Introduction to Rheumatoid Thumb Deformities
Rheumatoid arthritis (RA) profoundly affects the hand and wrist, with the thumb being involved in up to 70% of patients. Because the thumb is responsible for approximately 40% to 50% of overall hand function, preserving its stability, mobility, and painless pinch is a primary objective in rheumatoid reconstructive surgery. The metacarpophalangeal (MCP) joint is frequently the epicenter of pathologic changes, leading to predictable patterns of collapse.
The most common deformity encountered is the Nalebuff Type I (boutonnière) deformity. This is characterized by MCP joint flexion and secondary interphalangeal (IP) joint hyperextension. The pathogenesis begins with aggressive synovial hypertrophy within the MCP joint, which distends the dorsal capsule and attenuates the insertion of the extensor pollicis brevis (EPB) tendon.
As the EPB becomes detached and retracts proximally, the extensor hood stretches. This allows the extensor pollicis longus (EPL) tendon to subluxate ulnarly and volarly. Concurrently, the intrinsic muscles—specifically the abductor pollicis brevis (APB) and the adductor pollicis—migrate volarly below the axis of rotation of the MCP joint. Consequently, these muscles transition from being stabilizers to active flexors of the MCP joint, exacerbating the flexion deformity.
Clinical Pearl: The key to successful rheumatoid thumb reconstruction lies in addressing the entire kinematic chain. The status of the carpometacarpal (CMC) and IP joints must be meticulously evaluated before intervening at the MCP joint. A fused or stiff IP joint often necessitates motion preservation (arthroplasty) at the MCP joint to maintain functional dexterity.
Indications and Patient Selection
Surgical intervention at the thumb MCP joint is dictated by the severity of articular destruction, the flexibility of the deformity, and the condition of the adjacent joints.
- Soft Tissue Reconstruction (Synovectomy and Tendon Rebalancing): Indicated for early-stage disease where the MCP joint deformity is passively correctable, and radiographic evidence shows preserved articular cartilage with minimal erosive changes. The Inglis et al. technique is the gold standard for this stage.
- Silicone Implant Arthroplasty: Indicated for older, lower-demand patients with advanced joint destruction but adequate bone stock and restorable capsuloligamentous stability. It is particularly useful when the IP joint is severely damaged and requires arthrodesis, as preserving MCP motion becomes critical.
- Arthrodesis: The most predictable and durable procedure for severe, fixed deformities with profound bone loss or gross collateral ligament instability. It provides a stable post for pinch grip and is highly recommended for high-demand patients or when soft tissue reconstruction is doomed to fail.
Surgical Anatomy and Biomechanics
A thorough understanding of the dorsal apparatus of the thumb is mandatory. The EPB inserts into the dorsal base of the proximal phalanx and acts as the primary extensor of the MCP joint. The EPL inserts into the base of the distal phalanx, extending the IP joint, but also contributes to MCP extension through its connections to the dorsal hood.
The intrinsic muscles (APB radially and adductor pollicis ulnarly) send transverse fibers to the extensor mechanism. In the rheumatoid thumb, the attenuation of the dorsal capsule allows these intrinsics to slip volarly. Surgical reconstruction must not only repair the EPB but also dorsally advance the intrinsics to restore their mechanical advantage as MCP joint stabilizers.
Surgical Technique: Soft Tissue Reconstruction (Inglis et al.)
The Inglis technique focuses on radical synovectomy, relocation of the displaced intrinsic muscles, and reattachment of the EPB to restore active MCP extension.
1. Positioning and Incision
The patient is positioned supine with the arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the upper arm.
Make a longitudinal incision over the dorsum of the metacarpophalangeal joint. The incision should extend from the middle of the proximal phalanx to the midshaft of the first metacarpal.
Surgical Warning: Meticulous blunt dissection in the subcutaneous tissues is critical to identify and protect the terminal branches of the superficial radial nerve. Injury to these branches can result in debilitating neuromas.
2. Exposure and Assessment of the Extensor Mechanism
Deepen the dissection to expose the extensor apparatus. Observe the extensor pollicis brevis (EPB) to determine the extent of its pathology. In advanced Nalebuff Type I deformities, the EPB will have become detached from the proximal phalangeal bone and retracted proximally.
