BACKGROUND
Arik Zaretski Ravit Yanko-Arzi Yehuda Kollender Eyal GurJacob BickelsWide resection of long bone tumors can create a large intercalary bone defect requiring reconstruction. Such defects were traditionally reconstructed with prosthetic implants, allografts, and allograft prostheticcomposites, all of which were associated with considerably high rates of complications and failures.5Distraction osteogenesis provides biologic reconstruction of only small- to medium-sized intercalary defects. Moreover, it is a prolonged procedure, which requires up to 2 months for an elongation of 1 cm, and complications are frequent, patient compliance is critical, and large soft tissue defects cannot be addressedsimultaneously.8,12 Reported experience regarding safety and efficacy in the oncologic setup is also limited.Since the introduction of vascularized autogenous graft for long bone reconstruction after tumor resection in the early 1970s, the use of a free fibular flap has become a viable option for reconstruction of large intercalary bone defects following tumor resection or for the purpose of resection arthrodesis.3,4,6,9,10,11,13,15 Its inherentadvantage is based on its ability to exploit the biology of normal fracture healing rather than the creepingsubstitution that is fundamental to the incorporation of a nonvascularized graft.The fibula is an optimal vascularized graft source because of its anatomic accessibility and because removing an intercalary segment while preserving the proximal fibula, distal tibial-fibular syndesmosis, and the lateral malleolus would have minimal impact on knee and ankle stability and would not compromise weight-bearing capacity and overall function of the lower extremity. It allows reconstruction of large bone defects because of its independent blood supply, which permits graft incorporation into the host bone even when presence or viability of the surrounding soft tissue are considerably compromised because of previous surgery or radiation therapy.Furthermore, a vascularized fibular graft has the capability to hypertrophy over time as a response to continuous pressure load. As a result, vascularized fibula have shown excellent long-term durability.2,9,16 The fibular head can also be used for joint reconstruction after intercalary resection of bone tumors.7In summary, a free fibular graft provides a durable true biologic reconstruction with accommodative andregenerative capabilities associated with minimal short- and long-term complications.16 It requires a combined effort of highly trained and committed teams as well as the patient's compliance throughout a very long, complex, and demanding rehabilitation period. APPLIED ANATOMY OF THE FIBULAR FLAP
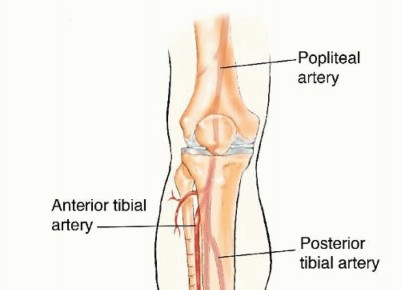
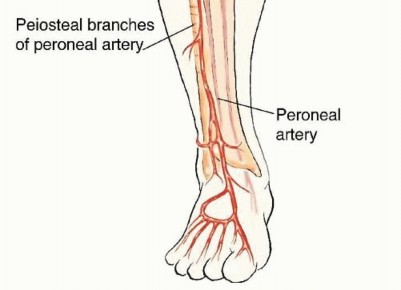
FIG 1 • The blood supply and drainage of the fibula are related to the peroneal artery and two peroneal veins, which follow a course parallel to the fibula. The fibula has a dual blood supply: endosteal and periosteal. The former is based on a nutrient artery that stems 6 to 14 cm from the peroneal bifurcation and the latter is based on multiple periosteal branches along the fibular diaphysis.
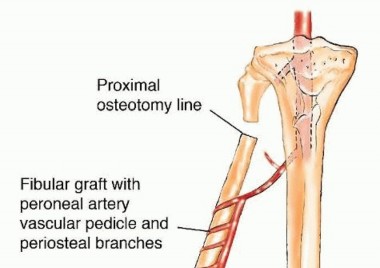
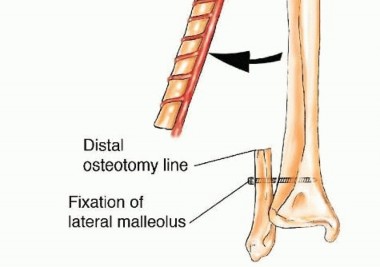
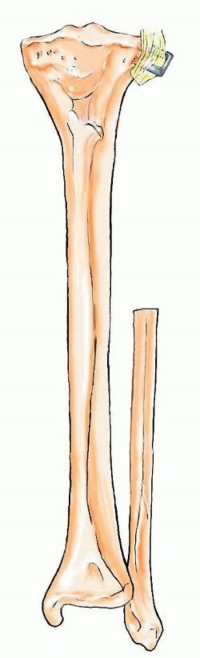
FIG 2 • Diaphyseal fibular graft, used for reconstruction of intercalary bone defects. If a long segment is required and the osteotomy is closed to the lateral malleolus, screw fixation to the tibia is advised to prevent valgus deformity and ankle instability. The proximal epiphysis may be included in the flap for joint reconstruction and preservation of longitudinal growth potential (in pediatric patients) after intra-articular resection of bone tumors (FIG 3). This flap is based on the anterior tibial vascular flap or the descending geniculate artery and is most commonly used for reconstructions following resections of the proximal humerus and distal radius.
