DEFINITION
Osteoarthritis, or more appropriately osteoarthrosis, is a common problem in the hand. The trapeziometacarpal joint is commonly affected, second in frequency only to the distal interphalangeal joint. Trapeziometacarpal joint osteoarthritis, however, can be much more disabling secondary to pain and weakness of grip and pinch strength.The surgical management of symptomatic basilar joint arthrosis varies according to the anatomy, radiographic staging, intraoperative confirmation of disease stage, and patient requirements.
ANATOMY
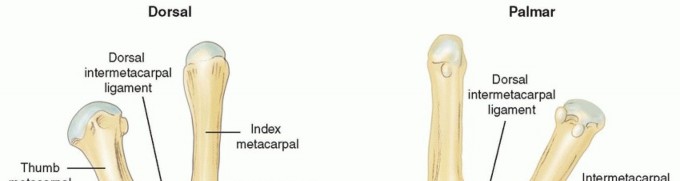
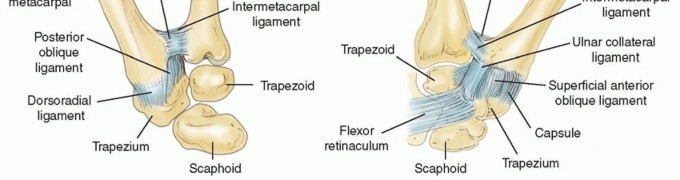
FIG 1 • CMC thumb joint.
PATHOGENESIS
The pathogenesis of CMC joint arthrosis is multifactorial, involving biochemical and biomechanical influences. The synovial fluid within the joints contains cytokines that invariably play a role in cartilage degradation anddecreased ability to withstand the loads generated at the joint during daily activities.9 Although not clearly delineated, estrogen or estrogen-related compounds probably play some protective role, which may explain the increased incidence of osteoarthritis in postmenopausal women (10 to 15:1).The palmar or anterior oblique ligament (AOL), or so-called beak ligament, has been shown to be the most important stabilizing ligament of the thumb. Degeneration or functional incompetence of this ligament leads to laxity, abnormal translation of the metacarpal on the trapezium, increased shear forces, and resultant abnormal wear patterns. This eburnation of the articular cartilage initially occurs along the palmar aspect ofthe joint.10 With progression of disease, osteophytes develop and eburnation progresses throughout the entire joint surface.Osteoarthrosis can also develop from damage and disruption of the articular cartilage. Any fracture through the metacarpal or trapezium joint surfaces yield arthrosis. Anatomic restoration of the joint surface can minimize this sequela but cannot eliminate the risk entirely. Paradoxically, however, a Bennett fracture may protect the joint from the development of osteoarthritis, assuming subluxation has been treated, by virtue of consequential unloading of the volar aspect of the joint.
NATURAL HISTORY
P.1069Arthrosis of the thumb CMC joint begins along the palmar aspect of the metacarpal secondary to laxity of the AOL. As the process progresses, the entire base of the metacarpal and distal trapezium becomes involved.There is initial eburnation of the cartilage, which progresses to osteophyte formation. As the disease continues, the TM assumes an adducted position and the metacarpophalangeal (MCP) joint may compensate by becoming hyperextensile, resulting in varying degrees of MCP joint hyperextension.The disease can involve all the trapezial articulations as well as the scaphotrapezoidal joint.15
PATIENT HISTORY AND PHYSICAL FINDINGS
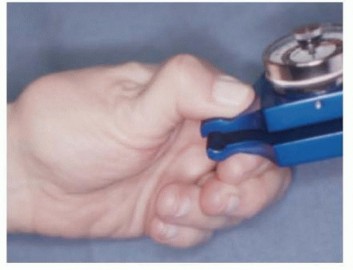
FIG 2 • Dynamic collapse of the thumb on key pinch testing.