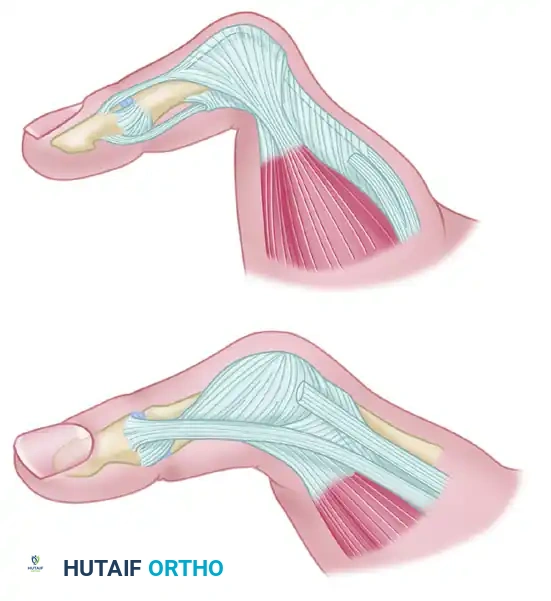
Figure A: Metacarpophalangeal joint of the thumb demonstrating extensive tendon damage. Following the rupture of the EPB insertion into the base of the proximal phalanx and its subsequent proximal retraction, the extensor hood becomes severely attenuated. This allows the abductor pollicis brevis and extensor pollicis longus to migrate volarward, dropping below the center of rotation of the MCP joint.
3. Tendon Dissection and Hood Release
Split the extensor hood longitudinally between the extensor pollicis longus (EPL) and the extensor pollicis brevis (EPB).
To mobilize the volarly displaced intrinsic muscles, detach the abductor pollicis brevis from the extensor hood on the radial side. Proceed to detach the adductor pollicis from the ulnar side. This release is crucial for correcting the flexion deforming forces acting on the joint.
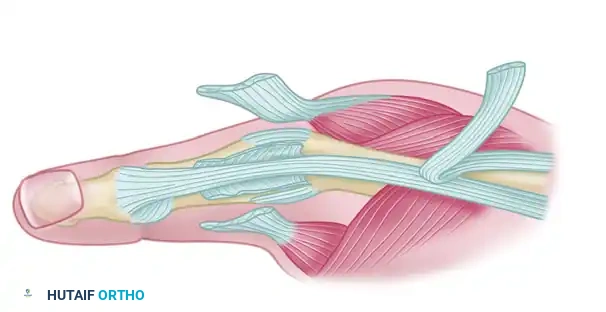
Figure B: The insertions of the extensor pollicis brevis and the adductor pollicis are meticulously dissected free from the remaining attenuated extensor tendon hood.
4. Joint Exposure and Synovectomy
Retract the remaining tendon structures laterally to fully expose the dorsal capsule and the underlying synovium.
Perform a meticulous and radical synovectomy. It is imperative to preserve the radial and ulnar collateral ligaments to maintain the coronal stability of the MCP joint. Excision of all synovium within the joint is often facilitated by gently flexing the MCP joint, which opens the dorsal joint space and allows access to the volar pouch.
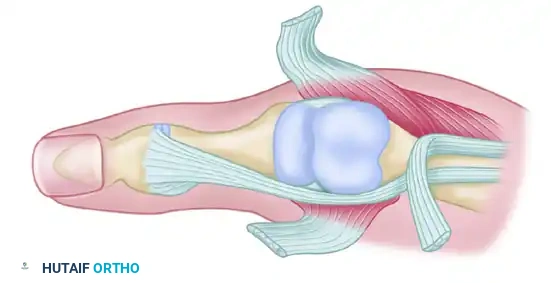
Figure C: Synovectomy is greatly facilitated by the flexion of the proximal phalanx. Note that the collateral ligaments are carefully preserved to prevent postoperative instability.
5. Skeletal Preparation and Tendon Reattachment
Prepare the dorsal base of the proximal phalanx for tendon reinsertion. Drill a small hole for sutures on each side of the dorsum of the base of the proximal phalanx. Make a larger central hole just distal to and between these suture holes to serve as the insertion point for the extensor pollicis brevis tendon.
Advance the EPB and attach it into the bony trough using non-absorbable sutures (e.g., 3-0 or 4-0 braided polyester) passed through the drill holes. The EPB must be attached with sufficient tension to maintain full extension of the metacarpophalangeal joint.
Next, reattach the abductor pollicis brevis and adductor pollicis dorsally to the reconstructed extensor mechanism. This dorsal advancement restores the balance of the joint, converting these muscles back into dynamic stabilizers rather than flexors.
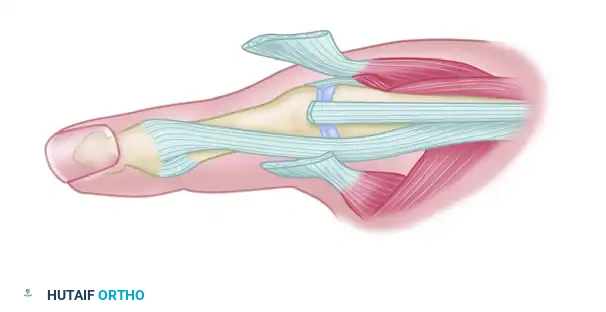
Figure D: Attachment of the extensor pollicis brevis tendon into the base of the proximal phalanx. If the EPB is severely degenerated or cannot be advanced sufficiently, the tendon of the extensor indicis proprius (EIP) can be transferred from the index finger and inserted into the base of the proximal phalanx to restore extension.