INDICATIONS
Segmental bone defects larger than 5 cm following resection due to the following: TumorRadiation-induced bone necrosisOsteomyelitisIn cases of high-grade sarcomas of bone, the authors generally use spacers for immediate reconstruction following tumor resection rather than performing the definitive reconstruction with vascularized fibula. The latter is carried out 2 years after tumor resection if there had been no tumor recurrence or lung metastases.
CONTRAINDICATIONS
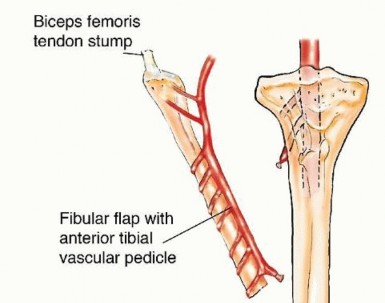
FIG 3 • Proximal fibular graft that includes the proximal fibular epiphysis and based on the anterior tibial vascular pedicle may be used for joint reconstruction and preservation of longitudinal growth in children following intra-articular resection of bone tumors. P.1284Donor site considerationsFibular deformity following previous injury to the lower extremity Vascular injury or compromise following previous trauma to the legVascular anomalies of the leg or plantar arches (eg, single-vessel or peroneal vessel-dominant foot) Recipient site considerationsInfection around the recipient site Suspected tumor recurrence
IMAGING AND OTHER STAGING STUDIES
Detailed preoperative evaluation of both the recipient and donor sites is mandatory. Imaging of the recipient site should provide information regarding the dimensions of bone (length and diameter) and soft tissue defects remaining after tumor resection, thus allowing the selection of the appropriate type and size of fibular flap to be used.Imaging of the donor site should include the entire leg and is aimed at excluding fibular deformity and at determining maximal flap length.The surgeon should verify adequate pulses in both posterior tibial and dorsalis pedis arteries. Evaluation of the deep and superficial plantar vascular arches is done using an equivalent to the palmar Allen test and is confirmed by Doppler ultrasound examination. If those studies are nonconclusive, an angiography or computed tomography angiography (CTA) is performed.
RECIPIENT SITE

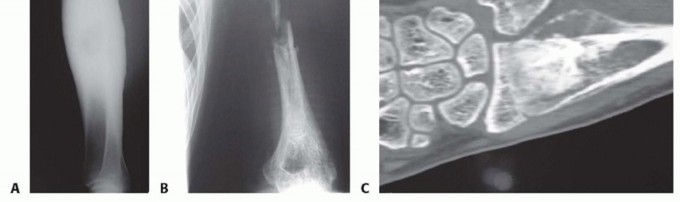
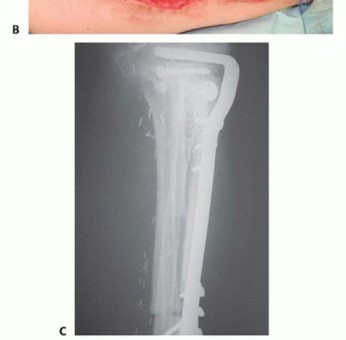
FIG 4 • A. Plain radiograph of the tibia showing a large diaphyseal low-grade osteosarcoma. B. Plain radiograph of the arm showing considerable bone loss and pathologic fracture associated with acute osteomyelitis of the humeral diaphysis. C. Coronal CT reconstruction of the distal forearm showing an osteosarcoma of the distal radius.
DONOR SITE
Plain radiography CTADoppler ultrasound (done intraoperatively to detect the skin island perforants)
SURGICAL MANAGEMENT
To minimize the duration of surgery and if the patient's position on the operating table permits, the fibular flap is harvested simultaneously with the preparation of the recipient site, a procedure that may include resection of the primary bone tumor or removal of a spacer that had been used in a previous surgery for reconstructive purposes.
