DEFINITION
Rheumatoid arthritis (RA) is a chronic, systemic, inflammatory condition of unknown etiology affecting 1% to 2% of the population.It affects females two to three times as frequently as males, and the incidence increases with age, typically peaking between 35 and 50 years of age.Peripheral joints are often affected in a symmetric pattern.The elbow is affected in about 20% to 70% of patients with RA, with a wide spectrum of severity.Ninety percent of these patients also have hand and wrist involvement and 80% also have shoulder involvement.Juvenile rheumatoid arthritis (JRA) is diagnosed based on the presence of arthritis, synovitis, or both in at least one joint lasting for more than 6 weeks in an individual younger than 16 years old.Compared with adult-onset RA, JRA is complicated by severe osseous destruction, deformity, and soft tissue contractures.
PATHOGENESIS
The cause of RA is unknown.Infectious etiologies have been proposed, but no microorganism has been proven to be causative.Genetic and twin studies have demonstrated that a genetic predisposition clearly exists, and the disease is also associated with autoimmune phenomena.In patients with RA, numerous cell types, including B lymphocytes, CD4 T cells, mononuclear phagocytes, neutrophils, fibroblasts, and osteoclasts, have been shown to produce abnormally high levels of various cytokines, chemokines, and other inflammatory mediators.The result is inflammatory-mediated proliferation of synovial tissue, leading to soft tissue and finally bony destruction.
NATURAL HISTORY
Overall, the disease progresses from predominantly soft tissue (synovial) inflammation to articular cartilage damage and ultimately subchondral and periarticular bone destruction.Manifestations of RA are initiated by synovitis and synovial hyperplasia resulting in pannus formation. This correlates with a boggy, inflamed elbow that is painful and with limited range of motion.Synovial proliferation coupled with joint capsule distention may produce a compressive neuropathy with pain, paresthesias, or weakness in the ulnar or radial nerve distributions, or both.Degeneration may progress to ligamentous erosion or disruption, or both. Clinically, the patient experiencesprogressive instability as ligamentous integrity is compromised.It may affect the annular ligament and produce radial head instability with anterior displacement.Eventually, the medial and lateral collateral ligament complexes may be disrupted, thus causing further instability.Prolonged synovitis leads to erosion of the cartilage followed by subchondral cyst formation and marginal joint erosions; the result is end-stage arthritis.End-stage disease is marked by severe damage to subchondral bone and gross joint instability. At this stage, patients typically have a painful, weak, and functionally unstable elbow.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients typically describe a history of a swollen, tender, and warm elbow with diminished and painful range of motion.This may be accompanied by a report of progressively declining function, constitutional complaints, and often polyarticular involvement.In early stages of the disease, the elbow may appear more boggy, with impressive soft tissue swelling and erythema about the elbow.As the disease progresses to later stages, soft tissue swelling may become less prominent and the elbow becomes more stiff and painful. Differences in Examination Findings between Rheumatoid Arthritis and Juvenile Rheumatoid Arthritis Elbows affected by JRA occur in younger patients as compared with elbows affected by RA. Patients with JRA also have stiffer elbows and therefore typically do not have instability.Often, JRA patients have more joints affected by the rheumatoid process, but they also demonstrate a greater tolerance for pain.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Anteroposterior (AP) and lateral radiographs of the elbow are obtained to assess the degree of rheumatoid involvement and for preoperative planning (FIG 1). No further studies are typically required.
CLASSIFICATION

