Introduction to the “Terrible Triad” of the Elbow
Originally described by Hotchkiss, the “terrible triad” of the elbow is a complex fracture-dislocation characterized by three distinct but biomechanically linked injuries: an elbow dislocation, a fracture of the radial head, and a fracture of the coronoid process. Historically, this specific constellation of injuries was designated as “terrible” due to uniformly poor clinical outcomes, characterized by chronic instability, severe stiffness, post-traumatic arthrosis, and the frequent need for revision surgeries.
Early studies reporting on elbow dislocations and fracture-dislocations indicated that triad injuries had a dismal prognosis. For instance, early literature by Ring et al. reported fair and poor results in 50% of their patient cohort. However, the paradigm of treatment has shifted dramatically over the last two decades. The advent of standardized, biomechanically sound surgical protocols has revolutionized patient outcomes. Recent literature, including landmark studies by Pugh et al., Egol et al., Forthman et al., and Lindenhovius et al., report good-to-excellent results in 70% to 83% of patients. McKee et al. similarly reported good-to-excellent results in 78% of 36 “terrible triad” injuries treated with a strict, standardized surgical algorithm.
Clinical Pearl: The fundamental goal in treating a terrible triad injury is not merely fracture union, but the restoration of sufficient concentric ulnohumeral and radiocapitellar stability to permit early, active range of motion (ROM). Prolonged immobilization in these injuries universally leads to a stiff, non-functional elbow.
Pathoanatomy and Biomechanics
Understanding the pathoanatomy is critical for successful surgical reconstruction. The essential lesion in a terrible triad injury is the disruption of the lateral collateral ligament (LCL) complex, with a progression of tissue failure from lateral to medial—often referred to as the Horii circle of soft tissue disruption.
The LCL injury typically occurs as an avulsion of its origin from the lateral epicondyle of the distal humerus. This avulsion often takes with it a variable amount of the common extensor musculature, leaving a characteristic "bare-spot" appearance on the lateral distal humerus.
The bony injuries to the radial head and coronoid vary significantly in fragment size, comminution, and complexity, but their loss profoundly destabilizes the elbow:
* The Coronoid Process: Acts as the primary anterior buttress preventing posterior subluxation of the ulna. Even small type I (tip) fractures represent an avulsion of the anterior capsule, leading to significant instability in extension.
* The Radial Head: Acts as a secondary stabilizer to valgus stress and a primary stabilizer to longitudinal forces. In the setting of an LCL tear and coronoid fracture, the radial head becomes a critical anterior and valgus restraint.
Clinical Evaluation and Radiographic Imaging
Patients typically present with a grossly deformed, swollen elbow following a high-energy fall onto an outstretched hand (FOOSH) with the arm in extension and supination.
Standard anteroposterior (AP) and lateral radiographs of the elbow are mandatory. The lateral radiograph must be scrutinized for the "drop sign"—an increase in the ulnohumeral distance indicating persistent subluxation.

FIGURE 57-65 A: Posterior fracture-dislocation with irreparable radial head and neck fractures. The type II coronoid fracture is not immediately apparent on this initial view.

FIGURE 57-65 B: The elbow has redislocated in a posterior splint at 90 degrees of elbow flexion. A large radial head fragment and coronoid fracture are readily apparent. The coronoid fracture must be repaired to provide stability before the radial head can be addressed.

FIGURE 57-66 B: Preoperative radiographic image demonstrating the classic "terrible triad" injury with posterior dislocation, radial head fracture, and coronoid fracture.