IMAGING AND OTHER DIAGNOSTIC STUDIES
FIG 3 • Preoperative posteroanterior (PA) stress and lateral radiographs of the right thumb. P.1070Stage V: stage IV appearance with the addition of narrowing or osteophytes in the scaphotrapezoid jointThe scaphotrapezoid joint is not specifically addressed in this system and may be difficult to assess radiographically, but it should always be assessed clinically during operative intervention because it may be a source of continued pain.
DIFFERENTIAL DIAGNOSIS
De Quervain diseaseTrigger thumb or stenosing tenosynovitis Carpal tunnel syndrome
NONOPERATIVE MANAGEMENT
Most patients with symptomatic thumb CMC joint arthrosis benefit from a trial of conservative therapy, which may include corticosteroid injection, thenar isometric strengthening exercises, and splinting.Although this will not eliminate the problem or alter the underlying disease process, conservative treatment often reduces symptoms, at least transiently, allowing the patient the opportunity to plan for surgical treatment at the most opportune time.Differential injection of steroids can also be helpful to assess how much of a patient's symptoms are coming from the thumb CMC joint versus other areas (carpal tunnel or de Quervain disease).
SURGICAL MANAGEMENT
The indications for surgical intervention for symptomatic thumb basilar joint arthrosis include pain and weakness.There are multiple procedures used to treat symptomatic CMC thumb arthritis, many of which have merit depending on the extent of arthritic involvement.Pantrapezial involvement contraindicates the use of arthrodesis or implant arthroplasty, in particular, because of the risk of incomplete pain relief.Arthrodesis may be preferable in younger, high-demand patients such as laborers.Resection arthroplasty can be performed with ligament reconstruction or without (hematoma distraction arthroplasty).5,7The flexor carpi radialis (FCR) and abductor pollicis longus (APL) are most commonly used when performing “suspensionplasty.”
PREOPERATIVE PLANNING
Consideration should be given to the age of the patient and the demands placed on the thumb. Dynamic collapse of the MCP joint during key pinch necessitates MCP fusion or capsulodesis.Intraoperative evaluation of the scaphotrapezotrapezoidal (STT) joint is critical to ensure adequate pain relief after surgery. Thus, hemitrapeziectomy is rarely performed once the decision to proceed with conventional resection arthroplasty is made. If retention of the proximal trapezium is elected because of the absence of STT disease, Artelon resurfacing or joint arthroplasty may be elected.Intraoperative assessment of the scaphotrapezoidal joint is recommended, and if changes exist, a 2- to 3-mm resection of the proximal trapezoid is performed.15 Care is taken not to injure the capitate.Suspensionplasty ensures stability of the TM during pinch and grip, resisting the cantilever bending forces that will potentially lead to subluxation and proximal migration compared to trapeziectomy alone.Intermediate-term outcome of the hematoma distraction arthroplasty suggests that this procedure may have a role in providing excellent pain relief in well-selected patients for whom grip strength is a less important issue.5
POSITIONING
The patient is supine, and the involved hand and arm are supported by a hand table.