FIG 1 • Preoperative AP and lateral radiographs of a 38-year-old woman with JRA demonstrating advanced changes of osteopenia, joint space narrowing, and changes in subchondral architecture.
DIFFERENTIAL DIAGNOSIS
Calcium pyrophosphate deposition disease OsteoarthritisPolymyalgia rheumatica Psoriatic arthritisSystemic lupus erythematosus Fibromyalgia
NONOPERATIVE MANAGEMENT
Optimal care of the patient with RA requires a team-based approach between the orthopaedic surgeon, rheumatologist, and physical therapists to coordinate the full gamut of nonsurgical and surgical treatment options.
MEDICAL THERAPY
The medical management of RA continues to evolve and is highly effective.Medical therapy includes classes of drugs known asdiseasemodifying antirheumatic drugs(DMARDs),immunomodulators,tumor necrosis factor(TNF)inhibitors, as well as other drugs targeting systemic inflammation. These medications may be given alone or as part of combination therapy.DMARDs include medications such as methotrexate, leflunomide, hydroxychloroquine, and sulfasalazine.Immunomodulators such as azathioprine and cyclosporine target the pathologic immune system but may also increase susceptibility to infection.Anti-TNF-alpha agents can reduce pain, morning stiffness, and swollen joints by inhibiting an inflammatory cytokine calledTNF-alpha. Examples of these drugs include etanercept, infliximab, adalimumab, golimumab, and certolizuman. These medications can also increase the risk of developing severe infection.Other medications which target inflammation include anakinra, abatacept, rituximab, tocilizumab, and tofacitinib.Nonsteroidal anti-inflammatory drugs (NSAIDs) and steroids, such as prednisone, may be prescribed to reduce symptoms of RA as well.Judicious use of intra-articular steroid injections also plays a role in symptom management.The importance of early referral to a rheumatologist for medical management cannot be overemphasized. Aggressive management of the synovitis can limit or delay the onset and severity of joint involvement. The most reliable and effective responses to antirheumatic medications are observed with therapy initiated in the early stages of the disease.
PHYSICAL THERAPY
The goal of physical therapy is to encourage range of motion, functional strength, and maintenance of activities of daily living. This is accomplished by activity modification, rest, ice, and gentle exercise.The primary objective of nonoperative management of the rheumatoid elbow is to minimize soft tissue swelling and to optimize range of motion, as preoperative range of motion is often predictive of postoperative total arc of motion after arthroscopic synovectomy as well as total elbow arthroplasty.
SURGICAL MANAGEMENT
Surgical management of the rheumatoid elbow primarily consists of synovectomy and total elbow arthroplasty. Surgical Management of the Elbow before Total Elbow Arthroplasty