FIGURE 57-66 C: Additional preoperative radiographic view highlighting the comminution of the radial head and the loss of the anterior coronoid buttress.
A preoperative computed tomography (CT) scan with 3D reconstructions is highly recommended. CT imaging allows for precise templating of the coronoid fragment size and radial head comminution, which dictates whether the radial head can be fixed or must be replaced.
Principles of Operative Treatment
The standardized surgical protocol developed by Pugh, McKee, and colleagues provides a reliable algorithm for restoring stability.
BOX 57-4: Principles of Operative Treatment of “Terrible Triad” Fracture-Dislocations
* Restore coronoid stability through fracture fixation (type II or III) or through anterior capsular repair (type I).
* Restore radial head stability through rigid fracture fixation or replacement with a metal prosthesis.
* Restore lateral stability through repair of the lateral collateral ligament (LCL) complex and associated secondary constraints (common extensor origin and posterolateral capsule).
* Repair the medial collateral ligament (MCL) in patients with residual posterior instability after lateral-sided reconstruction.
* Apply a hinged external fixator when conventional repair does not establish sufficient joint stability to allow early motion.
Surgical Approaches
The choice of surgical approach depends primarily on the fracture pattern, the type of instability, the extent of soft tissue injury, and surgeon experience.
A universal posterior midline incision is generally preferred by most elbow reconstruction specialists. Large, full-thickness fasciocutaneous flaps are elevated to access both the lateral and medial sides of the elbow without creating narrow skin bridges.
From the lateral side, the Kocher interval (between the extensor carpi ulnaris and the anconeus) or the Kaplan interval (between the extensor digitorum communis and the extensor carpi radialis brevis) can be utilized. Often, the trauma itself dictates the approach; the surgeon should operate through the traumatized planes to minimize further iatrogenic soft tissue dissection.
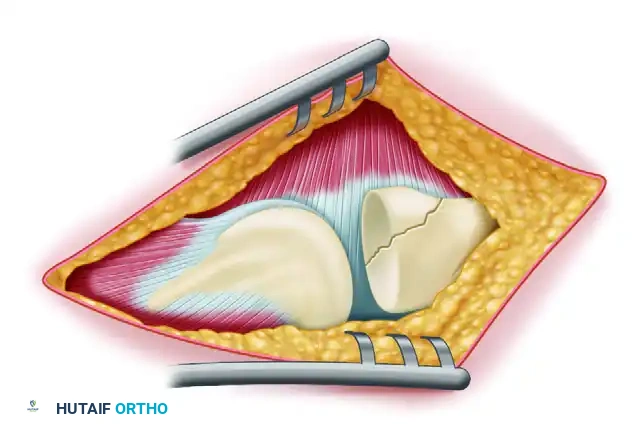
FIGURE 57-67 A: Diagrammatic representation of the lateral approach to the elbow, exposing the radiocapitellar joint and the avulsed lateral structures.
Step-by-Step Surgical Technique: The Deep-to-Superficial Protocol
The fixation strategy must proceed systematically from deep to superficial, as viewed from the lateral approach: Coronoid → Anterior Capsule → Radial Head → Lateral Collateral Ligament → Common Extensor Origin.
Step 1: Joint Access and Debridement
Upon entering the lateral side, the surgeon will typically find the LCL and common extensor origin completely avulsed from the lateral epicondyle.
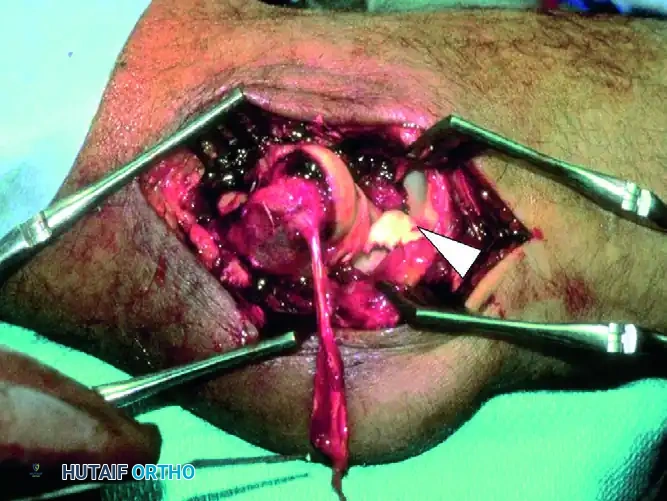
FIGURE 57-66 A: Intraoperative view of a “terrible triad” injury. Note the characteristic stripping of the lateral collateral ligament complex from the distal humerus. A portion of the common extensor origin/lateral ligament complex is hanging down from the bare lateral condyle. The coronoid fragment is trapped in the joint (arrowhead), and the defect in the radial head can be seen behind it.
The joint is irrigated, and fracture hematoma is cleared. If the radial head is irreparably comminuted, it is excised at this stage. Crucially, the radial head prosthesis is not inserted yet. The void left by the excised radial head provides unparalleled visualization of the deep, anteriorly located coronoid process.