APPROACH
Trapezium excision and ligament reconstruction and suspensionplasty can be performed using the Wagner (volar) approach or a dorsal approach. I prefer the dorsal approach except when performing an Eaton ligament reconstruction, in which case a volar approach is used. I have modified my technique since performing the ligament reconstruction and tendon interposition (LRTI) arthroplasty exclusively during the first 10 years ofpractice.12,14Over the past 5 years, I have performed a suspensionplasty using a distally based slip of the APL tendon, which obviates the need for a bony channel. This is a variation of other suspensionplasty techniques.8,11,16 In addition, I no longer pin the joint or interpose tissue into the space remaining after trapezial resection. Theprocedure is performed more expeditiously and seems to be associated with equivalent outcomes.13P.1071
TECHNIQUES
Ligament Reconstruction and Tendon Interposition Arthroplasty Using the Flexor Carpi Radialis Tendon
Ligament Reconstruction and Tendon Interposition Arthroplasty Using the Flexor Carpi Radialis Tendon
INCISION AND SUPERFICIAL DISSECTION
A triradiate is drawn before the tourniquet is inflated to allow palpation of the radial pulse in the vicinity of the anatomic snuffbox; this typically identifies the scaphotrapezial joint.When a substantial shoulder sign (prominence associated with dorsal subluxation of the proximal phalanx trapezium) exists, it can be difficult to identify the TM joint. In these cases, palpation of the scaphoid tuberosity is helpful to ensure that the incision is neither too distal nor too proximal.The triradiate incision facilitates dissection of the radial artery off the dorsal capsule; when first extensor compartment release is planned, however, a longitudinal incision may be preferred.At the outset, the radial sensory nerve must be identified and small branches must not be skeletonized or divided. This may cause postoperative radial sensory neuritis and even transient reflex sympathetic dystrophy.Place blunt retractors beneath the extensor pollicis longus (EPL) in a dorsal and ulnar position and the APL radially and volarly.The radial artery courses within this interval, and deep perforators to the dorsal capsule must be coagulated and divided so the artery can be retracted dorsally and ulnarly.
CAPSULAR INCISION AND TRAPEZIAL EXCISION
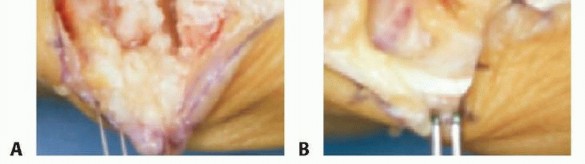
TECH FIG 1 • The base of the metacarpal is resected (A), and the trapezium is excised (B). Cut the trapezium into quadrants, beginning with the limb that parallels the expected course of the FCR tendon. Injury to the tendon during this portion of the procedure is unlikely if the saw is not brought completely through the trapezium.After making perpendicular cuts in the trapezium, place an osteotome and twist it to break apart its four quadrants. Removal of the trapezium in pieces with a rongeur is facilitated by sharp dissection of the remaining capsule, particularly volarly and around loose bodies. Avoid inordinate ripping and pulling with the rongeurs because damage to the underlying capsule can increase postoperative discomfort, particularly where it abuts the carpal tunnel.Remove osteophytic bone between the base of the thumb and index metacarpal so that pain does not accompany key pinch after the procedure. Identify the FCR tendon at the base of the arthroplasty space so it is not injured; remember that the trapezium may encircle the FCR tendon at its volar extent.At this portion of the procedure, I routinely have an assistant place traction on the index and long fingers to allow inspection of the scaphotrapezoidal joint. If there is cartilage fraying or eburnation, a motorized burr or rongeur is used to remove 2 to 3 mm of proximal trapezoid so that, with axial compression applied to the index and long finger metacarpals, there is no contact between the remaining trapezoid and scaphoid (TECH FIG 1B). I do not interpose soft tissue or FCR tendon into the space. Take care not to remove bone from the capitate. Creation of the Bony Channel through the Metacarpal Base
TECH FIG 2 • A tunnel is made at the base of the metacarpal. P.1072
FLEXOR CARPI RADIALIS HARVEST
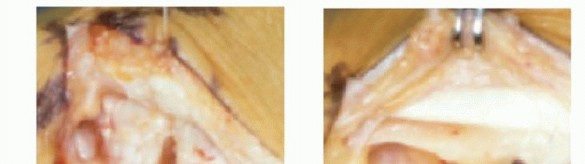
