TRANSCHONDRAL FRACTURES AND SEVERE TALAR INJURIES
The talus is a unique biomechanical keystone of the lower extremity, transmitting the entire weight of the body from the tibia to the foot. Because approximately 60% of its surface is covered by articular cartilage, it possesses a highly tenuous, retrograde blood supply. This anatomic reality makes the talus exceptionally vulnerable to osteonecrosis (avascular necrosis) following trauma.
While isolated transchondral fractures of the talar dome are frequently managed via arthroscopic debridement, microfracture, or osteochondral autograft transfer (discussed extensively in dedicated arthroscopy literature), high-energy trauma often results in far more devastating injuries. These include displaced fractures of the talar processes (lateral and posterior) and the catastrophic extrusion of the entire talar body.
Clinical Pearl: The primary goal in managing severe talar trauma is the restoration of articular congruity and the preservation of hindfoot height and biomechanics, even in the face of a high risk of subsequent osteonecrosis.
POSTERIOR PROCESS FRACTURES OF THE TALUS
Pathoanatomy and Clinical Presentation
The posterior process of the talus consists of two distinct tubercles: the lateral tubercle (often associated with an unfused os trigonum) and the medial tubercle. The tendon of the flexor hallucis longus (FHL) runs in the sulcus directly between these two tubercles.
Fractures of the posterior process are notoriously difficult to diagnose on standard radiographs and are frequently misdiagnosed as severe ankle sprains. Significant clinical attention must be directed toward posteromedial process fractures. These injuries are frequently associated with medial subtalar dislocations, though they can occur with lesser, twisting injuries. If left unrecognized, they lead to severe, long-term hindfoot disability, chronic pain, and FHL tenosynovitis.
Patients typically present with posteromedial or posterolateral ankle pain, swelling, and localized tenderness. A key clinical indicator is pain exacerbated by passive extension and active flexion of the great toe, as the FHL tendon glides through the fractured osseous tunnel.
Surgical Warning: If a patient has sustained an ankle injury and fails to improve after 6 to 8 weeks of conventional conservative treatment (immobilization and protected weight-bearing), a high index of suspicion must be maintained for a missed posterior or lateral talar process fracture.
Diagnostic Imaging
Standard anteroposterior (AP) and lateral radiographs of the ankle often fail to clearly delineate posterior process fractures due to osseous overlap of the malleoli and the calcaneus. A lateral radiograph of the contralateral foot is highly recommended for comparison to differentiate an acute fracture from a bipartite os trigonum.
Computed Tomography (CT) is the gold standard for definitive diagnosis, allowing for precise localization of the fragment, assessment of articular involvement (subtalar joint), and surgical planning.

Preoperative lateral radiograph demonstrating a suspicious osseous density posterior to the talus, often difficult to distinguish from an os trigonum without advanced imaging.

Preoperative sagittal CT scan clearly delineating a large, displaced posterior process fracture with intra-articular extension into the subtalar joint.
Nonoperative Management
A trial of nonoperative treatment is indicated for acute, non-displaced fractures. This consists of rigid immobilization in a short-leg cast or controlled ankle motion (CAM) boot with limited weight-bearing for 4 to 6 weeks.
In reports detailing avulsion fractures of the medial tubercle of the posterior process, patients generally achieve excellent outcomes with acute immobilization. However, fractures that are missed initially and present late typically respond poorly to conservative measures.
Surgical Technique: Excision of the Posterior Process
Persistence of symptoms, localized tenderness, and failure of nonoperative management are absolute indications for surgical excision of the fractured fragment.
Step-by-Step Approach:
1. Positioning: The patient is positioned prone to allow optimal access to the posterior ankle. A thigh tourniquet is applied.
2. Incision: A posterolateral or posteromedial incision is utilized depending on the primary location of the fragment. For lateral tubercle fractures, an incision is made just lateral to the Achilles tendon.
3. Dissection: The sural nerve and lesser saphenous vein are identified and protected laterally. The deep fascia is incised, and the interval between the peroneal tendons and the FHL is developed.
4. Fragment Excision: The fractured fragment is identified. Care must be taken to meticulously dissect the FHL tendon free from the fragment to prevent postoperative tethering. The fragment is sharply excised.
5. Closure: The surgical bed is irrigated, and the retinaculum is repaired to prevent tendon subluxation.

Postoperative lateral radiograph following successful excision of the posterior process fragment. The patient subsequently became asymptomatic with full restoration of FHL excursion.