Table 1 Mayo Radiographic Classification System


V Presence of bonyankylosis of the ulnohumeral jointMost commonly seen with JRAAdapted from Morrey BF, Adams RA. Semiconstrained arthroplasty for the treatment of rheumatoid arthritis of the elbow. J Bone Joint Surg Am 1992;74(4): 479-490; Connor PM, Morrey BF. Total elbow arthroplasty in patients who have juvenile rheumatoid arthritis. J Bone Joint Surg Am 1998;80(5):678-688.P.920An arthroscopic anterior capsular release may be performed at the time of the arthroscopic synovectomy to improve elbow extension. A posterior olecranon plasty may also be performed to reestablish normal concavity of the olecranon fossa.Posteromedial capsule release should be avoided to prevent the risk of iatrogenic ulnar nerve injury. If an elbow requires a release of the posterior capsule to regain elbow flexion (typically those with 100 degrees or less of preoperative flexion), then the surgeon should perform an open ulnar nerve decompression and subcutaneous transposition followed by complete posterior capsule release (including the posteromedial band of the medial collateral ligament).
TOTAL ELBOW ARTHROPLASTY
This procedure is indicated for advanced (grade III or IV) RA of the elbow in patients with significant pain and limitations in activities of daily living.Absolute contraindications include active infection, upper extremity paralysis, and a patient's refusal or inability to abide by postoperative activity restrictions.Relative contraindications include presence of infection at a remote site and a history of infected elbow or elbow prosthesis.
PREOPERATIVE PLANNING
AP and lateral radiographs of the elbow are reviewed to assess humeral bow and medullary canal diameter as well as angulation and diameter of the ulnar medullary canal.Preoperative radiographic templates may be helpful to assess preoperative radiographic magnification.In particular for JRA patients, the canal width may be very small, and therefore the surgeon must ensure that appropriately sized implants as well as intramedullary guidewires and reamers are available.If an ipsilateral total shoulder arthroplasty has been performed or is anticipated, a humeral cement restrictor should be used. A 4-inch humeral implant may also be considered; however, shorter, recently introducedhumeral components for total shoulder arthroplasty can typically be placed even in the presence of a 6-inch humeral stem. Overlapping cement mantles and/or a short cement gap between the humeral stems of the shoulder and elbow prostheses should be avoided to reduce the risk of subsequent periprosthetic fracture.Preoperative limitations in forearm rotation may be due in part to ipsilateral distal radioulnar joint pathology. Thus, radiographs should also be obtained of the ipsilateral shoulder and wrist.Implant Selection for Total Elbow ArthroplastyImplant options have traditionally been classified as linked (semiconstrained) or unlinked.These terms are being used with decreasing frequency, however, as some unlinked implant designs have been developed that have precisely contoured components that create a degree of constraint.Linked, semiconstrained implants inherently have about 7 degrees of varus-valgus and 7 degrees of axial rotation, “play,” whereas unconstrained implants typically refer to unlinked, resurfacing components.The stability of unconstrained implants depends on soft tissue and ligamentous integrity. Such tissues may be destroyed by the rheumatoid inflammatory process or surgically released with semiconstrained implants without compromising stability.Although no prospective comparisons between linked (semiconstrained) and unlinked implants have yet been performed, studies have generally reported improved survivorship with a semiconstrained design.7The semiconstrained design is preferred because it is equally effective in pain relief and in improving range of motion and function while preserving stability without an observed increase in aseptic loosening.7The Techniques section describes implantation of a linked, semiconstrained implant.Polyethylene bushing wear is a challenging issue which has been implicated as a limiting factor in long-term implant durability following total elbow arthroplasty.2,5,10 Polyethylene wear has been reported after total elbowarthroplasty with multiple implant designs.5,10 Osteolysis and loosening from particle-induced bushing wear is an important concern when considering mid- to long-term survivability of the implants, and this is of particular importance for younger patients undergoing total elbow arthroplasty, especially for posttraumatic conditions. Newer bearing designs have recently been created to address the potential issues related to polyethylene wear, including increasing the amount of polyethylene in the bushing as well as designs with conforming polyethylene and metallic-bearing surfaces. The implant described in the Techniques section uses a novel vitamin E highly cross-linked ultra-high-molecular-weight polyethylene bearing to prevent metal-to-metal contact and is designed to have improved polyethylene wear characteristics.Failure of the locking mechanisms used to link ulnar and humeral components in total elbow arthroplasty hasbeen reported for several implant designs.3,10 The implant described in the Techniques section employs a novel locking mechanism designed to reduce the potential for locking mechanism failure.Sequence and Timing of Total Elbow Arthroplasty in the Patient with Polyarticular InvolvementBecause RA typically affects multiple joint articulations, the timing of elbow arthroplasty should be considered with regard to the need for arthroplasties of other joints.In general, the most disabling articulation should be addressed first. In the case of equivocal involvement in the elbow and a lower extremity joint in which arthroplasty is planned, the surgeon must consider the postoperative effects of surgery and plan accordingly.If total elbow arthroplasty is performed first, at least 3 to 6 months should pass before lower extremityreconstruction is performed to allow adequate healing of the elbow. If the lower extremity will be addressed first, total elbow arthroplasty should be delayed until assistive ambulatory devices, which may put strain on the elbow, are no longer required.Patients with total elbow arthroplasty should not bear weight with crutches. A platform walker may be used, provided it does not increase strain on the elbow. This may be achieved by raising the walker's arm rest to an appropriate height such that when the forearm is placed onP.921the arm rest, the elbow may not be extended beyond 90 degrees of flexion.Assessment of the Cervical SpineBecause nearly 90% of patients with RA have cervical spine involvement, approximately 30% of whom have significant subluxation, the cervical spine must be evaluated before any surgery in which intubation is planned.Cervical spine radiographs should be routinely obtained.If patients have neck pain, decreased range of motion, myelopathic symptoms, or radiographic evidence of instability, a magnetic resonance imaging (MRI) study should be ordered with concomitant referral to a spine surgeon to consider addressing the cervical spine pathology before elbow surgery.Temporary Cessation of Medications before Total Elbow ArthroplastyTNF inhibitors affect the immune system and have been found to increase the risk of developing a prosthetic joint infection.In general, anti-TNF agents are typically stopped for a period of time preoperatively based on the half-life of the specific drug and for about 2 weeks after surgery to reduce the risk of perioperative morbidity.Methotrexate is generally continued in the perioperative period. Fewer complications, infections, and flares have been reported when methotrexate is continued perioperatively versus discontinuing it.Patients on chronic NSAIDs should stop taking those medications approximately 2 weeks before surgery to reduce the risk of increased bleeding.For patients on chronic steroids, stress-dose steroids may be required perioperatively.Communications with the patient's rheumatologist and the anesthesiologist are imperative to coordinate these efforts.
POSITIONING
Intravenous antibiotics are administered 30 to 60 minutes before the incision.The patient is placed in a supine position on the operating table with a rolled towel under the ipsilateral scapula. The arm is placed across the chest, and another rolled towel is placed under the elbow to support the arm.The entire operative extremity and shoulder girdle is prepared and draped; a sterile tourniquet is placed. An Ioban drape is placed circumferentially over all exposed skin.The arm is exsanguinated and the tourniquet inflated.
APPROACH
Multiple exposures, including triceps-on approaches, may be used to perform total elbow arthroplasty. The Bryan-Morrey approach (triceps-anconeus “slide”) provides excellent exposure and is particularly useful for surgeons with limited experience in triceps-sparing approaches. The Bryan-Morrey approach is described in thefollowing text.
TECHNIQUES
INCISION AND EXPOSURE