Palpate the FCR tendon at wrist level during passive flexion and extension of the wrist, where it is clearly tendinous. More proximally in the forearm, the tendon becomes less discrete. This generally correlates with the proximal one-third to half of the forearm. At that location, make a 1.5-cm transverse incision.Open the fascia, maximally flex the wrist, and identify the interval between the FCR tendon and muscle. Lift it into the wound via a curved clamp and divide it. Close this wound with 5-0 nylon sutures.Retract the capsular flaps to protect the overlying radial artery dorsally and ulnarly. Place a curved snap beneath the FCR tendon and pull it. This typically delivers the entire tendon into the arthroplasty space.Grasp the tendon at its tip and mobilize it to its insertion at the base of the index metacarpal without violating the small blood vessels that perfuse the tendon insertion itself.If adhesions between the FCR and the volar capsule are not released, the vector of the ligament reconstruction is based more proximally and will not closely simulate the original vector of the beak ligament. This, in my opinion, is a potential cause of early subsidence after ligament reconstruction.Taper the tendon for about 2 to 3 cm so the diameter of the tip of the tendon will easily fit through the bone tunnel via the Carroll tendon passer.Use a 4-0 Vicryl suture on a small needle to purchase the volar capsule for subsequent stabilization of the tendon interposition.If there are rents in the volar capsule, this same suture can be used to repair them, but I no longer am inordinately preoccupied with repairing small tears in the volar capsule because there is little risk of the tendon interposition extruding into the carpal canal or into the base of the metacarpal. Stabilization of the Thumb Metacarpal (Optional) and Flexor Carpi Radialis Tendon Tensioning
TECH FIG 3 • A. The FCR is passed through bony tunnel. B. A hand probe indicates FCR suspensionplasty. Usually, a 0.045- or 0.054-inch wire is used. It begins obliquely at the dorsoradial aspect of the metacarpal and purchases the ulnar carpus.I place the thumb in the “fisted” position as if engaged in key pinch. The TM is suspended at the level of the index metacarpal. Its base should be colinear with the scaphoid articular surface and the thumb tip should rest on the index finger, neither too extended nor flexed at its base.Ideally, this positions the thumb intrinsic muscles optimally on the Blix curve and ensures optimal restoration of pinch strength.Bend the wire external to the skin and cut it.A hand probe or the like is used to take the FCR tendon at the base of the metacarpal and pull it proximally (TECH FIG 3).When pinning has been performed, it should not prevent free excursion of the FCR through the bone channel. Pull the tendon tightly as it exits the dorsum of the TM and suture it to adjacent periosteum and soft tissue with 3-0 Vicryl suture.If pinning is not performed, at this point, ensure that you have suspended the metacarpal at the level of the index CMC joint.The extensor pollicis brevis (EPB) tendon is sutured more radially and divided distally. This completes the EPB tenodesis, rendering it an abductor of the metacarpal as opposed to a potential hyperextender of the MCP joint.Place a second suture slightly more proximal to the tenodesis suture so that the ligament reconstruction is stabilized adequately, and perform tissue interposition.
TISSUE INTERPOSITION (OPTIONAL)
Although Burton's original technique continues to “resurface” the metacarpal base to minimize the chance that interposition material may extrude through the channel, this is unlikely. Studies have suggested that interposition is not a critical element of the procedure if suspension of the metacarpal has beeneffectively executed.4 Furthermore, proximal migration, short of causing scaphometacarpal impingement, appears not to affect the functional outcome.6P.1073In a higher demand patient, however, residual length of the FCR is available for interposition as follows. The tendon is folded into the volar aspect of the arthroplasty space to ensure that it will sink into its depth. From that point distally, the tendon is folded back and forth about four times on a single Keith needle, like ribbon candy.A 4-0 Vicryl suture is used to stabilize each corner of the tendon anchovy, and then a second Keith needle is placed through it, parallel to the first. Apertures in each needle should be volar, the tip of each needle dorsal, and, with the previously placed volar capsular suture, each limb is threaded and the anchovy is slid down and delivered into the arthroplasty space. The two Vicryl limbs are tied, securing the tissue interposition (TECH FIG 4).
