Introduction to Extensor Mechanism Contractures
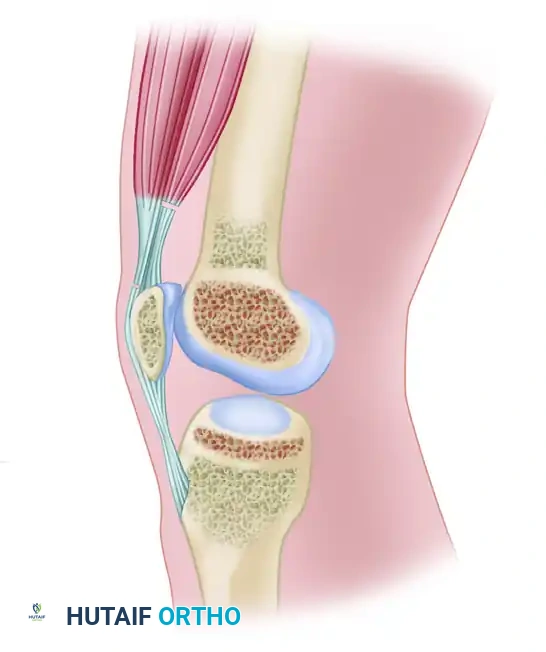
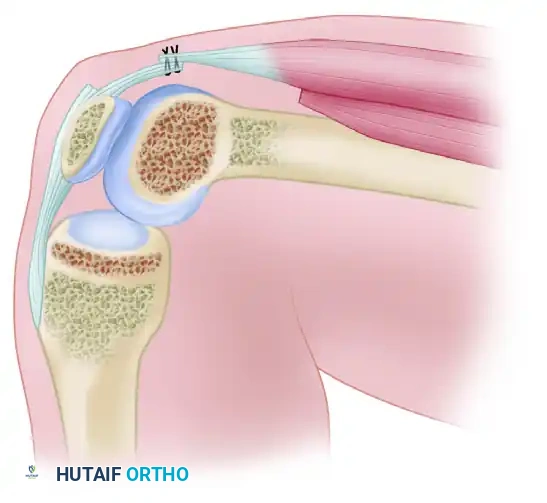
Severe extension contracture of the knee is a profoundly debilitating complication, most frequently arising secondary to distal femoral fractures, prolonged immobilization, or severe soft-tissue trauma. The pathoanatomy is characterized by the obliteration of the normal gliding planes within the extensor mechanism. Specifically, the vastus intermedius undergoes fibrotic degeneration, transforming into a rigid, scarred band that tethers the posterior surface of the rectus femoris and the superior pole of the patella directly to the anterior cortex of the femur.
When conservative measures—such as aggressive physical therapy, manipulation under anesthesia (MUA), and arthroscopic lysis of adhesions—fail to restore functional flexion, open or mini-open surgical intervention becomes necessary. The Thompson Quadricepsplasty remains the foundational open technique for addressing this pathology. However, to mitigate the extensive soft-tissue trauma associated with the classic approach, modern staged, sequential, and mini-incision modifications have been developed.
This comprehensive guide details both the classic Thompson Quadricepsplasty and the contemporary staged mini-incision technique, providing orthopedic surgeons with the critical biomechanical insights and step-by-step methodologies required to safely restore knee flexion.
Pathoanatomy and Biomechanics of Arthrofibrosis
To successfully execute a quadricepsplasty, the surgeon must understand the sequential tethering that restricts knee flexion:
1. Intrinsic Intraarticular Adhesions: Fibrosis within the suprapatellar pouch, medial and lateral gutters, and the anterior interval (the space posterior to the infrapatellar fat pad and anterior to the tibia).
2. Capsular and Retinacular Contracture: Thickening and shortening of the medial and lateral patellar retinacula, as well as the lateral expansions of the vasti.
3. Extrinsic Musculotendinous Tethering: The vastus intermedius adheres to the femoral periosteum, eliminating the excursion of the rectus femoris.
Surgical Pearl: The primary goal of quadricepsplasty is not merely to cut scar tissue, but to systematically isolate and release these three distinct anatomical blocks while preserving the continuity and active contractile tension of the extensor mechanism.
