Introduction & Epidemiology
Spinal trauma represents a significant public health burden, characterized by high morbidity, potential for permanent disability, and substantial socioeconomic costs. The primary concern in managing any spinal injury is not solely the structural integrity of the bony or ligamentous elements, but critically, the intimate relationship these structures share with the delicate neurological elements: the spinal cord, its issuing nerve roots, and the cauda equina. The overarching goal is the preservation and optimization of neurological function, coupled with the restoration of spinal stability.
The incidence of spinal cord injury (SCI) in the United States is approximately 54 cases per million population, with an estimated 18,000 new SCIs annually. The mechanisms of injury are diverse, predominantly motor vehicle collisions (47.6%), followed by falls (22.3%), acts of violence (14.2%), and sports-related injuries (7.6%). Males account for the majority of these injuries (78%), with an average age at injury around 43 years. While complete paraplegia has remained relatively stable, advancements in pre-hospital care, surgical techniques, and rehabilitation have led to a slight increase in the proportion of incomplete neurological deficits, highlighting the imperative for timely and precise intervention.
The initial assessment dictates the entire management pathway. If a patient presents without neurological complication, a rigorous evaluation of the inherent stability of the injured segment is paramount. Any potential for delayed neurological involvement must be meticulously assessed, and if such a risk exists, stringent precautions must be implemented at every stage of patient handling, investigation, and treatment to prevent its manifestation. In cases of incomplete paraplegia or other major neurological deficits, vigilance is elevated further, demanding utmost care to prevent any neurological deterioration. Conversely, for patients with complete paraplegia, early and accurate establishment of the prognosis regarding potential recovery is critical for patient counseling and planning. Only once the neurological deficit is definitively deemed total and permanent can the intensity of vigilance surrounding the physical handling of the spinal injury be marginally relaxed, though meticulous care remains essential for comprehensive long-term management.
In summary, the cornerstone of effective management of spinal injuries hinges upon a profound and thorough understanding of the specific nature of damage to the bony architecture, the critical supportive ligamentous structures, and the intimately related neurological elements. This integrated perspective guides therapeutic decisions, from conservative care to complex surgical reconstruction, always prioritizing the patient's neurological future and spinal stability.
Surgical Anatomy & Biomechanics
A profound understanding of spinal anatomy and biomechanics is non-negotiable for any surgeon managing spinal trauma. The spine is a complex osteoligamentous structure designed for both flexibility and stability, protecting the vital neurological elements housed within.
Vertebral Morphology
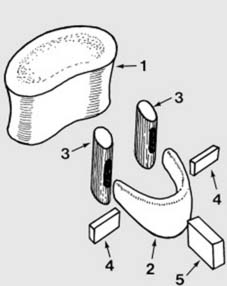
The components of a typical vertebra possess intricate interrelationships, forming a functional unit. An exploded diagram, such as the one presented, effectively illustrates these individual elements:
*
Vertebral Body:
The primary weight-bearing structure, an anterior cylindrical mass. Its superior and inferior surfaces are covered by hyaline cartilage, articulating with the intervertebral discs.
*
Vertebral Arch (Neural Arch):
Composed of two pedicles and two laminae.
*
Pedicles:
Short, stout processes extending posteriorly from the posterolateral aspects of the vertebral body. They contribute significantly to the structural integrity of the vertebral column and are critical for pedicle screw fixation.
*
Laminae:
Flat plates extending posteromedially from the pedicles, uniting in the midline to form the posterior aspect of the vertebral arch.
*
Processes:
*
Spinous Process:
Projects posteriorly and inferiorly from the junction of the laminae, serving as an attachment point for muscles and ligaments.
*
Transverse Processes:
Project posterolaterally from the junction of the pedicles and laminae, providing attachment for muscles and ligaments.
*
Articular Processes (Facets):
Superior and inferior articular processes project from the junction of the pedicles and laminae, forming synovial joints (facet joints) that guide and limit spinal motion. The orientation of these facets varies significantly by region, influencing regional kinematics.
Regional variations are crucial. Cervical vertebrae are characterized by smaller bodies, larger vertebral foramina, bifid spinous processes (C2-C6), and transverse foramina for the vertebral arteries. Thoracic vertebrae have heart-shaped bodies, long, slender, inferiorly sloping spinous processes, and costal facets for rib articulation. Lumbar vertebrae possess large, kidney-shaped bodies and stout, quadrangular spinous processes. The sacrum and coccyx, formed by fused vertebrae, provide a stable base for the spine and pelvis.
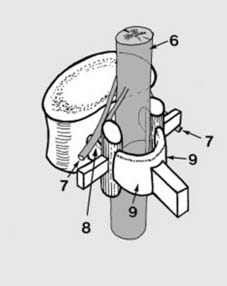
Illustration of different vertebral types, demonstrating regional variations in morphology.
Ligamentous Structures
The ligaments of the spine are critical for maintaining stability, limiting excessive motion, and resisting forces.
*
Anterior Longitudinal Ligament (ALL):
A broad, strong band covering the anterior aspect of the vertebral bodies and discs, resisting hyperextension.
*
Posterior Longitudinal Ligament (PLL):
Narrower and weaker than the ALL, located on the posterior aspect of the vertebral bodies within the vertebral canal, resisting hyperflexion and posterior disc herniation.
*
Ligamentum Flavum:
Composed predominantly of elastic tissue, connecting the laminae of adjacent vertebrae. Its elasticity helps maintain constant tension and prevents buckling into the spinal canal during extension.
*
Interspinous Ligaments:
Connect adjacent spinous processes.
