Introduction to Patellar Fracture Management
The patella is the largest sesamoid bone in the human body, serving a critical biomechanical role in the extensor mechanism of the knee. It increases the moment arm of the quadriceps tendon, thereby significantly enhancing the mechanical advantage of knee extension. The initial treatment of acute patellar fractures must prioritize the protection of the soft tissue envelope and the prevention of further displacement.
In the acute setting, the extremity should be immediately splinted in full extension or slight flexion. Cryotherapy (ice application) is highly recommended to mitigate hemarthrosis and soft tissue swelling; however, to prevent thermal soft tissue damage, ice must never be applied directly to the skin. A thorough neurovascular examination and assessment of the overlying skin are mandatory, as the subcutaneous nature of the patella makes it highly susceptible to open fractures and severe soft tissue contusions.
Nonoperative Management
Nonoperative management is reserved for a highly specific subset of patients. Closed fractures with minimal displacement, minimal articular incongruity, and an intact extensor retinaculum (evidenced by the patient's ability to perform a straight-leg raise) can be successfully treated conservatively.
Indications and Acceptable Parameters
The definition of "acceptable displacement" has evolved, but strict adherence to radiographic parameters is essential to prevent post-traumatic patellofemoral arthritis and extensor lag.
- Boström Criteria: Historically, Boström considered 3 to 4 mm of fragment separation and 2 to 3 mm of articular incongruity to be the maximum acceptable limits for nonoperative treatment. If either parameter is exceeded, operative intervention is indicated. In his long-term follow-up, fractures meeting these criteria and treated nonoperatively yielded the best overall functional results.
- Edwards, Johnell, and Redlund-Johnell Criteria: A more stringent 30-year long-term follow-up study by Edwards et al. demonstrated that two-thirds of patients with more than 2 mm of diastasis or 1 mm of articular incongruity developed chronic complaints and objectively reduced quadriceps strength. Therefore, modern practice leans toward these stricter parameters.
Nonoperative Protocol
Nonoperative treatment consists of immobilizing the knee in full extension using a well-molded cylinder cast or a rigid locked hinged knee brace from the ankle to the groin. Immobilization is typically maintained for 4 to 6 weeks. Weight-bearing is allowed as tolerated in full extension. Serial radiographs should be obtained at 1, 2, and 4 weeks to ensure no secondary displacement occurs as swelling subsides.
Operative Management: Principles and Indications
Fractures associated with extensor retinacular tears, open fractures, and closed fractures exhibiting more than 2 to 3 mm of displacement or >1 to 2 mm of articular incongruity are best treated operatively.
The primary surgical goals are:
1. Anatomic restoration of articular congruity to minimize post-traumatic arthritis.
2. Robust repair of the extensor mechanism.
3. Rigid internal fixation secure enough to permit early postoperative range of motion (ROM).
Timing of Surgery
When the soft tissue envelope is pristine, osteosynthesis should be performed as soon as practical. Unnecessary delay retards convalescence, exacerbates quadriceps atrophy, and unfavorably affects the final functional outcome.
Surgical Warning: If severe contusion, fracture blisters, or deep abrasions are present, surgery must be delayed. Operating through compromised skin drastically increases the risk of deep infection. In cases of superficial infection or severe abrasion, surgery should be delayed 7 to 10 days until the soft tissue envelope has re-epithelialized and the danger of contaminating the operative wound is minimal.
Management of Open Patellar Fractures
Open fractures of the patella are a surgical emergency. They require immediate administration of intravenous antibiotics, tetanus prophylaxis, and urgent surgical débridement and irrigation.
* Soft Tissue Coverage: Early soft tissue coverage (within 5 days) significantly reduces the incidence of deep infection.
* Fixation Strategy: The same surgical techniques used for closed fractures can be successfully applied to open fractures. Literature reports 77% good or excellent results following the operative treatment of open patellar fractures.
* Vascular Considerations: Soft tissue stripping must be kept to the absolute minimum necessary to stabilize the fracture. Torchia and Lewellen strongly discourage the use of circumferential cerclage wires in open fractures due to their potential adverse effects on the already compromised osseous vascularity.
Biomechanics of the Extensor Mechanism
Understanding the biomechanics of the patellofemoral joint is crucial when deciding between osteosynthesis, partial patellectomy, and total patellectomy. Historically, some authors claimed the patella was a phylogenetic remnant that could be excised without consequence. This has been definitively refuted.
Haxton demonstrated that the power of knee extension increases as the joint extends; the power is significantly greater at 30 degrees of flexion than at 60, 90, or 120 degrees. Kaufer's landmark biomechanical study comparing intact and patellectomized cadaveric knees revealed that 15% to 30% more quadriceps force is required to fully extend a patellectomized knee compared to an intact knee.