LATERAL PROCESS FRACTURES OF THE TALUS
Lateral process fractures (often termed "snowboarder's fractures") occur via a mechanism of axial loading combined with dorsiflexion and inversion. The lateral process articulates with both the fibula and the calcaneus; thus, displaced fractures severely disrupt the lateral column of the ankle and the subtalar joint.
Imaging and Indications
Like posterior process fractures, lateral process fractures are easily missed on plain radiographs. Coronal CT imaging is essential to evaluate the degree of displacement and comminution. Displaced fractures (>2 mm) or those causing subtalar incongruity require Open Reduction and Internal Fixation (ORIF).
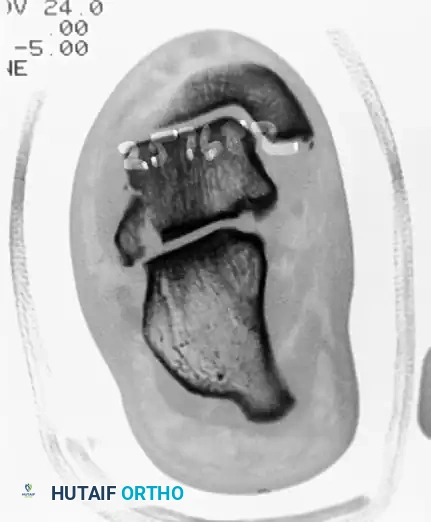
Preoperative coronal CT scan demonstrating a significantly displaced lateral process fracture of the talus, disrupting the subtalar articulation.
Surgical Technique: ORIF of the Lateral Process
- Positioning: Supine with a bump under the ipsilateral hip to internally rotate the leg, providing direct access to the lateral ankle.
- Approach: An anterolateral approach is utilized, starting proximal to the ankle joint and extending distally toward the base of the fourth metatarsal.
- Reduction: The fracture hematoma is evacuated. The fragment is anatomically reduced using a dental pick or small point-to-point reduction forceps.
- Fixation: Stabilization is achieved using two 2.0 mm or 2.4 mm cortical lag screws.
- Countersinking: It is critical that the screw heads are fully countersunk beneath the articular cartilage to prevent impingement against the lateral malleolus or calcaneus.

Postoperative Anteroposterior (AP) radiograph showing anatomic reduction and stabilization of the lateral process.
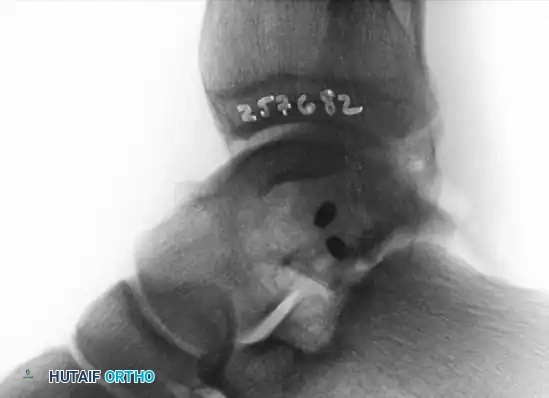
Postoperative lateral radiograph confirming the placement of fully countersunk screws, ensuring no intra-articular hardware prominence.
TALAR BODY EXTRUSION
Extrusion of the talar body, or the entire talus (pan-talar extrusion), is a devastating injury that typically occurs secondary to extreme high-energy trauma (e.g., motor vehicle collisions, falls from significant heights).
These injuries are almost universally open fractures, characterized by severe soft tissue stripping, gross contamination, and complete disruption of the talar blood supply (artery of the tarsal canal, deltoid branches, and sinus tarsi vessels).
The Dilemma of Reimplantation
Historically, consensus on the treatment of a completely extruded talar body has been lacking. The primary debate centers on whether to reimplant the avascular, contaminated bone or to discard it and perform a primary tibiocalcaneal fusion.
Because the functional results of primary talar body excision—with or without immediate tibiocalcaneal fusion—are most often poor due to massive limb length discrepancy and loss of ankle height, current evidence-based practice strongly favors the reimplantation of the extruded talus. Maintenance of limb length and the anatomic height of the ankle mortise is critical for long-term functional salvage.