INTERCALARY RESECTION
As a rule, a vascularized fibula in its straight and simple configuration is sufficient for reconstruction of bone defects of the upper extremity because of the relatively narrow cross-sectional diameter of the latter.Reconstruction of such defects of the lower extremity requires graft material of a larger diameter because of the additional mechanical support needed. A double-barrel fibular flap can be used for reconstruction of femoral and tibial defects of up to 13 cm. Longer defects may require the support of an allograft, which provides the initial stability required for bone healing, graft incorporation, and subsequent fibular hypertrophy.Furthermore, in cases of failed vascular anastomosis, the combined fibular-allograft construct is still comparable to multiple cortical allogenic struts with a relatively good chance of success, especially if reliable fixation is achieved. The technique of combined reconstruction with an allograft and the vascularized fibula, asdescribed by Capanna and his colleagues,1,2 provides such stability and is the preferred method of reconstruction used by the authors for long intercalary defects of the lower extremities.P.1285
TECHNIQUE
POSITION AND INCISION

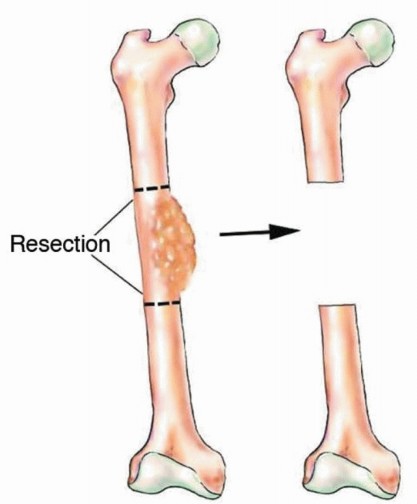
TECH FIG 2 • Diaphyseal tumor is resected with wide margins, leaving a long intercalary bone defect.



TECH FIG 4 • Following tissue sampling and cultures, administration of intravenous antibiotics, and
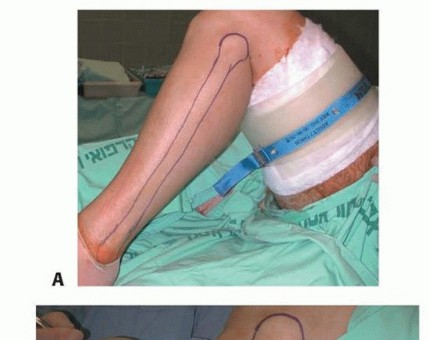


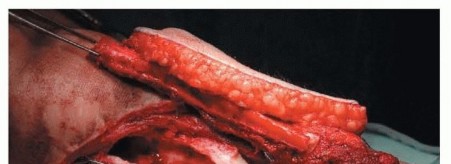
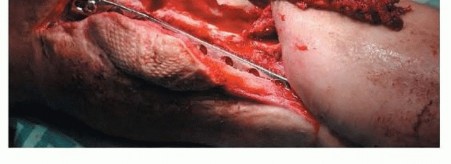
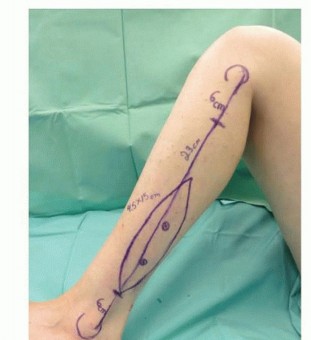
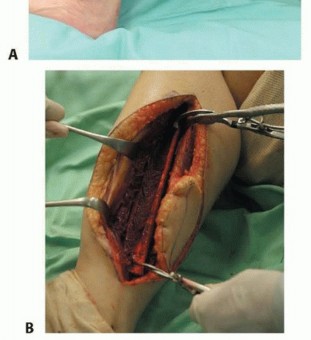
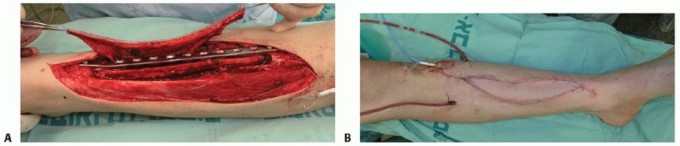
TECH FIG 5 • A. An anterolateral leg incision is used for harvesting of the fibular flap. B. An intercalary fibular segment, 6 cm longer from the bone defect, with its periosteal cuff is harvested.