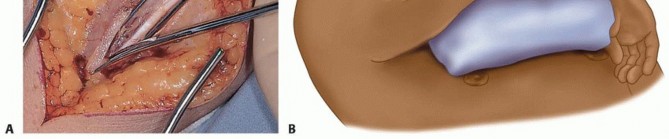
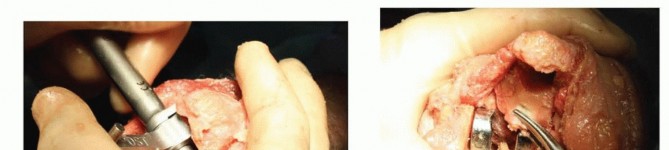
TECH FIG 1 • A,B. The ulnar nerve is identified along the medial border of the triceps, and a vessel loop is placed.(continued)
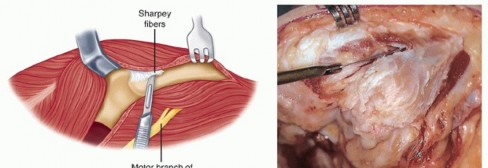
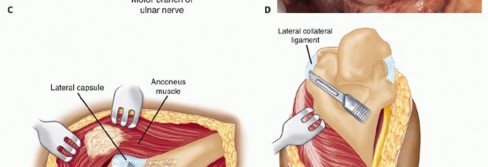
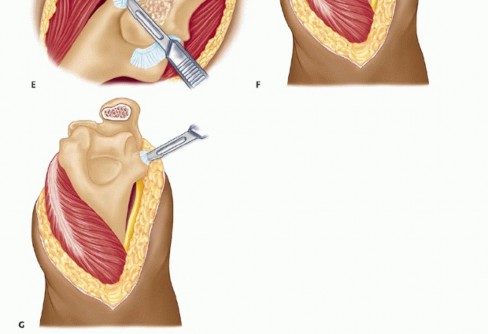
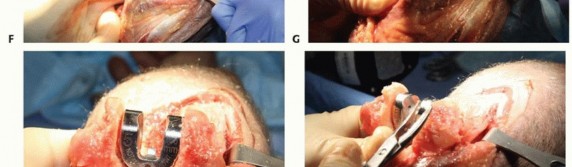
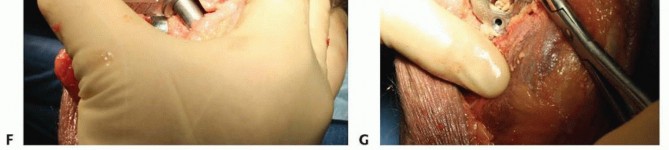
TECH FIG 1 •(continued)C,D. Under tension, the medial and ulnar border of the triceps (C) and the anconeus (D) are incised from their insertions into the olecranon. E. The fibers of the extensor mechanism are further reflected laterally. F. The extensor mechanism is slid lateral to the lateral condyle. G. The medial collateral ligament is released to give the elbow maximal motion and to facilitate complete exposure of the ulnohumeral joint.