CAPSULAR REPAIR AND WOUND CLOSURE
TECH FIG 4 • The tendon anchovy held in place with Vicryl sutures. Place a bulky thumb spica dressing, followed by volar and thumb spica splints. The hand is elevated for 3 or 4 days after surgery.1. Abductor Pollicis Longus Suspensionplasty
INCISION AND DEEP DISSECTION

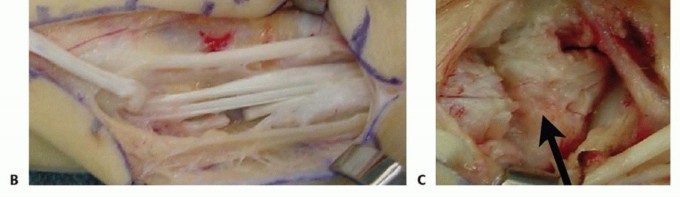
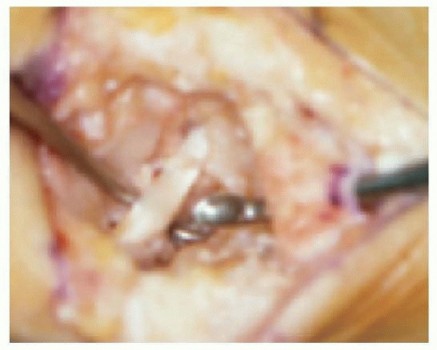
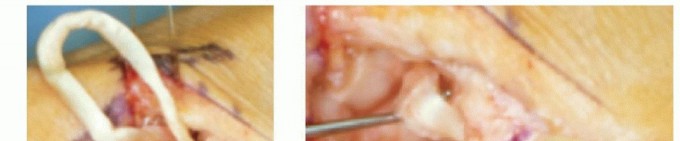
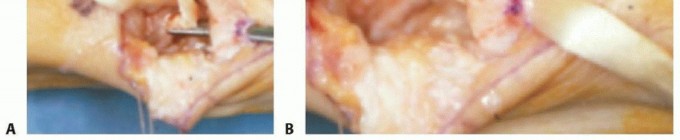
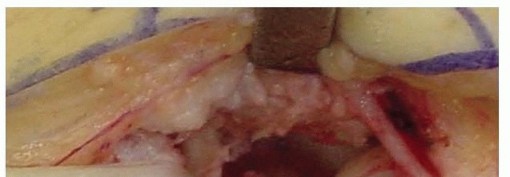
TECH FIG 5 • APL suspensionplasty technique. A. Skin incision. B. Distally based slip of APL. C. Trapezium excision (arrowidentifies the trapezium).At the myotendinous junction of the APL, release the ulnar-most slip of APL and free it to the level of its insertion at the metacarpal base (TECH FIG 5B).Expose the EPL and APL tendons—in between is the capsule of the TM joint.Perform a capsulotomy to expose the trapezium (TECH FIG 5C), which is resected after being cut partially into four fragments with a saw and osteotome.The base of the TM is not squared off; not resecting a small sliver from the metacarpal base may help to preserve the intermetacarpal ligament.P.1074The FCR tendon is visualized in the base of the arthroplasty space. With traction on the index and long fingers, inspect the scaphotrapezoidal joint; if it is arthritic, resect the proximal trapezoid. Creation of the Abductor Pollicis Longus Suspensionplasty Poke the APL slip through the capsule to within the arthroplasty space. Using a right angle clamp, pass it through a slit in the FCR tendon or around the FCR while grabbing some local capsule as well (TECH FIG 6).TECH FIG 6• APL slip is passed through and around FCR (arrow).Position the thumb so that it rests on the index finger in the fisted position—distracted so that the metacarpal base is at the level of the index CMC joint. A Kirschner wire is not placed.Pull the APL slip taut and place a 3-0 Vicryl suture between the APL slip, at the level of the metacarpal base, and the EPB (radially) and the tissue deep to the EPL (ulnarly).