Surgical Warning: The extruded talar body should be discarded and NOT replaced in only two specific situations:
1. Gross, unsalvageable contamination (e.g., farmyard injuries, sewage exposure).
2. Severe, non-reconstructable comminution and crushing of the talar body.
Prognosis and Complications
Surgeons must counsel patients extensively regarding the high complication rates associated with talar reimplantation:
* Osteonecrosis (AVN): Partial or total osteonecrosis rates vary from 54% to 83%. Rates are significantly higher when the extruded talus is concurrently fractured.
* Infection: While older literature reported infection rates as high as 50%, modern aggressive debridement protocols have reduced this to 0% to 10% in specialized trauma centers.
* Secondary Surgeries: Approximately 37% of patients will require subsequent surgical intervention (e.g., delayed arthrodesis, hardware removal, or core decompression).
Surgical Technique: Reimplantation
- Debridement: The extruded talus is subjected to meticulous, high-volume pulsatile lavage and soaked in a broad-spectrum antibiotic solution (e.g., Bacitracin/Polymyxin or Vancomycin) on the back table. The open wound undergoes aggressive surgical debridement of all necrotic soft tissue.
- Reduction: Open reduction is almost always required. The talus is carefully reinserted into the ankle mortise, ensuring correct anatomic orientation.
- Stabilization: The reimplanted talus is inherently unstable. A spanning external fixator or heavy transfixion Steinmann pins (driven from the calcaneus, through the talus, and into the tibia) must be used to hold the reduction and protect the soft tissue envelope.
- Soft Tissue Coverage: Immediate or early soft tissue coverage (often requiring free tissue transfer) is mandatory to prevent desiccation of the avascular bone.
MANAGEMENT OF THE MISSING OR UNSALVAGEABLE TALUS
In scenarios where the patient presents with a missing talus (lost at the scene of the accident), or the talus is deemed unsalvageable due to severe crushing or gross contamination, a staged "damage control" orthopedic protocol is required.
Stage 1: Acute Management
- Irrigation and Debridement: Aggressive I&D of the open joint space.
- Antibiotic Spacer: Placement of a polymethylmethacrylate (PMMA) antibiotic-impregnated spacer (typically loaded with Vancomycin and Tobramycin) into the void left by the missing talus. This maintains the dead space and delivers high local concentrations of antibiotics.
- External Fixation: Application of a rigid, spanning delta-frame external fixator to maintain limb length and stabilize the soft tissues.
- Systemic Therapy: Initiation of culture-directed intravenous antibiotics.
Stage 2: Definitive Reconstruction
At approximately 2 to 3 weeks post-injury, if the soft tissue envelope has healed and the patient remains free of clinical infection, the patient is returned to the operating room.
- Hardware Removal and Culturing: The external fixator is removed. Deep tissue cultures and fluid aspirates are taken from the pin sites and the ankle joint dead space.
- Decision Pathway based on Cultures:
- If Cultures are Negative (Aseptic): The surgeon proceeds with a tibiocalcaneal arthrodesis. To restore the height lost by the missing talus, a structural femoral head allograft is meticulously contoured and interposed between the distal tibia and the calcaneus. Rigid internal fixation is achieved using a retrograde intramedullary nail or heavy compression screws.
- If Cultures are Positive (Septic): Internal hardware and structural allografts are strictly contraindicated. The surgeon must perform a primary tibiocalcaneal arthrodesis utilizing external fixation. A Calandruccio compression clamp or a circular Ilizarov frame is preferred, as it provides dynamic compression across the fusion site without introducing internal foreign bodies. Long-term, infectious disease-guided intravenous antibiotics are administered until fusion is achieved.
POSTOPERATIVE PROTOCOLS
Whether managing a process fracture or a catastrophic extrusion, postoperative rehabilitation must be strictly controlled.
* Process Fractures: Patients are kept non-weight-bearing in a splint for 2 weeks, followed by transition to a CAM boot. Progressive weight-bearing and active range of motion (ROM) begin at 4 to 6 weeks, contingent upon radiographic evidence of healing.
* Talar Extrusions: Patients remain strictly non-weight-bearing for a minimum of 10 to 12 weeks. Serial radiographs are required to monitor for the Hawkins sign (subchondral radiolucency indicating revascularization) or the onset of sclerosis (indicating AVN). If AVN develops but the talus remains structurally intact without collapse, prolonged protected weight-bearing in a patellar tendon-bearing (PTB) orthosis may be utilized to prevent mechanical deformation while creeping substitution occurs.