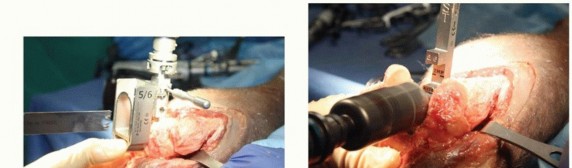
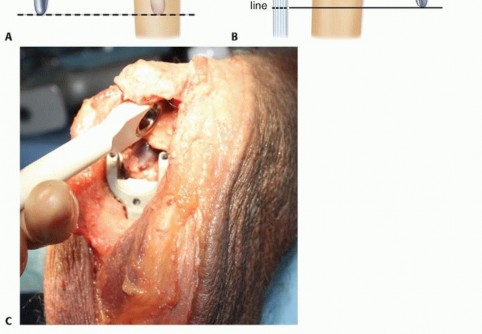
TECH FIG 2 • A. Following trochlear resection with an oscillating saw. B. A burr is used to enter the roof of the olecranon. C. The humeral awl reamer is used to identify the medullary canal. D. Progressive humeral canal rasping is performed up to the desired size and fit. E. The humeral canal rasp is seated so that the solid line matches the axis of flexion.(continued)
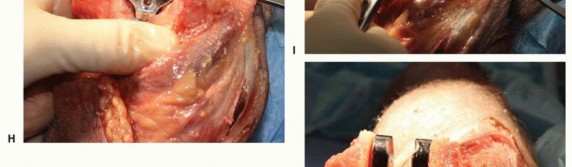

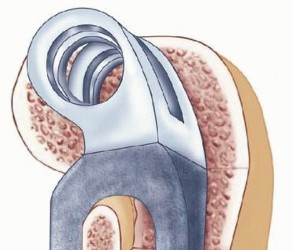
TECH FIG 2 •(continued)F. The humeral cut guide is placed and secured, and an oscillating saw is used to make vertical cuts. G. The trephine stabilizer is fully seated in the canal, and the trephine saw is advanced until it reaches the depth stop. H. The humeral provisional is fully seated. I. A rongeur is used to remove excess bone from the condyle distal to the provisional. J. After resection, the humeral provisional is flush with the distal aspect of the humeral condyles.
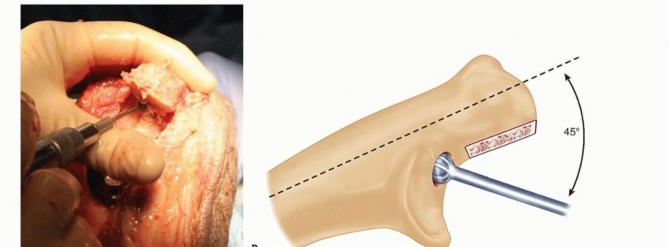


TECH FIG 3 • A,B. The olecranon tip is resected, and a high-speed burr is used to open the ulnar medullary canal at the base of the coronoid. C. The flexible, solid, and cannulated ulnar awl reamers are progressively advanced prior to rasping. The surgeon's hand is placed over the ulnar shaft to guide aiming of the reamers and rasps down the center of the canal. D,E. The pilot ulnar rasp is advanced until the center of the rasp matches the center of the sigmoid notch.(continued)
TECH FIG 3 •(continued)F. The ulnar clearance template is rotated around the sigmoid notch. Any excess bone noted when scoring the surface of the bone is then excised. G. The tip of the coronoid is removed to eliminate impingement and improve flexion.




