rates, and Salvage Management
While joint-preserving surgery for FAI yields excellent outcomes in appropriately selected patients, the procedures are technically demanding, and complications can be profound. Iatrogenic neurovascular injury is a primary concern. Transient neuropraxia of the pudendal nerve or sciatic nerve can occur secondary to prolonged or excessive traction during the arthroscopic phase. Strict adherence to traction time limits (generally less than 2 hours) and meticulous perineal padding minimize this risk. Injury to the lateral femoral cutaneous nerve (LFCN) is the most common neurological complication of the anterior limited open approach, occurring in up to 10% of cases, though it is usually transient.

Structural complications involving the proximal femur are devastating. Iatrogenic femoral neck fracture is a catastrophic complication directly related to over-resection of the cam lesion. Adhering to the 30% cross-sectional resection rule and enforcing strict postoperative weight-bearing restrictions are critical preventative measures. Similarly, avascular necrosis (AVN) of the femoral head can result from inadvertent damage to the extraosseous retinacular vessels during capsulotomy or overly aggressive posterosuperior osteochondroplasty. Surgeons must maintain a healthy respect for the vascular anatomy, particularly the terminal branches of the medial circumflex femoral artery.

Heterotopic ossification (HO) and intra-articular adhesions are well-documented postoperative sequelae that can severely limit range of motion and cause recurrent pain. Routine prophylaxis with NSAIDs (e.g., Indomethacin or Naproxen) for 2 to 4 weeks postoperatively significantly reduces the incidence of clinically relevant HO. Finally, the most common cause of revision surgery is under-resection of the impingement deformity, leading to persistent mechanical symptoms. Salvage management for failed joint preservation surgery typically involves revision osteochondroplasty if the joint space is preserved, or conversion to Total Hip Arthroplasty (THA) if secondary osteoarthritis has progressed.
| Com