The Classic Thompson Quadricepsplasty
The classic Thompson technique is an aggressive, open procedure indicated for severe, recalcitrant extension contractures where the vastus intermedius is entirely replaced by dense fibrotic scar tissue.
Preoperative Preparation and Positioning
- Anesthesia: General or regional anesthesia with profound muscle relaxation is mandatory.
- Positioning: Supine on a radiolucent operating table. A sterile tourniquet is applied high on the proximal thigh.
- Equipment: An electrocoagulation unit must be used throughout the operation to maintain meticulous hemostasis, as postoperative hematoma is a primary catalyst for recurrent arthrofibrosis.
Step-by-Step Surgical Technique
1. Surgical Approach and Exposure
Make an anterior longitudinal incision through the skin and superficial fascia, extending from the proximal third of the thigh down to the distal pole of the patella. The exact trajectory of this incision should be modified to incorporate or bypass previous surgical scars to optimize skin flap viability.
2. Isolation of the Rectus Femoris
Divide the deep fascia along both the medial and lateral borders of the rectus femoris muscle. Extend this dissection from the proximal extent of the skin incision down to the patella. Carefully separate the rectus femoris from the adjacent vastus medialis and vastus lateralis.
3. Capsular and Retinacular Release
Divide the anterior portion of the knee capsule. This must include the lateral expansions of the vasti on both sides of the patella. The release must be carried far enough posteriorly and distally to completely overcome their contracture.
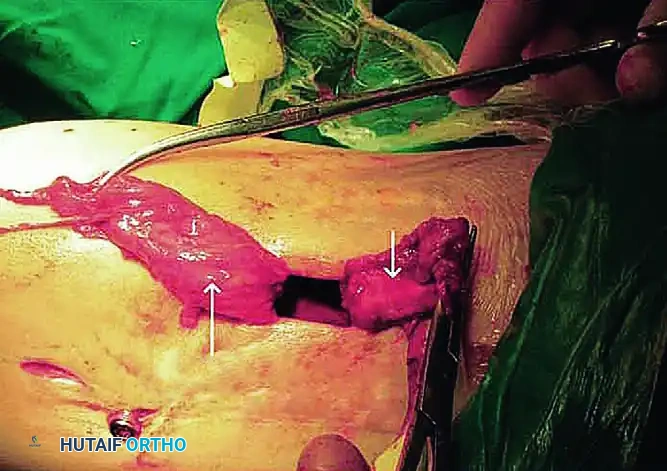
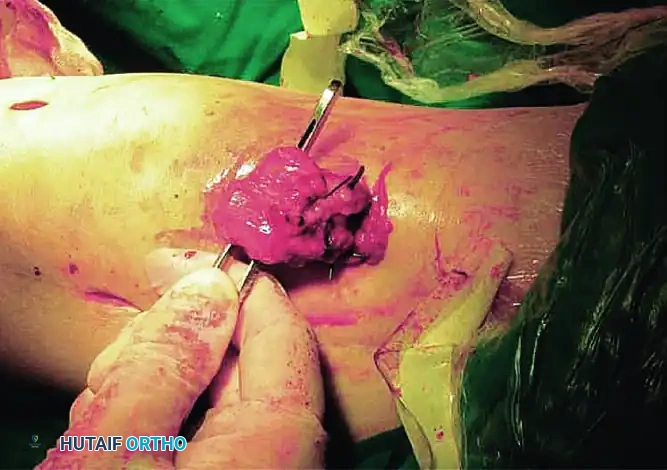
4. Excision of the Vastus Intermedius
This is the critical step of the Thompson procedure. The vastus intermedius will typically present as a dense, scarred band binding the rectus femoris and patella to the femur.
- Excise the vastus intermedius completely.
- Crucial Step: Leave a thin fibrous or periosteal covering on the anterior surface of the femur to prevent raw cortical bone from adhering to the rectus femoris postoperatively.
Surgical Warning: If the tendon of the rectus femoris has been destroyed by the initial injury or previous surgeries, the surgeon must create a neo-tendon by making longitudinal incisions through the dense scar tissue in the distal third of the thigh.