TECH FIG 4 • A,B. A trial reduction of the components is performed and range of motion is assessed to evaluate for bony impingement.

TECH FIG 5 • A,B. Separate cementing of the humeral and ulnar medullary canals is recommended. C. The ulnar stem inserter is used to prevent scratching of the ulnar component while fully seating the implant.

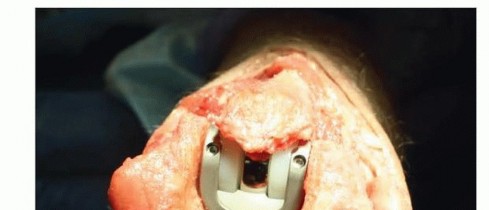
TECH FIG 6 • The humeral component is inserted to the optimal depth that allows proper articulation with the ulnar component.
ASSEMBLY AND IMPACTION


TECH FIG 7 • A. The ulnar-bearing assembly tool is squeezed until significant resistance is felt to attach the ulnar bearing. There is no audible click. B. The articulation inserter is applied and squeezed until resistance is felt and the bearings are seated. There is no audible click with this maneuver.(continued)

TECH FIG 7 •(continued)C. Linked components after the humeral screws are tightened.
TRICEPS REATTACHMENT


TECH FIG 8 • Cruciate (A,B) and transverse (C) drill holes are placed in the ulna for triceps reattachment on a Coonrad-Morrey total elbow replacement. The repair for the Nexel total elbow arthroplasty is identical to this repair when the Bryan-Morrey approach is performed.(continued)


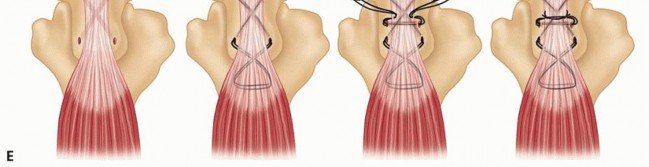
TECH FIG 8 •(continued)D. Planned triceps repair. E. Suture is passed through the proximal ulna and then woven through the triceps tendon before being tied together.
Ulnar Nerve Transposition and Wound Closure
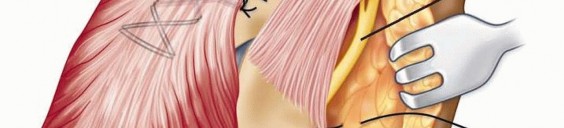
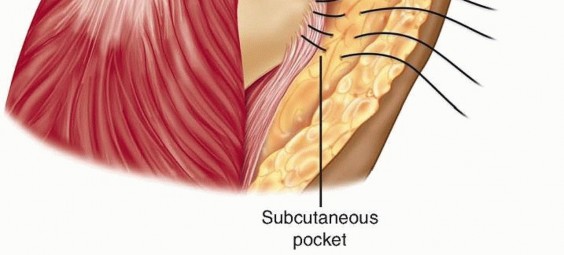
The protected nerve is in the subcutaneous tissue pocket previously created, and dermal sutures are placed to protect and secure the nerve (TECH FIG 9).
Wounds are closed in layers, and a drain is placed. Staples are used to close the skin.
An anterior splint is placed with the elbow in full extension, making sure to adequately pad the anterior aspect of the splint both proximally and distally to prevent skin breakdown.
Ulnar Nerve Transposition and Wound Closure TECH FIG 9 • The ulnar nerve is transposed into the subcutaneous tissue of the medial epicondylar region and secured with sutures in the dermal layer. P.931
PEARLS AND PITFALLS

POSTOPERATIVE CARE
Postoperatively, the anteriorly placed splint maintains the elbow in full extension for about 24 to 36 hours. The elbow is strictly elevated overnight and on postoperative day 1.The drain is removed on postoperative day 1 or when output is less than 30 mL in an 8-hour period.After splint removal, open-chain active-assisted range of motion is allowed. A formal physical therapy consultation is not usually required.The patient is restricted to no pushing and no overhead activities for 3 months to protect the triceps. In addition, no repetitive lifting of objects heavier than 5 pounds and no lifting greater than 10 pounds in a single event is recommented to maximize the survivorship of the implant.
OUTCOMES