*
Supraspinous Ligament:
A strong, cord-like ligament connecting the tips of the spinous processes from C7 to the sacrum (above C7, it becomes the nuchal ligament). Both interspinous and supraspinous ligaments resist hyperflexion.
*
Intertransverse Ligaments:
Connect adjacent transverse processes.
*
Capsular Ligaments:
Surround the facet joints, contributing to their stability.
Damage to these ligamentous structures, especially the posterior ligamentous complex (PLC – composed of the supraspinous, interspinous, and ligamentum flavum, and facet capsules), is a critical determinant of spinal stability.
Spinal Cord and Nerve Roots
The spinal cord extends from the foramen magnum to approximately the L1-L2 vertebral level, where it tapers into the conus medullaris. Below this, the lumbar, sacral, and coccygeal nerve roots continue as the cauda equina within the lumbar cistern. These neurological elements are exquisitely sensitive to compression, traction, and direct contusion. Understanding their precise anatomical relationship to the bony and ligamentous structures at each level is paramount for both diagnosis and surgical planning. Blood supply to the spinal cord, primarily from the anterior spinal artery and paired posterior spinal arteries, reinforced by radicular arteries, must also be considered, as compromise can lead to ischemia.
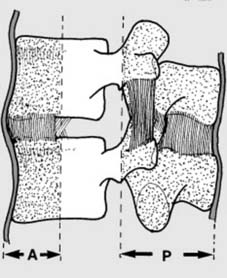
Illustration depicting the spinal cord and nerve roots within the vertebral canal.
Biomechanics and Stability
Spinal stability can be broadly defined as the ability of the spine to maintain its patterns of displacement under physiological loads without causing pain, neurological deficit, or gross deformity. The
three-column concept by Denis
is foundational in assessing spinal stability:
1.
Anterior Column:
Anterior longitudinal ligament, anterior half of the vertebral body, and anterior annulus fibrosus.
2.
Middle Column:
Posterior half of the vertebral body, posterior annulus fibrosus, and posterior longitudinal ligament.
3.
Posterior Column:
Posterior bony arch (pedicles, laminae, spinous process), posterior ligamentous complex (ligamentum flavum, interspinous, supraspinous ligaments, facet capsules), and facet joints.
An injury involving only one column is generally considered stable. Disruption of two columns typically indicates instability. Involvement of the middle column is particularly critical, as it signifies a higher likelihood of spinal canal compromise and instability.
Depiction of the three-column concept of spinal stability.
Other classification systems, such as the AO Spine classification , provide more granular details for specific fracture types (e.g., compression, burst, flexion-distraction, translational) and incorporate morphological features, neurological status, and specific posterior ligamentous complex integrity for determining stability and guiding treatment.
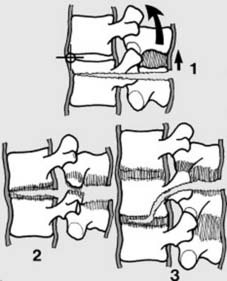
Kinematic chains and load-bearing capacity are also crucial. The spine acts as a flexible rod, transmitting forces from the head to the pelvis. Abnormal forces (compression, distraction, flexion, extension, rotation, shear) can lead to injury when physiological limits are exceeded.
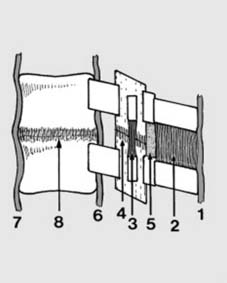
Diagram illustrating various forces acting on the vertebral segment.
Indications & Contraindications
The decision-making process for spinal trauma management is multifaceted, balancing the imperative for neurological preservation, spinal stability, and patient-specific factors. It generally involves a thorough assessment of fracture morphology, neurological status, ligamentous integrity, and patient comorbidities.
Indications for Operative Management
The primary indications for surgical intervention in spinal trauma are aimed at:
1.
Decompression of Neural Elements:
To relieve direct compression on the spinal cord or nerve roots, which may be caused by bony fragments, hematoma, or disc material. This is particularly urgent in cases of progressive or incomplete neurological deficit.
2.
Restoration of Spinal Alignment and Stability:
To prevent delayed neurological deterioration, reduce pain, facilitate early mobilization, and prevent progressive deformity.
3.
Correction of Deformity:
To address kyphotic or scoliotic deformities that result from trauma and may lead to functional impairment or pain.
Specific injury patterns and clinical presentations commonly warrant surgical intervention:
*
Unstable Fractures:
Any fracture type disrupting two or more columns (per Denis classification) or classified as unstable by other systems (e.g., AO Spine Type B or C injuries). This includes many burst fractures, fracture-dislocations, and flexion-distraction injuries (Chance fractures).
*
Neurological Deficit:
*
Progressive Neurological Deficit:
Any worsening of neurological function.
*
Incomplete Neurological Deficit:
Evidence suggests that early decompression (within 72 hours, ideally 24 hours) in incomplete SCI can improve neurological recovery.
*
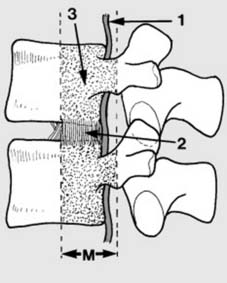
Spinal Canal Compromise:
Significant narrowing of the spinal canal (e.g., >30-50% in burst fractures) even in the absence of neurological deficit, particularly in the thoracic spine where the canal-to-cord ratio is small.