Because extension is the most critical function of the knee, patellectomy definitively impairs the mechanical efficiency of the quadriceps. While this impairment may not completely prevent ordinary activities, Peeples and Margo found that 15% of patellectomy patients developed an extensor lag, and 50% reported significant weakness affecting stair climbing. Long-term studies by Jakobsen et al. and Edwards et al. reported permanent reductions in quadriceps strength of 33% and 44%, respectively, following total patellectomy.
Surgical Techniques: Osteosynthesis
Accepted methods for patellar osteosynthesis include various wiring techniques, cannulated screw fixation, and specialized plating. Marya, Bhan, and Dove demonstrated the superiority of fixation, reporting 80% excellent results after anterior tension band osteosynthesis compared to only 50% excellent results after patellectomy.
Wiring Techniques
The anterior tension band principle is the gold standard for transverse patellar fractures. It functions by converting the tensile distraction forces at the anterior cortex (generated by the quadriceps) into compressive forces at the articular surface during knee flexion.
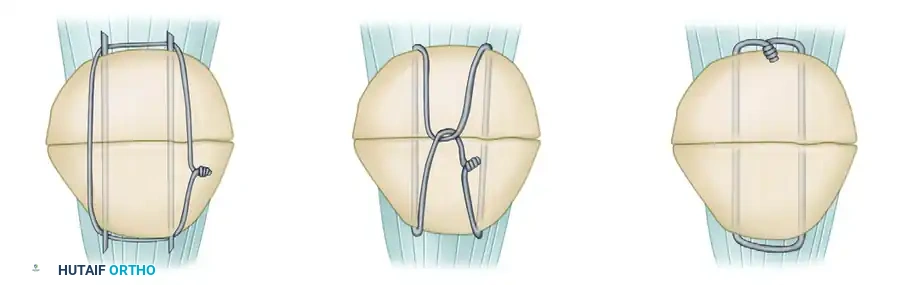
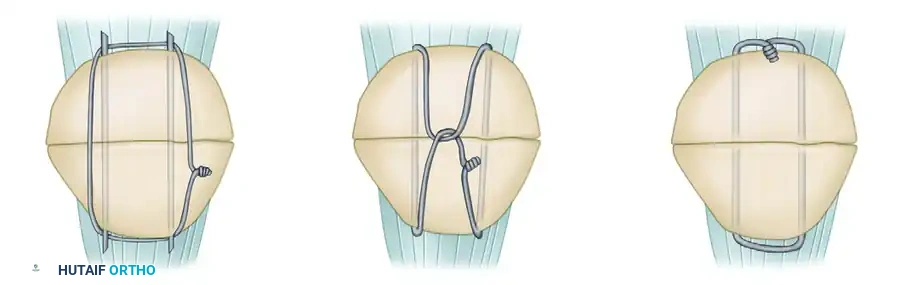
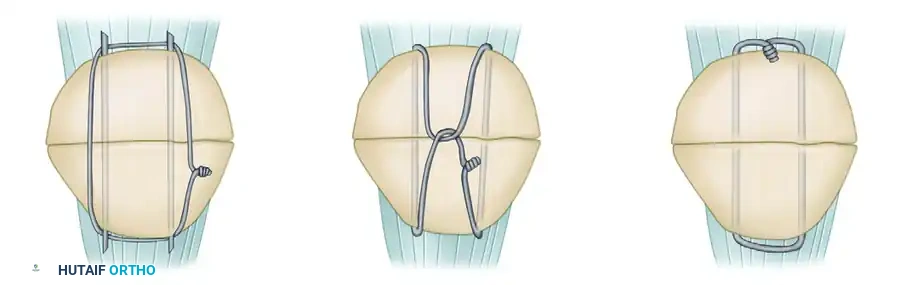
Figure 54-61: Types of patellar fixation. A, Modified tension band. B, Lotke longitudinal anterior band (LAB) wiring. C, Magnusson wiring.
- Modified Tension Band Wiring (Figure 54-61, A): Two parallel longitudinal Kirschner wires (K-wires) or cannulated screws are passed from superior to inferior through the fracture fragments. A flexible stainless steel wire (usually 18-gauge) is passed behind the pins proximally and distally in a figure-of-eight fashion over the anterior surface of the patella. As the wire is tensioned, it compresses the anterior cortex.
- Lotke Longitudinal Anterior Band (LAB) Wiring (Figure 54-61, B): Utilizes a longitudinal wiring configuration to provide stability, particularly useful in specific fracture patterns where a figure-of-eight may not provide uniform compression.
- Magnusson Wiring (Figure 54-61, C): An alternative wiring technique designed to capture the poles of the patella securely.
Management of Inferior Pole Comminution
Preserving the inferior pole is highly desirable to maintain patellar length and allow earlier motion.
* Vertical Wiring: Yang and Byun reported excellent functional results with no hardware failure or nonunions in 25 patients treated with a separate vertical wiring technique for comminuted inferior pole fractures. Biomechanically, this proved stronger than partial patellectomy with pull-out sutures.