5. Intraoperative Flexion and Adhesion Release
With the vastus intermedius excised, slowly and gently flex the knee to 110 degrees. This maneuver will audibly and palpably release the remaining intraarticular adhesions. Do not force flexion beyond the tissue's elastic limit to avoid patellar tendon avulsion or supracondylar femur fracture.
6. Muscle Interposition and Closure
Evaluate the condition of the vastus medialis and lateralis:
- If they are severely scarred: Interpose subcutaneous tissue and fat between them and the rectus femoris to prevent cross-adhesion.
- If they are relatively normal: Suture them to the margins of the rectus femoris as far distally as the distal third of the thigh.
Deflate the tourniquet prior to closure. Obtain absolute, meticulous hemostasis. Place closed-suction drains and close the wound in layers.
Modern Mini-Incision Staged Quadricepsplasty (Wang, Zhao, He)
As an alternative designed to minimize iatrogenic damage to the quadriceps mechanism, a proximal-based, staged, sequential release of the intrinsic and extrinsic structures was developed. This mini-incision technique systematically addresses the pathology in five distinct stages, allowing the surgeon to stop the procedure as soon as adequate flexion is achieved.
STAGE 1: Lateral Retinacular Release
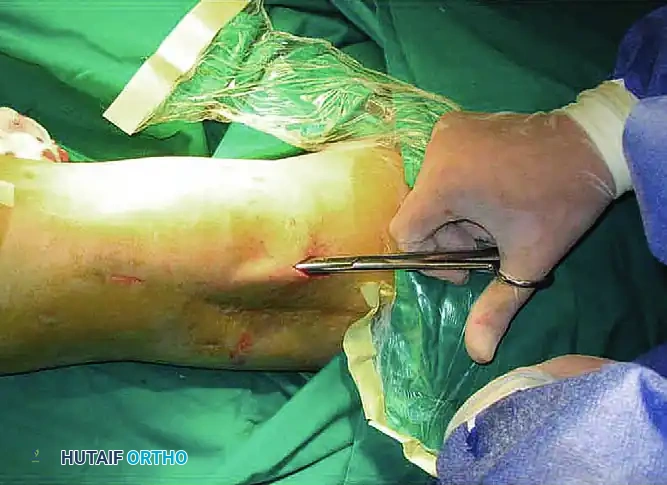
- Utilizing an inside-out technique, create a percutaneous parapatellar lateral arthrotomy.
- Incise the lateral retinaculum directly from the patella along its lateral border, extending from the superolateral corner of the patella down to the lateral aspect of its lower pole.
- To fully restore the lateral recess, free the lateral retinaculum from the lateral femoral condyle. Continue proximally to free the vastus lateralis tendon and the iliotibial band from their adhesions to the distal third of the femur.
STAGE 2: Mobilization of the Anterior Compartments
- Systematically mobilize the suprapatellar pouch, the patellofemoral compartment, and the anterior interval by sharply dividing the adhesions within these spaces.
- Anatomical Note: The anterior interval is defined as the region of the knee posterior to the infrapatellar fat pad and anterior to the anterosuperior aspect of the tibial plateau. Obliteration of this space is a major contributor to patella infera and restricted flexion.
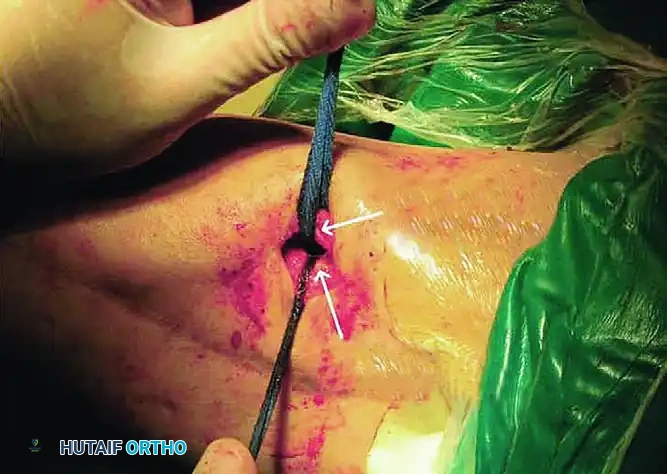
- Separate the tendinous tissue of the vastus intermedius from the posterior surface of the rectus femoris and the anterior surface of the femur.