*
Ligamentous Instability:
Severe disruption of the posterior ligamentous complex (PLC) often necessitates stabilization, especially if associated with neurological compromise or bony injury. MRI is critical for assessing PLC integrity.
*
Failure of Non-Operative Management:
Progressive deformity, persistent pain, or neurological deterioration despite adequate conservative treatment.
*
Open Fractures:
Require surgical debridement and stabilization to prevent infection.
*
Penetrating Trauma:
May require exploration for neural decompression, dural repair, or foreign body removal.
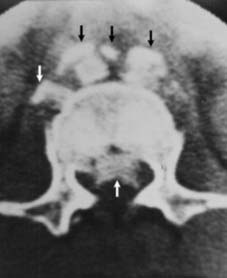
Illustration of significant spinal canal compromise due to a burst fracture.
Indications for Non-Operative Management
Conservative management is typically reserved for stable injuries without neurological compromise, where the intrinsic stability of the spine is preserved or can be adequately maintained with external support.
*
Stable Compression Fractures (e.g., AO Spine Type A0, A1, A2):
Without significant canal compromise, kyphotic deformity, or posterior ligamentous injury. These often involve wedge fractures with minimal anterior height loss.
*
Stable Burst Fractures (e.g., some A3/A4):
Without significant canal compromise, neurological deficit, or severe kyphosis, particularly in the lumbar spine.
*
Minor Ligamentous Injuries:
Sprains without frank instability.
*
Sacral Fractures:
Many isolated, non-displaced sacral fractures, if stable and without neurological compromise, can be managed conservatively.
*
Certain Cervical Fractures:
Stable odontoid fractures (Type I, some Type II), stable C1 fractures, or stable C2 Hangman's fractures can often be treated with external immobilization.
Contraindications to Operative Management
Absolute contraindications are rare but include:
*
Unstable Medical Comorbidities:
Patients who are medically unstable and unable to tolerate surgery (e.g., severe cardiac decompensation, uncontrolled sepsis). Resuscitation and stabilization are paramount.
*
Irreversible Coagulopathy:
Untreatable bleeding disorders.
Relative contraindications include:
*
Severe Local Infection:
Active infection at the surgical site.
*
Poor Soft Tissue Envelope:
Compromised skin integrity precluding safe surgical incision and wound closure.
*
Moribund Patient:
Where the risks of surgery clearly outweigh any potential benefits for survival or quality of life.
*
Complete Spinal Cord Injury:
While there is ongoing debate, in some centers, early surgery for complete SCI may be considered less urgent than for incomplete injuries, focusing more on stabilization and deformity prevention than neurological recovery. However, the current trend is towards early stabilization for most unstable injuries regardless of completeness, for ease of patient care, pain control, and rehabilitation.
Summary: Operative vs. Non-Operative Indications
| Indication | Operative Strategy | Non-Operative Strategy |
|---|---|---|
| Neurological Deficit |
-
Progressive Deficit:
Urgent decompression + stabilization.
- Incomplete Deficit: Early decompression + stabilization (ideally <24-72h). - Radiculopathy (due to compression): Decompression (for persistent/severe symptoms). |
- Stable Isolated Radiculopathy (no cord signs): Initial trial of conservative management (rest, NSAIDs, physical therapy) for select cases. |
| Spinal Instability (Mechanical) |
-
Unstable Burst Fractures:
Decompression (if indicated) + posterior or combined anterior/posterior instrumentation & fusion.
- Fracture-Dislocations: Reduction + rigid instrumentation & fusion. - Flexion-Distraction Injuries (e.g., Chance): Posterior instrumentation & fusion. - Severe Kyphosis/Deformity: Corrective osteotomies + instrumentation & fusion. |
-
Stable Compression Fractures (AO A0, A1, A2):
External bracing (TLSO, cervical collar), pain management, physical therapy.
- Stable Burst Fractures (no neurological deficit, minimal canal compromise): External bracing (TLSO), close radiographic follow-up. |
| Spinal Canal Compromise | - Significant Canal Narrowing (>30-50%): Decompression (laminectomy, corpectomy) + stabilization, even in neurologically intact patients, especially in thoracic spine. | - Minor Canal Compromise (<25-30%), Neurologically Intact: Close observation, conservative management. |
| Posterior Ligamentous Complex (PLC) Injury | - Complete PLC Disruption: Instrumentation & fusion (often posterior approach). | - Minor Sprains/Partial Tears (intact stability): External bracing, activity modification. |
| Open Spinal Fractures | - Surgical debridement, copious irrigation, stabilization, possible delayed closure. | - Not applicable. |
| Failed Non-Operative Management | - Progressive deformity, intractable pain, or neurological deterioration despite optimal conservative therapy. | - Continued conservative approach if patient refuses surgery or has absolute contraindications. |
| Severe Comorbidities | - Relative contraindication; careful risk-benefit analysis. May perform limited stabilization or external fixation if life-threatening. | - Definitive conservative management, supportive care, medical optimization. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and careful patient positioning are paramount to optimize surgical outcomes and minimize complications in spinal trauma.
Pre-operative Assessment
- Clinical Evaluation: A comprehensive history details the mechanism of injury, associated injuries, and pre-existing medical conditions. A thorough neurological examination, documented using the ASIA Impairment Scale (AIS), is critical to establish a baseline and identify evolving deficits.
-
Imaging Studies:
- Plain Radiographs: Anteroposterior and lateral views are initial screens for alignment and gross bony abnormalities. Oblique views or flexion/extension views may be used for specific stability assessments in the cervical spine after careful clinical clearance.