CAPSULAR CLOSURE AND REHABILITATION

|Address MCP ▪ Static laxity is no longer viewed as an absolute indication for capsulodesis joint or fusion. Rather, dynamic collapse during pinch is a relative indication. hyperextensibilityAddress ▪ If proximal trapezoid excision is not performed, pain at this articulation may scaphotrapezoidal persist.diseasePinning is not ▪ Neither pinning for 4 weeks nor tissue interposition is required. Outcomes essential; tissue appear not to be compromised by modest proximal metacarpal migration. interposition is not However, these elements of the procedure do have a role if concern about essential any potential for scaphometacarpal impingement exists.Ensure stability of ▪ The APL should be placed through the FCR or around it and shouldthe APL capture some capsule. This technical point will prevent the APL and TM from suspension sliding proximally along the FCR.||Joint fusion timing ▪ When necessary, concomitant MCP joint fusion should be performed after tendon harvest and passage to avoid thumb manipulation after fusion.|------
POSTOPERATIVE CARE
First monthAt 2 weeks, the patient returns for suture removal, wound inspection, and placement of a fiberglass thumb spica cast that allows full motion of the thumb interphalangeal joint, unless MCP joint fusion has been performed.At 4 weeks, the patient returns again, the Kirschner wire is pulled (if one has been placed), and a forearm-based thumb spica Orthoplast splint is fashioned by the hand therapist.Gentle wrist and thumb MCP joint range-of-motion exercises are initiated as well as thenar isometric exercises. The latter are performed with the thumb in the splint.Month 2At 6 weeks, if the patient is comfortable, gentle pinch and grip strengthening exercises are initiated. By 8 weeks, flexion-adduction and opposition exercises are begun.Month 3By this time, the patient is usually doing well enough that the splint can be discarded. Grip and pinch exercises are typically continued by the patient via a home program.No rigorous attempt is made for the thumb to reach the ring and small finger bases because there is no functional relevance to these activities and they risk stretching theP.1075ligament. In addition, passive range of motion is not a part of the postoperative regimen.During months 3 to 6, the patient is encouraged to use the hand and to push the exercises vigorously. Typically, patients return to normal activities, including golf and tennis.
OUTCOMES
Ligament Reconstruction and Tendon Interposition Arthroplasty Improvements in grip strength typically exceed improvements in key pinch strength. In 1995, Tomaino et al14 noted that key pinch strength took at least 6 years to equal preoperative measurements.At an average follow-up of 9 years (range 8 to 11), these authors14 reported on 24 thumbs in 22 patients and found that average grip strength increased 93%, average key pinch strength increased 34%, and tip pinch strength increased 65% compared with preoperative values.In contrast to many other studies, stress radiographs showed an average subluxation of the metacarpal base of only 11% and subsidence of only 13%. This compares favorably with the radiographic outcomesafter the hematoma distraction arthroplasty.5,7Even in series in which proximal migration of the metacarpal base averaged greater than 20%, there has been no significant correlation between maintenance of arthroplasty space height and objective orsubjective clinical outcome (FIG 4).6
ABDUCTOR POLLICIS LONGUS SUSPENSIONPLASTY

FIG 4 • Postoperative lateral radiograph shows arthroplasty space 1 year after surgery. In summary, APL suspensionplasty is a simple yet effective treatment alternative for basal joint arthritis. The suspensionplasty technique uses our current understanding of the forces involved during pinch andgrip2 as well as the role of normal ligamentous anatomy. APL suspensionplasty appears at least in terms of early outcome to have very similar results to those which have been reported using the LRTI technique.