TECH FIG 6 • A-F. If a large skin defect is anticipated at the tumor resection site, the fibular graft is removed with an overlying skin island, which is used for coverage of that defect and for monitoring of flap viability.(continued)
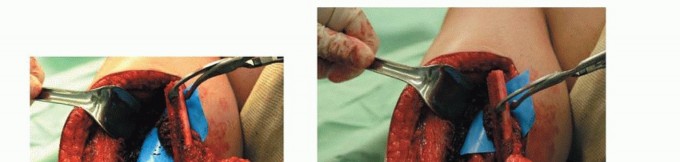

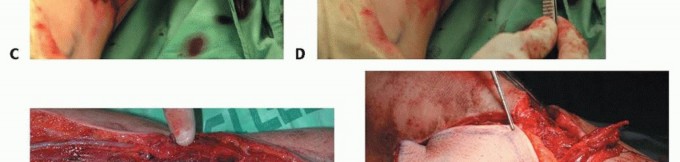
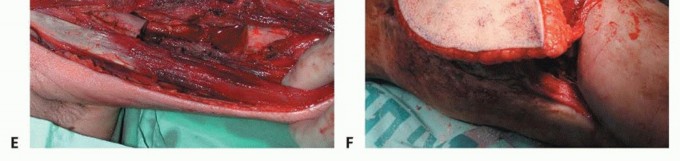
TECH FIG 6 •(CONTINUED)

TECH FIG 7 • Skin is harvested and the underlying fascia is left intact over the peroneal tendons.
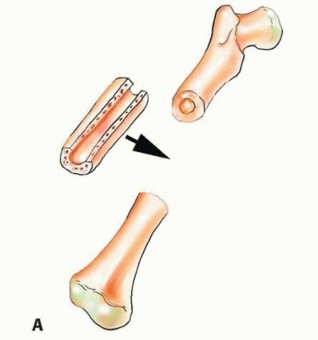
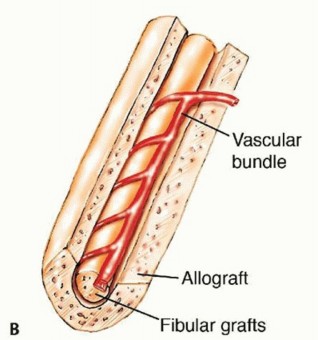
TECH FIG 8 • A. The allograft is cut to the same length as the bone defect, and a groove is opened longitudinally by removing as much cortical and cancellous bone as needed to allow insertion of the fibular graft into it. It is then inserted to fill the bone defect and fixed to its proximal and distal edges with a side plate and screws. B. A defect is created in the allograft cortex to allow the passage of the fibular vascular pedicle.
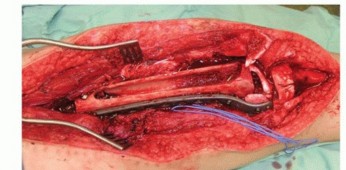
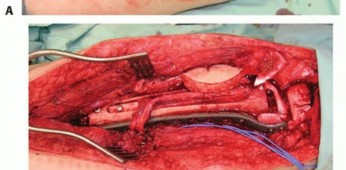
TECH FIG 9 • A. Intercalary defect of the distal femur is filled with canoe-shaped allograft. B. The free vascularized fibula is inserted into the allograft's medullary canal. A small skin island is included to allow monitoring of flap perfusion. C. Plain radiograph in a different patient showing the fibular graft inserted into the allograft's medullary canal and fixed with screws.
INTRA-ARTICULAR RESECTIONS
TECH FIG 10 • Following removal of a proximal fibular graft, the stump of the lateral collateral ligament is secured to the lateral tibial metaphysis to restore lateral knee joint stability.
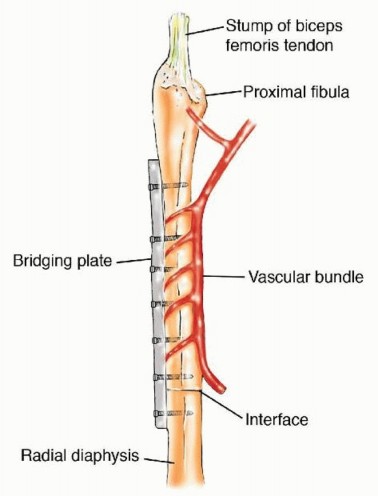
TECH FIG 11 • Reconstruction of proximal fibular graft to the remaining radial diaphysis.


PEARLS AND PITFALLS
FIG 5 • A. An implantable Cook-Swartz Doppler is used to monitor fibular flap perfusion. B. Following wound closure, flap perfusion is monitored by the implantable Doppler and viability of the overlying skin island.