- Computed Tomography (CT) Scan: The gold standard for assessing bony anatomy, fracture morphology, and spinal canal compromise. 3D reconstructions are invaluable for understanding complex fracture patterns and planning screw trajectories.
- Magnetic Resonance Imaging (MRI): Essential for evaluating soft tissue injuries, including disc herniations, ligamentous disruptions (especially the PLC), spinal cord contusion, edema, hematoma, and nerve root impingement. It is critical in cases of neurological deficit or suspected ligamentous instability not evident on CT.
- Dynamic Flexion/Extension Views: Rarely performed in acute trauma due to risk of neurological compromise. Reserved for chronic stability assessment in equivocal cases.
- Medical Optimization: Patients with spinal trauma often have polytrauma. Medical optimization includes resuscitation, management of hemorrhage, pulmonary function assessment, cardiac clearance, and deep vein thrombosis (DVT) prophylaxis. Coagulation status, nutritional status, and glycemic control must be optimized.
- Surgical Goals: Clearly define the primary goals: neural decompression, reduction of deformity, restoration of stability, and choice of fusion strategy. This informs the approach, extent of instrumentation, and bone grafting techniques.
- Implant Selection: Based on biomechanical requirements, fracture pattern, patient anatomy, and surgeon preference. Pedicle screws are the workhorse for thoracolumbar fixation. Plates and cages are used for anterior column support. The number of levels to instrument (short vs. long segment) is a critical decision.
Patient Positioning
Patient positioning must achieve adequate surgical exposure, maintain spinal alignment, facilitate reduction maneuvers, and protect neural elements and pressure points.
*
General Principles:
*
Maintain Spinal Immobilization:
Until definitive fixation, the spine must be continuously protected. Log-rolling techniques are essential during transfer to the operating table.
*
Prevent Pressure Injuries:
Meticulous padding of all bony prominences, especially in patients with neurological deficits, is crucial to prevent decubitus ulcers and nerve palsies.
*
Optimize Hemodynamics:
Positioning should avoid compression of the abdomen, which can increase intra-abdominal pressure, impede venous return, and engorge the epidural venous plexus, leading to increased intraoperative blood loss.
*
Anesthetic Access:
Ensure adequate access for anesthesia monitoring and airway management.
-
Prone Position (Most Common for Posterior Approaches):
-
Supports:
Various supports are used:
- Relton frame/Jackson table/Andrews frame: Allows the abdomen to hang freely, reducing intra-abdominal and epidural venous pressure.
- Chest rolls/Bolsters: Placed longitudinally from clavicle to iliac crest, laterally to the abdomen, to achieve the same effect.
- Head Positioning: Carefully positioned on a soft pillow or headrest to prevent brachial plexus or facial nerve compression. In cervical spine injuries, the head may be placed in a Mayfield skull clamp to facilitate reduction and maintain alignment.
- Extremities: Arms are supported on arm boards, often abducted and flexed to 90 degrees at the elbow, ensuring radial and ulnar nerves are protected. Legs are padded to prevent peroneal nerve compression.
- Eyes/Face: Protected from pressure.
-
Supports:
Various supports are used:
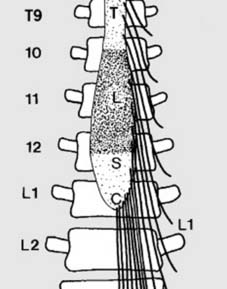
Illustration of prone patient positioning with appropriate padding and frame support.
-
Supine Position (For Anterior Cervical or Thoracic Approaches):
- Cervical: Head placed on a donut pillow or foam headrest. Shoulder roll may be used to achieve slight cervical extension and open the anterior neck.
- Thoracic: May require a transverse roll or sandbag under the scapulae to facilitate exposure.
-
Lateral Decubitus Position (For Anterolateral Thoracic or Lumbar Approaches):
- Patient positioned with the desired side up.
- Axillary roll placed to protect the dependent brachial plexus.
- Pillow between knees, lower leg flexed, upper leg extended for stability.
- Beanbag or similar device may be used for stability and to adjust spinal flexion/extension.
Intraoperative fluoroscopy or navigation is typically used to confirm correct spinal level and guide instrumentation. Neuromonitoring (SSEP, MEP) is standard practice, especially in cases of neurological deficit or complex deformity correction, to detect impending neural compromise.
Detailed Surgical Approach / Technique
Surgical intervention in spinal trauma aims to achieve neural decompression, anatomical reduction, and rigid stabilization. The choice of approach (posterior, anterior, or combined) depends on the injury morphology, location, neurological status, and the need for direct or indirect decompression and reconstruction.
General Principles
- Meticulous Hemostasis: Essential due to the vascularity of the spine and proximity to neurological structures.
- Preservation of Soft Tissues: Minimize muscle stripping to reduce pain, facilitate healing, and preserve blood supply to bony elements and muscle. Subperiosteal dissection is preferred.
- Neural Protection: Constant vigilance to avoid iatrogenic injury during dissection, decompression, and instrumentation. Intraoperative neuromonitoring (SSEP, MEP) is highly recommended.
- Appropriate Exposure: Adequate working space is critical for visualization and instrument manipulation.
Posterior Approach (Most Common for Thoracolumbar Trauma)
This approach is versatile for decompression (indirect or direct), reduction, and posterior instrumentation and fusion.
-
Incision and Dissection:
- Midline Incision: Centered over the fractured level, extended cranially and caudally to encompass the planned fusion levels.