COMPLICATIONS
One cause of unsatisfactory outcome after basal joint arthroplasty is residual pain because of failure toaddress scaphotrapezial or scaphotrapezoidal disease.15 Routine complete excision of the trapezium certainly precludes the scaphotrapezial joint pain. Routine intraoperative observation and treatment of the scaphotrapezoidal disease by partial excision of the proximal trapezoid prevents scaphotrapezoidal jointpain.15Unaddressed instability of the MCP joint can also impair functional outcome after ligament reconstruction. During lateral pinch, MCP joint hyperextension causes reciprocal deformity more proximally, imposing metacarpal adduction and stressing the reconstructed ligament. Accordingly, early identification of hyperextension in excess of 30 degrees during key pinch should prompt stabilization to protect the integrity of the basal joint ligament reconstruction. Even with a sound ligament reconstruction and appropriate stabilization of the MCP joint, it is theoretically possible to develop recurrent laxity at the basal joint due to stretching of the ligament reconstruction.
REFERENCES
- Bettinger PC, Linscheid RL, Berger RA, et al. An anatomic study of the stabilizing ligaments of the trapezium and trapeziometacarpal joint. J Hand Surg Am 1999;24(4):786-798.
- Cooney WP III, Chao EY. Biomechanical analysis of static forces in the thumb during hand function. J Bone Joint Surg Am 1977;59(1): 27-36.
- Esenwein P, Hoigne D, Zdravkovic V, et al. Resection, interposition and suspension arthroplasty for treatment of basal joint arthritis of the thumb: a randomized and prospective comparison of techniques using the abductor pollicis longus and the flexor carpi radialis tendon [in German]. Handchir Mikrochir Plast Chir 2011;43(5): 289-294.
- Gerwin M, Griffith A, Weiland AJ, et al. Ligament reconstruction basal joint arthroplasty without tendon interposition. Clin Orthop Relat Res 1997;(342):42-45.
- Gray KV, Meals RA. Hematoma and distraction arthroplasty for thumb basal joint osteoarthritis: minimum 6.5-year follow-up evaluation. J Hand Surg Am 2007;32(1):23-29.
- Kriegs-Au G, Petje G, Fojtl E, et al. Ligament reconstruction with or without tendon interposition to treat primary thumb carpometacarpal osteoarthritis. A prospective randomized study. J Bone Joint Surg Am 2004;86-A(2):209-218.P.1076
- Kuhns CA, Emerson ET, Meals RA. Hematoma and distraction arthroplasty for thumb basal joint osteoarthritis: a prospective, single-surgeon study including outcomes measures. J Hand Surg Am 2003;28(3):381-389.
- Nylén S, Juhlin LJ, Lugnegard H. Weilby tendon interposition arthroplasty for osteoarthritis of the trapezial joints. J Hand Surg Br 1987;12(1):68-72.
- Pellegrini VD Jr. Pathomechanics of the thumb trapeziometacarpal joint. Hand Clin 2001;17:175-184.
- Pellegrini VD Jr, Olcott CW, Hollenberg G. Contact patterns in the trapeziometacarpal joint: the role of the palmar beak ligament. J Hand Surg Am 1993;18(2):238-244.
- Sigfusson R, Lundborg G. Abductor pollicis longus tendon arthroplasty for treatment of arthrosis in the first carpometacarpal joint. Scand J Plast Reconst Hand Surg 1991;25:73-77.
- Tomaino MM. Ligament reconstruction tendon interposition arthroplasty for basal joint arthritis. Rationale, current technique, and clinical outcome. Hand Clin 2001;17:207-221.
- Tomaino MM. Suspensionplasty for basal joint arthritis: why and how. Hand Clin 2006;22:171-175.
- Tomaino MM, Pellegrini VD Jr, Burton RI. Arthroplasty of the basal joint of the thumb. Long-term follow-up after ligament reconstruction with tendon interposition. J Bone Joint Surg Am 1995;77(3):346-355.
- Tomaino MM, Vogt M, Weiser R. Scaphotrapezoid arthritis: prevalence in thumbs undergoing trapezium excision arthroplasty and efficacy of proximal trapezoid excision. J Hand Surg Am 1999;24(6):1220-1224.
- Weilby A. Tendon interposition arthroplasty of the first carpometacarpal joint. J Hand Surg Br 1988;13(4):421-425.