POSTOPERATIVE CARE AND REHABILITATION
All patients must be treated and monitored postoperatively according to a strict and constant protocol. They are admitted to the department of plastic surgery for the first 5 days after surgery, where they are monitored for vital signs and flap viability and administered a mildly elevated volume of lactated Ringer solution (1.2 times the maintenance) to maintain blood flow through the anastomosis and prevent thrombus formation. This fluid protocol is maintained for a total of 5 days.Enoxaparin is given for prevention of deep vein thromboses. Blood samples are drawn twice daily for blood count and electrolytes. Hemoglobin levels are kept between 9 and 10 g/mL to minimize blood viscosity and further decrease the likelihood of anastomotic thrombus.Recipient extremities are immobilized for 3 months (an upper extremity by a brace and a lower extremity by a plaster cast) after which gradual passive ranges of motion are practiced.Signs of bony union are evaluated radiologically by serial plain radiographs. Bone unions are usually seen after 4 to 5 months in the upper extremity and after 5 to 7 months in the lower extremity. Partial weight bearing is allowed on detection of radiologic evidence of bone union. Gradual physical loads on the limb are recommended until full weight bearing is achieved.
OUTCOMES
Solid bony unions associated with fibular hypertrophy, full weight bearing, and mechanical load capacities are achieved in the vast majority of patients. Fibular hypertrophy occurs over years and is the result of pressure transport, microfractures, and callus formation.Mild to moderate decreases in range of motion are common and of a similar extent to those seen after other types of reconstructive surgeries. The latter is the result of the extent of resection of bone and soft tissues rather than the mode of reconstruction.Deep infections are rare, as is hardware failure requiring revision surgery.
COMPLICATIONS
Recipient siteAnastomotic thrombosis and loss of flap viability Partial skin island necrosisNonunion InfectionHardware failure and breakage Donor siteValgus ankle deformity Ankle joint instabilityTransient or permanent peroneal palsyTransient or permanent peroneal distribution area sensory deficit Skin graft failure and tendon exposureTransient or permanent great toe flexion impairment
REFERENCES
- Capanna R, Bufalini C, Campanacci M. A new technique for reconstructions of large metadiaphyseal bone defects. Orthop Traumatol 1993;3:159-177.
- Capanna R, Campanacci DA, Belot N, et al. A new reconstructive technique for intercalary defects of long bones: the association of massive allografts with vascularized fibular autograft. Long-term results and comparison with alternative techniques. Orthop Clin North Am 2007;38:51-60.
- Chang DW, Weber KL. Use of a vascularized fibula bone flap and intercalary allograft for diaphyseal reconstruction after resection of primary extremity bone sarcomas. Plast Reconstr Surg 2005;116: 1918-1925.
- Gebert C, Hillmann A, Schwappach A, et al. Free vascularized fibular grafting for reconstruction after tumor resection in the upper extremity. J Surg Oncol 2006;94:114-127.
- Getty PJ, Peabody TD. Complications and functional outcomes of reconstruction with an osteoarticular allograft after intra-articular resection of the proximal part of the humerus. J Bone Joint Surg 1999;81(8):1138-1146.
- Innocenti M, Delcroix L, Manfrini M, et al. Vascularized proximal fibular epiphyseal transfer for distal radial reconstruction. J Bone Joint Surg Am 2004;86:1504-1511.
- Innocenti M, Delcroix L, Manfrini M, et al. Vascularized proximal fibular epiphyseal transfer for distal radial reconstruction. J Bone Joint Surg Am 2005;87:237-246.P.1291
- Kocaoglu M, Eralp L, Rashid H, et al. Reconstruction of segmental bone defects due to chronic osteomyelitis with use of an external fixator and an intramedullary nail. J Bone Joint Surg Am 2006;88: 2137-2145.
- Malizos KN, Zalavras CG, Soucacos PN, et al. Free vascularized fibular grafts for reconstruction of skeletal defects. J Am Acad Orthop Surg 2004;12:360-369.
- McKee DM. Microvascular bone transplantation. Clin Plast Surg 1978;5:283-292.
- O'Brien BM, Morrison WA, Ishida H, et al. Free flap transfers with microvascular anastomoses. Br J Plast Surg 1974;27:220-230.
- Paley D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. Clin Orthop Relat Res 1990;250:81-104.
- Rose PS, Shin AY, Bishop AT, et al. Vascularized free fibula transfer for oncologic reconstruction of the humerus. Clin Orthop Relat Res 2005;438:80-84.
- Schmulder A, Gur E, Zaretski A. Eight-year experience of the Cook-Swartz Doppler in free-flap operations in microsurgical and reexploration results with regard to a wide spectrum of surgeries. Microsurgery 2011;31(1):1-6.
- Taylor GI, Miller GD, Ham FJ. The free vascularized bone graft. A clinical extension of microvascular techniques. Plast Reconstr Surg 1975;55:533-544.
- Zaretski A, Amir A, Meller I, et al. Free fibula long bone reconstruction in orthopedic oncology: a surgical algorithm for reconstructive options. Plast Reconstr Surg 2004;113:1989-2000.