- Subperiosteal Dissection: The thoracolumbar fascia is incised along the midline. Using electrocautery and Cobb elevators, the paraspinal muscles (erector spinae group: iliocostalis, longissimus, spinalis) are carefully stripped subperiosteally off the spinous processes, laminae, and transverse processes. This dissection is carried laterally to expose the facet joints and the base of the transverse processes, providing access for pedicle screw insertion. Minimally invasive techniques utilize muscle-splitting or tubular retractors to reduce muscle damage.
-
Pedicle Screw Placement: The cornerstone of posterior spinal fixation.
- Entry Point Selection: Critical and level-dependent. For thoracic pedicles, generally at the junction of the superior articular process, transverse process, and lamina. For lumbar pedicles, typically at the junction of the mamillary process, pars interarticularis, and transverse process.
- Pedicle Preparation: A high-speed burr or awl creates a starting hole. A pedicle probe (gear shift probe) is advanced into the pedicle, carefully palpating all five pedicle walls (superior, inferior, medial, lateral, anterior) to ensure an intraosseous trajectory.
- Screw Trajectory and Depth: Fluoroscopic guidance (AP and lateral views) or 3D navigation is invaluable. Screws are aimed toward the vertebral body, typically converging medially. Length is chosen to maximize purchase while avoiding anterior cortical penetration.
- Tapping and Screw Insertion: Pedicles are tapped (optional depending on screw design). Screws are inserted, ensuring firm bicortical purchase for optimal pullout strength.
-
Decompression (If Indicated):
- Laminectomy/Laminotomy: Removal of the lamina to directly decompress the spinal cord or nerve roots. Often performed above or below the level of greatest canal compromise.
- Facetectomy: Partial or total removal of facet joints, typically to gain access for discectomy or foraminotomy, or to facilitate reduction.
- Indirect Decompression (Ligamentotaxis): In burst fractures, reduction and distraction through posterior instrumentation can pull retropulsed fragments anteriorly, decompressing the canal.
-
Reduction of Deformity:
- Distraction: Applied through the screws to restore vertebral height and reduce kyphosis.
- Compression: Used across stable segments to enhance lordosis or compress fracture fragments.
- Cantilever Technique: Screws are placed, rods are contoured to the desired sagittal profile, and then carefully seated into the screw heads, using the contoured rod to reduce the deformity.
- Derotation: Used for coronal plane deformities.
-
Rod Contouring and Insertion:
- Rods are contoured to match the desired physiological sagittal and coronal spinal curves.
- Rods are then inserted into the heads of the pedicle screws and secured with set screws.
- Cross-Links: May be added between rods to enhance construct rigidity, especially in long constructs or highly unstable injuries.
-
Fusion:
- Decortication: The posterior elements (transverse processes, laminae, facet joints) are decorticated to expose cancellous bone, promoting osteointegration.
- Bone Grafting: Autograft (e.g., local bone from decortication, iliac crest), allograft, or synthetic bone graft substitutes are placed over the decorticated surfaces to achieve solid arthrodesis.
-
Wound Closure: Meticulous layered closure, ensuring no dead space and appropriate soft tissue coverage over the implants.
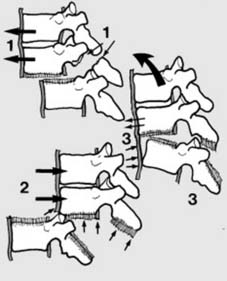
Illustration of posterior instrumentation with pedicle screws and rods.
Anterior Approach (Cervical, Thoracic, Lumbar)
Anterior approaches provide direct access to the vertebral body and intervertebral disc, enabling direct decompression, corpectomy, and reconstruction of the anterior column.
-
Anterior Cervical Discectomy and Fusion (ACDF)/Corpectomy (ACCF):
- Indications: Cervical disc herniation with cord compression, traumatic cervical burst fractures with anterior column instability and canal compromise.
- Approach: Smith-Robinson approach, typically on the right side. Transverse or longitudinal skin incision. Dissection between the carotid sheath (lateral) and the trachea/esophagus (medial), exposing the anterior aspect of the cervical spine.
- Decompression: Discectomy and/or corpectomy to remove compressing elements (disc, bone fragments).
- Reconstruction: Placement of a structural cage or allograft/autograft bone block into the defect to restore vertebral height.
- Fixation: Anterior cervical plate and screws to stabilize the construct and promote fusion.
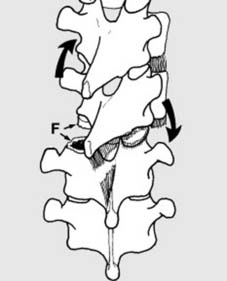
Illustration of anterior cervical plating.
-
Anterolateral Thoracic/Thoracolumbar Approaches:
- Indications: Significant anterior column pathology (e.g., severe burst fractures with retropulsed fragments, kyphotic deformity) not adequately addressed posteriorly, or when direct anterior decompression and reconstruction are preferred.
- Approach: Requires a thoracotomy (for thoracic spine), thoracoabdominal approach (for thoracolumbar junction), or retroperitoneal approach (for lumbar spine). These are often more invasive but allow for direct visualization and removal of anterior pathology.
- Decompression: Corpectomy (vertebral body resection) to decompress the spinal cord directly.
- Reconstruction: Placement of a structural cage (titanium, PEEK) or bone graft to restore anterior column height and load-bearing capacity.
- Fixation: Anterior vertebral body plate and screws.
Depiction of anterior vertebral body reconstruction with a cage and plate.
Combined Anterior and Posterior Approaches
- Indications: Highly unstable injuries, severe kyphotic deformity, or when both anterior and posterior column support are necessary (e.g., in cases of extensive vertebral body destruction and posterior ligamentous complex injury). Staged procedures are often employed.