* Basket Plates: Matejcic et al. described the use of a specialized basket plate for comminuted inferior poles. In 51 patients, 46 achieved good to excellent results, with zero poor results reported.
External Fixation
While less common, open reduction and external fixation using superior and inferior pins placed transversely (adjacent to the proximal and distal poles) and connected to compressive clamps has been utilized for transverse and comminuted fractures. Liang and Wu advocate this method to save all major fragments, allowing motion at 2 weeks and frame removal at 4 weeks. Circular external fixation under arthroscopic control has also been described, though it remains a highly specialized technique.
Partial Patellectomy
Because of the severe biomechanical penalties of total patellectomy, the surgeon must make every effort to save all of the patella, or at least the proximal or distal third. If a pole is severely comminuted and articular reconstruction is impossible, a partial patellectomy is indicated.
Fragment Preservation and Fixation
When partial patellectomy is chosen, as much of the patella as possible must be salvaged. Larger comminuted pieces can occasionally be secured to the main fragment using small interfragmentary screws to increase the size of the retained patellar remnant. The unsalvageable fragments are excised, and the extensor mechanism (quadriceps or patellar tendon) is reattached to the remaining bone via heavy non-absorbable sutures passed through longitudinal drill holes.
Clinical Pearl: The size of the retained fragment matters. Marder et al. demonstrated marked alterations in patellofemoral contact areas after a 60% patellectomy, reducing the contact area to less than 50% of normal. Saltzman et al. noted that in successful outcomes, the salvaged fragment averaged 11.8 cm².
The Tendon Reattachment Controversy
The precise anatomic site for reinserting the tendon into the patellar remnant is highly debated:
* Articular Edge Reattachment: Saltzman et al. recommended reattachment near the articular edge to prevent mechanical step-off. However, biomechanical cadaver models show this increases the force required to extend the knee.
* Anterior Cortex Reattachment: Marder et al. found that posterior (articular) attachment caused the proximal pole of the patella to tilt abnormally into the femoral articular surface. Conversely, anterior reattachment restored a more normal pattern of patellofemoral contact. Zhao et al. corroborated this, reporting highly satisfactory clinical results in 21 patients with anterior cortex reattachment.
Regardless of the chosen site, intraoperative lateral radiographs must be evaluated carefully before closure to ensure the extensor mechanism is not excessively shortened and the remaining patella is tracking smoothly without abnormal tilt.
Total Patellectomy
Total patellectomy is a salvage procedure of last resort, indicated strictly when comminution is so extensive that no functional articular surface can be reconstructed, and no fragment is large enough to anchor the extensor mechanism.
Surgical Technique and Soft Tissue Management
The procedure involves meticulous subperiosteal enucleation of the patellar fragments to preserve the continuous sleeve of the extensor retinaculum. The quadriceps tendon is then directly repaired to the patellar tendon.
To counteract the inevitable loss of mechanical advantage, Günal et al. compared simple patellectomy with patellectomy combined with advancement of the vastus medialis obliquus (VMO). At a minimum 3-year follow-up, functional results and extensor power were significantly superior in the VMO advancement cohort.
Despite the documented quadriceps weakness and atrophy, long-term follow-up studies indicate that 78% of patients eventually achieve good or excellent subjective results following total patellectomy, provided the retinacular repair is robust and rehabilitation is strictly adhered to. Kaufer noted that elevating the tibial tubercle by 1.5 cm can theoretically eliminate the biomechanical deficit of a patellectomy, though in clinical practice, this secondary procedure is seldom necessary.
Postoperative Rehabilitation Protocol
The success of patellar fracture surgery is heavily dependent on the postoperative rehabilitation protocol, which must be tailored to the security of the fixation.
- Phase I (0-2 Weeks): The knee is typically immobilized in a hinged knee brace locked in full extension. Weight-bearing as tolerated in extension is permitted. Isometric quadriceps exercises (quad sets) and straight-leg raises are initiated immediately to prevent profound atrophy.
- Phase II (2-6 Weeks): If rigid osteosynthesis was achieved, controlled active-assisted range of motion is initiated. Flexion is gradually increased (e.g., 0-30 degrees initially, progressing by 15-30 degrees weekly). The brace remains locked in extension for ambulation.
- Phase III (6-12 Weeks): Once radiographic union is evident (typically 6-8 weeks), the brace is discontinued. Progressive resistance exercises, stationary cycling, and closed-kinetic-chain strengthening are emphasized. Full functional recovery may take 6 to 12 months.
Conclusion
The management of patellar fractures requires a nuanced understanding of knee biomechanics and meticulous surgical execution. While nonoperative treatment is highly effective for strictly defined, undisplaced fractures, operative intervention is mandatory for displaced or open injuries. The overarching goal remains the preservation of the patella through rigid osteosynthesis to maintain the mechanical advantage of the extensor mechanism. When comminution dictates partial or total patellectomy, precise soft tissue management and tendon reattachment techniques are paramount to minimizing postoperative extensor lag and optimizing long-term patient outcomes.