FIG 2 • A,B. A 66-year-old female with long-standing RA and Mayo grade IV changes.(continued)
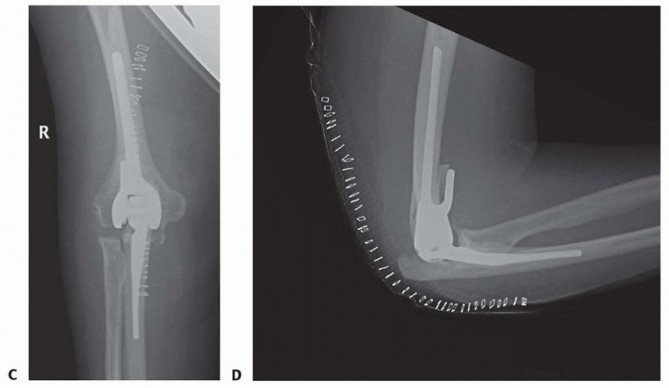
FIG 2 •(continued)C,D. Postoperative radiographs following Nexel total elbow arthroplasty. The prosthetic survival rate was 92.4% at 10 years of follow-up, thus approaching the success of lower extremity arthroplasty.Total elbow arthroplasty for JRAConnor and Morrey1 reported 87% good or excellent results on 19 patients (24 elbows) followed for a mean of 7.4 years.The mean improvement in the Mayo Elbow Performance Score was 59 points, 96% had little or no pain, and there was no evidence of loosening in any prostheses at the latest follow-up.The mean flexion-extension arc of motion improved by only 27 degrees (from 67 to 90 degrees) in this study, which is reflective of the severe soft-tissue contractures associated with JRA.
COMPLICATIONS
InfectionAseptic loosening Mechanical failureShort term Long termUlnar nerve injuryTriceps weakness or avulsion Ulnar component fracture Ulnar fractureWound healing problems
REFERENCES
- Connor PM, Morrey BF. Total elbow arthroplasty in patients who have juvenile rheumatoid arthritis. J Bone Joint Surg Am 1998;80(5): 678-688.
- Day JS, Baxter RM, Ramsey ML, et al. Characterization of wear debris in total elbow arthroplasty. J Shoulder Elbow Surg 2013;22: 924-931.
- Figgie MP, Su EP, Kahn B, et al. Locking mechanism failure in semiconstrained total elbow arthroplasty. J Shoulder Elbow Surg 2006;15: 88-93.
- Gill DR, Morrey BF. The Coonrad-Morrey total elbow arthroplasty in patients who have rheumatoid arthritis. A ten- to fifteen-year followup study. J Bone Joint Surg Am 1998;80(9):1327-1335.
- Horiuchi K, Momohara S, Tomatsu T, et al. Arthroscopic synovectomy of the elbow in rheumatoid arthritis. J Bone Joint Surg Am 2002;84-A(3):342-347.
- Kelly EW, Coghlan J, Bell S. Five- to thirteen-year follow-up of the GSB III total elbow arthroplasty. J Shoulder Elbow Surg 2004;13: 434-440.
- Little CP, Graham AJ, Karatzas G, et al. Outcomes of total elbow arthroplasty for rheumatoid arthritis: comparative study of three implants. J Bone Joint Surg Am 2005;87(11):2439-2448.
- Morrey BF, Adams RA. Semiconstrained arthroplasty for the treatment of rheumatoid arthritis of the elbow. JBone Joint Surg Am 1992;74(4):479-490.
- Rymaszewski LA, Mackay I, Amis AA, et al. Long-term effects of excision of the radial head in rheumatoid arthritis. J Bone Joint Surg Br 1979;66(1):109-113.
- Wright TW, Hastings H. Total elbow arthroplasty failure due to overuse, C-ring failure, and/or bushing wear. J Shoulder Elbow Surg 2005;14:65-72.