The choice of technique is highly individualized, requiring an experienced surgeon to weigh the benefits and risks of each approach in the context of the specific patient and injury.
Complications & Management
Spinal surgery, particularly for trauma, carries inherent risks. A comprehensive understanding of potential complications, their incidence, and salvage strategies is crucial for patient safety and optimal outcomes.
Common Complications
-
Neurological Injury:
- Incidence: Highly variable, 0.5-5% for pedicle screw placement alone, higher in deformity correction or complex trauma.
- Description: Direct trauma to the spinal cord or nerve roots during decompression, screw misplacement, over-distraction, or malreduction. Can manifest as new or worsened motor/sensory deficit, radiculopathy, or cauda equina syndrome.
-
Management/Salvage:
- Intraoperative: Immediate detection via neuromonitoring prompts cessation of activity, screw repositioning, or decompression.
- Postoperative: Urgent imaging (CT for screw position, MRI for cord compression/hematoma). Prompt surgical revision for decompression or hardware adjustment. Steroids may be considered.
-
Dural Tear and Cerebrospinal Fluid (CSF) Leak:
- Incidence: 3-15%, higher in revision surgery or complex decompressions.
- Description: Accidental laceration of the dura mater, leading to CSF leakage. Can cause headache, pseudomeningocele, or increase infection risk.
-
Management/Salvage:
- Intraoperative: Primary repair with suture (e.g., 6-0 Prolene), reinforced with dural sealants (fibrin glue), muscle graft, or fat graft. Valsalva maneuver to confirm seal.
- Postoperative: Bed rest, head elevation, CSF diversion (lumbar drain) for persistent leaks. Surgical exploration and repair for large, symptomatic, or persistent leaks.
-
Infection:
- Incidence: Superficial: 2-5%; Deep: 0.5-2%, higher in open injuries or compromised patients.
- Description: Superficial wound infection, deep surgical site infection, discitis, osteomyelitis. Can lead to implant failure, pseudarthrosis, and sepsis.
-
Management/Salvage:
- Superficial: Oral antibiotics, local wound care.
- Deep: Surgical debridement, copious irrigation, deep cultures, intravenous antibiotics (6-12 weeks), may require hardware removal if infection persists despite treatment (usually after fusion is complete). Negative pressure wound therapy.
-
Instrumentation Failure:
- Incidence: 2-10%, depending on fracture type, bone quality, and construct length.
- Description: Screw pullout, rod fracture, loss of reduction, implant prominence. More common in osteoporotic bone or long fusions without adequate anterior support.
- Management/Salvage: Surgical revision with stronger fixation, longer construct, additional anterior column support, or cement augmentation in osteoporotic bone.
-
Pseudarthrosis (Non-Union):
- Incidence: 5-20%, higher in smokers, multi-level fusions, or extensive posterior element injury.
- Description: Failure of bony fusion, leading to persistent pain, implant failure, or progressive deformity.
- Management/Salvage: Revision surgery with re-debridement, fresh bone grafting (often autograft with biologics like BMP), and potentially more rigid or extended instrumentation. May consider electrical stimulation.
-
Vascular Injury:
- Incidence: Rare but potentially catastrophic (e.g., great vessel injury in anterior lumbar approaches, vertebral artery injury in cervical approaches).
- Description: Hemorrhage, pseudoaneurysm, AV fistula.
- Management/Salvage: Urgent surgical exploration and vascular repair (suture, graft, embolization). Pre-operative planning with CT angiography can identify aberrant vessels.
-
Pulmonary Complications:
- Incidence: Common, especially in patients with high thoracic injuries or prolonged recumbency.
- Description: Atelectasis, pneumonia, pulmonary embolism (PE).
- Management/Salvage: Prophylaxis (early mobilization, incentive spirometry, DVT prophylaxis). Aggressive pulmonary hygiene, chest physiotherapy. Anticoagulation and IVC filter for confirmed PE.
-
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE):
- Incidence: DVT 15-80% (depending on prophylaxis/screening), PE 5-20%, especially in SCI.
- Description: Venous clot formation in lower extremities or pelvis, risk of fatal PE.
- Management/Salvage: Chemical (LMWH) and mechanical (SCDs, TEDs) prophylaxis. Early ambulation. Anticoagulation for confirmed DVT/PE; IVC filter for contraindications to anticoagulation.
-
Adjacent Segment Disease (ASD):
- Incidence: Progressive, cumulative risk (2-4% per year).
- Description: Degeneration or instability at the spinal segment immediately adjacent to a fused level.
- Management/Salvage: Initial conservative management. Surgical intervention (decompression, fusion, or arthroplasty) if symptomatic and refractory to conservative care.
Table of Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approximate Range) | Management/Salvage Strategy |
|---|---|---|
| Neurological Injury | 0.5-5% |
Intraop:
Neuromonitoring (SSEP/MEP), immediate cessation of activity, screw repositioning, decompression.
Postop: Urgent imaging (CT/MRI), prompt surgical revision for decompression/hardware adjustment. Consider corticosteroids. |
| Dural Tear / CSF Leak | 3-15% |
Intraop:
Primary suture repair (6-0 Prolene), reinforcement with dural sealants (fibrin glue), muscle/fat graft. Valsalva test.
Postop: Bed rest, head elevation, lumbar drain for persistent leaks. Surgical exploration and repair for large/symptomatic leaks. |
| Surgical Site Infection | Superficial: 2-5%; Deep: 0.5-2% |
Superficial:
Oral antibiotics, local wound care.