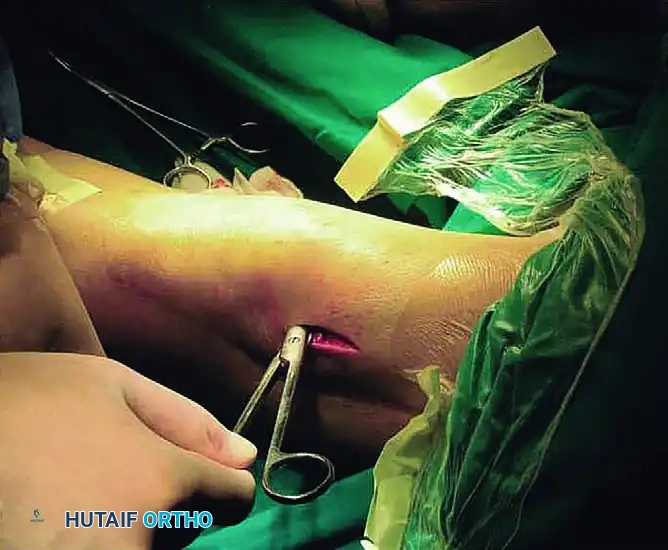
STAGE 3: Medial Retinacular Release

- Using a percutaneous inside-out technique, release the medial patellar retinaculum through the suprapatellar pouch, patellofemoral compartment, and anterior interval that were reestablished in Stage 2.
- Pitfall Avoidance: Take extreme care to delineate the medial arthrotomy margin. This margin starts from the medial epicondyle of the femur and slants laterally to the tibial tubercle. You must avoid detachment of the vastus medialis from its critical insertion at the superomedial corner of the patella.
- Free the medial retinaculum from the medial femoral condyle, and free the vastus medialis from the distal third of the femur to fully restore the medial recess.
STAGE 4: Transection of the Vastus Intermedius
- If flexion remains inadequate after the first three stages, proceed to Stage 4.
- Transect the previously mobilized vastus intermedius at a level near its musculotendinous junction. In knees with moderate arthrofibrosis, these first four stages often allow knee flexion of more than 120 degrees, at which point the procedure can be terminated.
STAGE 5: Quadriceps Tendon Lengthening
For severe arthrofibrosis, the fifth stage is mandatory to gain more than 90 degrees of flexion.
- Transect the rectus femoris at a more distal level than the vastus intermedius, adjacent to its patellar insertion.
- Deliver the free tendinous ends of the vastus intermedius and the rectus femoris through the surgical wound.
- Gently manipulate the knee in flexion repeatedly until maximal passive flexion is achieved.
- Overlap the proximal tendinous end of the vastus intermedius and the distal portion of the rectus femoris tendon.
- Suture the overlapped tendons using a No. 2 nonabsorbable braided suture (e.g., Ethibond) with the knee held strictly in 90 degrees of flexion.
Dynamic Tensioning Pearl: Test the passive range of motion after repairing the quadriceps tendon. The lengthened tendon must be under substantial tension but remain competent at 90 degrees of flexion.
- If the knee flexes easily beyond 90 degrees: Increase the overlapping of the tendons by advancing the vastus intermedius tendon more proximally. This reduces the risk of a severe postoperative extension lag.
- If flexion is restricted: Decrease the overlapping by fixing the vastus intermedius tendon more distally.
Throughout the procedure, continuously manipulate the knee in flexion to release any remaining intraarticular adhesions and assess the arc of motion. Once flexion of more than 120 degrees is achieved, terminate the extraarticular portion of the procedure. Place closed suction drains and close the skin.
Note: With the suprapatellar pouch, lateral recess, and medial recess restored, arthroscopic surgery can now be safely performed for the lysis of any residual fine intraarticular adhesions.