6. Skeletal Stabilization
To protect the tendon repairs and maintain the joint in the corrected position, the metacarpophalangeal joint must be temporarily immobilized. Maintain the MCP joint in 0 degrees of extension by driving two transfixing Kirschner wires (typically 0.045-inch) across the joint.
Alternative Interventions: Arthroplasty and Arthrodesis
When the articular cartilage is destroyed, soft tissue reconstruction alone will fail. The surgeon must choose between arthroplasty and arthrodesis.
Silicone Implant Arthroplasty
Arthroplasty may be preferable to an attempt to maintain metacarpophalangeal joint motion if the interphalangeal joint is sufficiently damaged to require arthrodesis. A thumb with both the MCP and IP joints fused can be highly functional but lacks fine dexterity.
For a successful silicone implant arthroplasty (e.g., Swanson implant):
* Bone Stock: Sufficient bone stock must be present to allow stable seating of the implant stems within the medullary canals of the metacarpal and proximal phalanx.
* Ligamentous Integrity: It must be possible to obtain reasonable joint stability with the restoration or preservation of capsuloligamentous structures. The implant acts as a dynamic spacer, not a stabilizing hinge; therefore, the collateral ligaments must be competent or reconstructable.
Pitfall: Silicone implant arthroplasty carries specific long-term risks, including implant breakage, dislocation, and particulate synovitis (silicone reactive disease). Consequently, implant arthroplasty is generally reserved for selected older patients with low functional demands on their thumbs.
Resection Arthroplasty
Resection arthroplasty, which was popular in the past, involves excising the metacarpal head without placing an implant. This technique does not provide a stable metacarpophalangeal joint and often results in a weak, shortened, and unstable thumb. It has largely been abandoned in modern reconstructive orthopedics in favor of arthrodesis or implant arthroplasty.
Metacarpophalangeal Arthrodesis
If the restoration of joint stability is doubtful, or if the patient is young and high-demand, arthrodesis is the more predictable and reliable procedure.
The MCP joint is typically fused in:
* 10 to 15 degrees of flexion.
* Slight pronation (to allow pulp-to-pulp pinch with the index finger).
* 10 to 15 degrees of abduction.
Fixation can be achieved using crossed Kirschner wires, tension band wiring, or miniature plate and screw constructs, depending on bone quality and surgeon preference.
Postoperative Care and Rehabilitation
The success of the Inglis soft tissue reconstruction relies heavily on strict adherence to the postoperative protocol to allow tendon healing while preventing stiffness.
- Immediate Postoperative Phase (0-2 Weeks): Following wound closure, a bulky, non-compressive dressing is applied, reinforced with a volar thumb spica splint. The thumb is immobilized with the MCP joint in full extension and the CMC joint in palmar abduction. The IP joint is left free to allow early active motion, which prevents EPL adhesions.
- First Clinic Visit (2 Weeks): The initial splint and skin sutures are removed. The surgical site is inspected for signs of infection or necrosis. A custom thermoplastic thumb spica splint is fabricated, maintaining the MCP joint in extension.
- Pin Removal Phase (4 Weeks): The transfixing Kirschner wires are removed in the clinic at approximately 4 weeks postoperatively.
- Mobilization Phase (4-7 Weeks): Following K-wire removal, a structured rehabilitation program begins. The patient initiates active range of motion (ROM) exercises for the MCP joint under the guidance of a certified hand therapist. Splinting is continued at all times except during these dedicated exercise periods for another 2 to 3 weeks.
- Strengthening Phase (7+ Weeks): The splint is gradually weaned during the day. Gentle strengthening exercises, focusing on pinch and grip, are introduced. Heavy lifting and forceful pinching should be avoided for at least 10 to 12 weeks to ensure complete maturation of the tendon transfers.
Complications
- Recurrent Deformity: The most common complication of soft tissue reconstruction in RA is the recurrence of the flexion deformity. This usually results from progressive rheumatoid disease, failure of the tendon repair, or unrecognized CMC joint disease leading to secondary MCP collapse.
- Pin Tract Infection: Meticulous pin care is required while the K-wires are in place. Superficial infections usually resolve with oral antibiotics and pin removal.
- Stiffness: Over-tensioning of the EPB or prolonged immobilization can lead to a stiff MCP joint in extension. While a stiff, straight MCP joint is highly functional (akin to an arthrodesis), it may limit fine motor tasks if the IP joint is also compromised.
- Nerve Injury: Neuroma of the superficial radial nerve branches can cause severe, intractable pain, highlighting the need for careful dorsal dissection.