Deep: Surgical debridement, copious irrigation, deep cultures, IV antibiotics (6-12 wks). May require hardware removal (after fusion). Negative pressure wound therapy. |
| Instrumentation Failure | 2-10% | Revision surgery: stronger fixation, longer construct, additional anterior column support, cement augmentation (in osteoporosis). |
| Pseudarthrosis (Non-Union) | 5-20% | Revision surgery: re-debridement, fresh bone grafting (autograft + biologics), more rigid/extended instrumentation. Electrical stimulation. |
| Vascular Injury | <1% (catastrophic) | Urgent surgical exploration, vascular repair (suture, graft, embolization). Pre-op imaging (CTA) for high-risk approaches. |
| Pulmonary Complications | Variable, up to 20-30% |
Prophylaxis:
Early mobilization, incentive spirometry, DVT prophylaxis.
Treatment: Aggressive pulmonary hygiene, chest physiotherapy, antibiotics (for pneumonia), bronchodilators. |
| DVT / Pulmonary Embolism | DVT: 15-80%; PE: 5-20% |
Prophylaxis:
Chemical (LMWH) and mechanical (SCDs, TEDs).
Treatment: Anticoagulation for DVT/PE. IVC filter for contraindications to anticoagulation or recurrent PE despite anticoagulation. |
| Adjacent Segment Disease (ASD) | 2-4% per year | Initial conservative management (NSAIDs, PT, injections). Surgical intervention (decompression, fusion, or arthroplasty) if symptomatic and refractory. |
| Ileus / Bowel Dysfunction | Common, especially with thoracolumbar injury | Nasogastric decompression, bowel rest, prokinetic agents. Gradual diet advancement. |
| Urinary Tract Infection (UTI) | Common, especially with SCI | Strict catheter care, early removal of foley catheter, appropriate antibiotics for positive cultures. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is an integral component of comprehensive spinal injury management, aiming to optimize functional recovery, prevent secondary complications, and facilitate a safe return to activity. Protocols vary based on the extent of injury, surgical stability, and neurological status.
Immediate Post-Operative Period (Days 0-7)
- Pain Management: Multimodal analgesia (opioids, NSAIDs, neuropathic agents) to control pain, facilitate mobilization, and minimize opioid dependence. Epidural analgesia or patient-controlled analgesia (PCA) may be used initially.
- DVT Prophylaxis: Continued pharmacological (LMWH, fondaparinux) and mechanical (sequential compression devices, compression stockings) prophylaxis is essential, particularly for patients with SCI or prolonged immobilization.
- Bowel and Bladder Management: Address post-operative ileus, constipation, and neurogenic bladder. Early mobilization, stool softeners, and a bowel regimen are initiated. Intermittent catheterization or indwelling catheter care for neurogenic bladder.
- Wound Care: Monitor for signs of infection, hematoma, or dehiscence. Dressing changes per protocol.
- Neurological Assessment: Serial neurological exams (ASIA scale) to detect any changes or recovery.
-
Early Mobilization:
- Log-rolling: Maintain spinal precautions during transfers.
- Out of Bed: Gradually progress from supine to sitting, then standing, typically within 24-48 hours, depending on surgical stability and patient tolerance.
- Ambulation: Short, supervised walks initiated as soon as safely possible, often with assistive devices.
Early Rehabilitation Phase (Weeks 1-6)
-
Bracing:
- Indications: May be used to provide external support, limit motion, and enhance comfort, particularly in less stable constructs or for patient reassurance.
- Types: Cervical collars (soft, semi-rigid, rigid), thoracolumbar sacral orthoses (TLSO), Jewett braces.
- Duration: Typically 6-12 weeks, depending on the fracture type, surgical construct, and radiographic evidence of healing.
-
Physical Therapy:
- Focus: Regain mobility, strength, and endurance.
-
Activities:
- Range of Motion (ROM): Gentle, protected active and passive ROM exercises for adjacent joints, avoiding excessive spinal motion at the surgical site.
- Strengthening: Gradual strengthening of core musculature (abdominal, paraspinal) and extremity muscles. Isometrics initially, progressing to dynamic exercises.
- Gait Training: Progression from assistive devices to independent ambulation. Balance and proprioception exercises.
- Functional Training: Activities of daily living (ADLs), transfers, body mechanics.
- Occupational Therapy: Addresses specific ADL challenges, adaptive equipment needs, and home modifications.
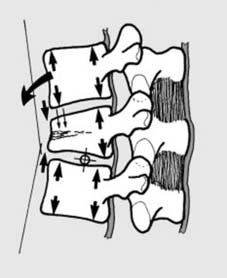
Illustration of post-operative bracing (TLSO) for spinal support.
Intermediate Rehabilitation Phase (Weeks 6-12)
-
Progression of Therapy:
- Increase intensity and duration of strengthening exercises.
- Incorporate more dynamic and functional movements.
- Balance training on unstable surfaces.
- Spine stabilization exercises to activate deep core muscles.
- Brace Weaning: If a brace was prescribed, it is gradually weaned based on clinical and radiographic healing, and patient comfort and confidence.
- Pain Management: Transition to non-opioid medications, focus on physical therapy modalities and patient education for self-management.
Long-Term Rehabilitation and Return to Activity (Months 3+)
- Radiographic Follow-up: Regular X-rays (and possibly CT scans) at 3, 6, and 12 months post-surgery to assess fusion progress, hardware integrity, and spinal alignment.
- Advanced Strengthening: Progress to advanced resistance training, focusing on compound movements and functional patterns specific to the patient's goals.