Postoperative Care and Rehabilitation Protocols
The success of a quadricepsplasty is entirely dependent on the postoperative rehabilitation protocol. The surgeon must balance the need to maintain the newly acquired flexion with the need to protect the extensor mechanism repair (if lengthened) and prevent severe extension lag.
Immediate Postoperative Phase
- A compressive wrap with an elastic bandage is applied from the toes to the proximal thigh to minimize edema and hemarthrosis.
- Physical therapy is initiated on postoperative day one.
Protocol for Lengthened Quadriceps Tendon (Stage 5 Utilized)
When the quadriceps tendon has been lengthened, the repair must be protected during the initial healing phase.
- Weeks 0-3: A continuous passive motion (CPM) machine is used as tolerated. The range and speed of motion are increased gradually, but must not exceed 90 degrees of flexion during the first 3 weeks. Active-assisted flexion (restricted to 90 degrees) and patellar mobility exercises begin on day one.
- Weeks 4-6: Additional flexion and quadriceps-strengthening exercises are introduced. This includes active straight-leg raises, isometric quadriceps exercises, progressive resistance exercises, and stationary bicycling.
- Nighttime Splinting: The knee is kept in full extension in a rigid splint or brace during the night to prevent flexion contractures and minimize extensor lag.
Protocol for Intact Quadriceps Tendon (Stages 1-4 Only)
If the quadriceps tendon was not lengthened (e.g., classic Thompson without rectus destruction, or Wang Stages 1-4 only), the rehabilitation program is significantly more aggressive.
- There is no restriction on the range of motion.
- Aggressive CPM, active, and active-assisted exercises for both the quadriceps and hamstrings are critical.
Long-Term Expectations and Complication Management
- Manipulation Under Anesthesia (MUA): If 90 degrees of flexion is not obtained by 6 weeks (for the mini-incision) or 3 months (for the classic Thompson), gentle manipulation under anesthesia may be required.
- Extensor Lag: Patients must be counseled preoperatively to expect a very slow return of active quadriceps extension. Severe quadriceps weakness will persist for many months. While most patients achieve significant improvements in their arc of flexion, an extension lag of 10 to 15 degrees is a common and often acceptable trade-off for functional flexion.
- Pediatric Considerations: If the patient is not skeletally mature, parents must be warned that some of the improvement in flexion may be lost as longitudinal bone growth occurs, potentially necessitating future interventions.
By meticulously executing these surgical steps and adhering to strict, phase-appropriate rehabilitation protocols, orthopedic surgeons can reliably restore functional mobility to patients suffering from severe arthrofibrosis and extensor mechanism contractures.
===FINAL_OUTPUT_ENDS_HERE===
📚 Medical References
- Thompson quadricepsplasty for the stiff knee, J Bone Joint Surg 82B:992, 2000.
- Herzenberg JE, Davis JR, Paley D, Bhave A: Mechanical distraction for treatment of severe knee fl exion contractures, Clin Orthop 301:80, 1994.
- Martin JN, Vialle R, Denormandie P, et al: Treatment of knee fl exion contracture due to central nervous system disorders in adults, J Bone Joint Surg 88A:840, 2006.
- Masse A, Biasibetti A, Demangos J, et al: The Judet quadricepsplasty: long-term outcome of 21 cases, J Trauma 61:358, 2006.
- Merchan EC, Myong C: Quadricepsplasty: the Judet technique and results of 21 posttraumatic cases, Orthopedics 15:1081, 1992.
- Nicoll EA: Quadricepsplasty, J Bone Joint Surg 45B:483, 1963.
- Steinfeld R, Torchia ME: Arthroscopically assisted percutaneous quadricepsplasty: a case report and description of a new technique, Arthroscopy 14:212, 1998.
- Thompson TC: Quadricepsplasty to improve knee function, J Bone Joint Surg 26:366, 1944.
- Tomak Y, Piskin A, Gulman B, et al: Treatment of U-shaped bone ankylosis of the knee with the Ilizarov method: a case report, J Bone Joint Surg 87A:1104, 2005.
- Ulusal AE, Ulusal BG, Lin YT, et al: The advantages of