-
Return to Work/Sport:
- Sedentary Work: May be possible within 3-6 months.
- Light Manual Labor: 6-12 months, with proper body mechanics training.
- Heavy Manual Labor/Contact Sports: Typically not advised for at least 12 months, and often depends on complete fusion and specific injury patterns. Contact sports may be permanently restricted for certain spinal fusions.
- Patient Education: Emphasize lifelong ergonomic principles, proper lifting techniques, and maintaining a healthy weight and active lifestyle to prevent future spinal issues.
- Psychological Support: Address potential issues like depression, anxiety, and post-traumatic stress disorder, especially in patients with SCI.
Effective rehabilitation is a collaborative effort involving the surgeon, physiatrist, physical therapist, occupational therapist, and the patient. It requires patience, persistence, and adherence to prescribed protocols to maximize functional recovery and achieve long-term success.
Summary of Key Literature / Guidelines
The management of spinal trauma is dynamic, evolving with advancements in imaging, surgical techniques, and biomechanical understanding. Several classifications and guidelines underpin current evidence-based practice.
Classification Systems
- Denis Three-Column Classification (1983): As discussed, this system categorized the spine into anterior, middle, and posterior columns, defining stability based on column involvement. It was a seminal contribution, identifying middle column injury as critical for instability.
- AO Spine Thoracolumbar Spine Injury Classification System (2014): This comprehensive system is currently the most widely adopted for thoracolumbar fractures. It classifies injuries based on fracture morphology (Type A: compression, Type B: tension, Type C: translation), neurological status, and integrity of the posterior ligamentous complex (PLC). Each element is assigned a score, guiding treatment decisions towards operative or non-operative management.
- Subaxial Cervical Spine Injury Classification System (SLIC) (2007): Similar to the AO Spine system, SLIC helps determine management for subaxial cervical fractures based on morphology, integrity of the disco-ligamentous complex, and neurological status.
- Frankel Scale / ASIA Impairment Scale (AIS): These are critical for documenting neurological status and predicting prognosis for spinal cord injury. The ASIA scale, with its standardized motor and sensory examination, is the preferred method for communication and research.
Key Evidence-Based Guidelines and Literature
- Timing of Decompression for Incomplete Spinal Cord Injury: Landmark studies and meta-analyses (e.g., the STASCIS study) have strongly supported the benefit of early surgical decompression (within 24-72 hours) for patients with incomplete traumatic spinal cord injury. Early intervention is associated with improved neurological recovery compared to delayed decompression. This has become a cornerstone of modern spinal trauma management.
- Management of Burst Fractures: While stable burst fractures without neurological deficit can often be managed conservatively (e.g., with bracing), unstable burst fractures, especially those with significant canal compromise or neurological deficits, generally require surgical stabilization. Debates persist regarding anterior versus posterior approaches, but recent evidence often favors posterior approaches for robust stabilization, with anterior column reconstruction reserved for specific cases of severe anterior column deficiency or significant kyphosis.
- Posterior Ligamentous Complex (PLC) Integrity: MRI has revolutionized the assessment of PLC injury. Studies highlight the critical role of an intact PLC in maintaining spinal stability. A disrupted PLC, even in the absence of severe bony injury, often indicates instability and necessitates surgical stabilization.
- Cervical Spine Clearance: Guidelines for clearance of the cervical spine in awake, alert, and pain-free trauma patients without neurological deficits emphasize clinical assessment combined with advanced imaging (CT scan, especially for high-risk mechanisms or persistent midline tenderness). The National Emergency X-Radiography Utilization Study (NEXUS) criteria and the Canadian C-Spine Rule are widely used tools to determine the need for imaging. MRI may be indicated for ligamentous injury or occult neurological deficits.
- DVT/PE Prophylaxis in SCI: Strong evidence supports aggressive DVT prophylaxis (pharmacological and mechanical) in patients with spinal cord injury due to their extremely high risk of thromboembolic events. Current guidelines recommend initiation of prophylaxis as early as possible.
- Minimally Invasive Spine Surgery (MISS) in Trauma: While historically open approaches predominated, MISS techniques (e.g., percutaneous pedicle screw fixation) are increasingly being utilized for appropriate spinal trauma cases. Literature suggests potential benefits in reduced blood loss, shorter hospital stays, and decreased post-operative pain, though it may not be suitable for all complex injuries or those requiring direct decompression.
- Role of Biologics: The use of bone morphogenetic proteins (BMPs) and other biologics in spinal fusion for trauma is an area of ongoing research. While BMPs can enhance fusion rates, their use is not without controversy due to potential complications (e.g., heterotopic ossification, osteolysis) and cost.
Future Directions
Future advancements in spinal trauma will likely focus on:
*
Precision Medicine:
Tailoring treatment based on genetic predispositions, specific injury biomechanics, and individual patient responses.
*
Enhanced Neuromonitoring:
Development of more sensitive and specific intraoperative neuromonitoring techniques.
*
Regenerative Strategies:
Stem cell therapies, neuroprotective agents, and other novel biologics aimed at improving spinal cord recovery.
*
Robotics and Navigation:
Increasing adoption of robotic assistance and advanced navigation systems for improved screw accuracy and reduced radiation exposure.
*
Biomechanically Optimized Implants:
Development of smarter implants that adapt to bone quality or allow for dynamic stabilization.
The continuous integration of clinical experience with robust scientific evidence remains the cornerstone for providing optimal care to patients with spinal injuries, always striving to master injury assessment and ensure spinal stability and neurological integrity.

Conceptual illustration representing the complex interplay of factors in spinal stability.