FIGURE 57-66 D: Radiograph demonstrating that after radial head resection alone, profound ulnohumeral instability is still present.
Step 2: Coronoid and Anterior Capsule Stabilization
Coronoid fixation is the foundation of terrible triad reconstruction. The method of fixation depends entirely on the size of the fragment.
Small Tip Avulsions (Type I):
Small fragments cannot accept screws. Instead, they are reduced and fixed using heavy nonabsorbable sutures. The sutures are passed through the anterior capsule and the coronoid fragment, then shuttled through drill holes exiting the posterior aspect of the proximal ulna (olecranon). Tying these sutures posteriorly effectively anchors the anterior capsule and coronoid tip back to their anatomic bed, restoring the anterior soft-tissue buttress.
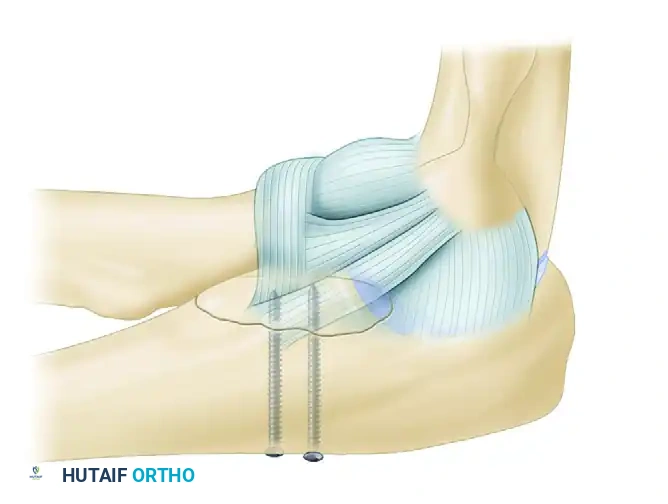
FIGURE 57-62 A: Small coronoid fracture fragments and the attached anterior capsule can be securely fixed with transosseous sutures passed through the proximal ulna.
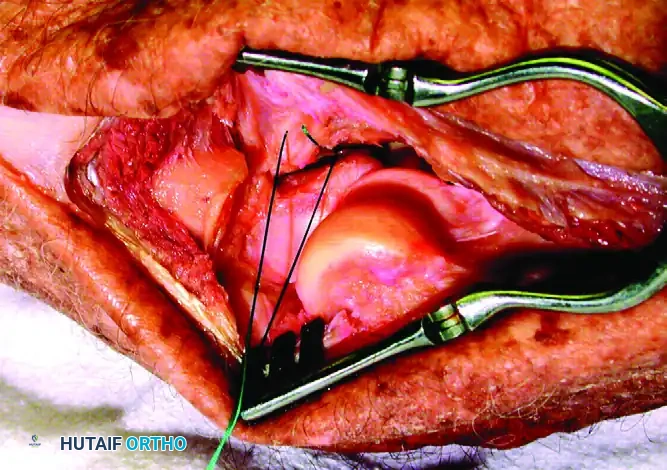
FIGURE 57-67 B: The anterior capsule is captured by nonabsorbable sutures and secured through drill holes in the fracture bed of the coronoid.
Large Fragments (Type II and III):
Larger coronoid fragments provide a critical bony buttress and must be rigidly fixed. This is typically achieved using cannulated lag screws directed from the posterior aspect of the ulna into the coronoid fragment, or occasionally from anterior to posterior if a separate medial approach is utilized.
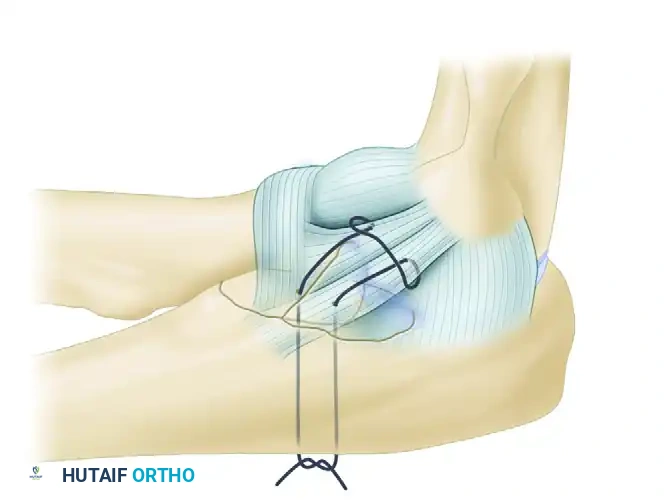
FIGURE 57-62 B: Lag screws can be used to achieve rigid interfragmentary compression for larger coronoid fragments.
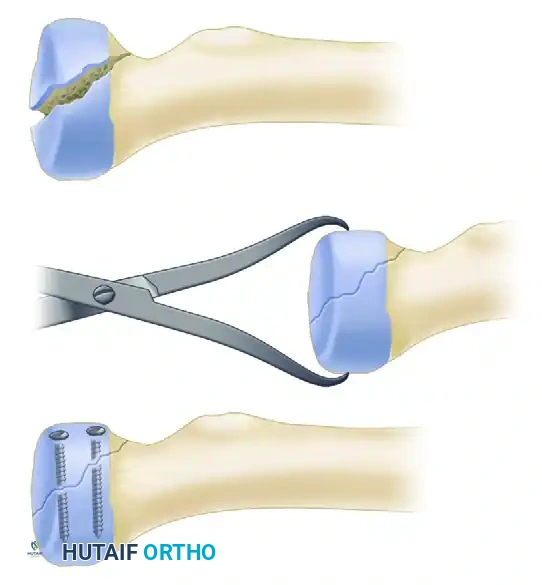
FIGURE 57-67 C: Diagram showing reduction and fixation of a large coronoid fragment with two countersunk screws.

FIGURE 57-66 E: Radiograph showing that even after coronoid suture repair, minor subluxation may still be present until the radial head and LCL are addressed.
Step 3: Radial Head Management
Once the coronoid is secure, attention turns to the radial head. Management is dictated by the ability to obtain an anatomic reduction and whether the bone quality allows the reduction to be maintained under early motion.
- Open Reduction Internal Fixation (ORIF): Indicated for simple fracture patterns (typically <3 fragments) where rigid fixation can be achieved with headless compression screws or a low-profile plate.
- Radial Head Arthroplasty: If the fracture is highly comminuted, cannot be adequately stabilized, or involves the radial neck, replacement with a modular metal prosthesis is mandatory.
Surgical Warning: Never perform a radial head resection without replacement in the setting of a terrible triad injury. The radial head is a critical secondary stabilizer; its absence in a ligamentously compromised elbow will lead to catastrophic posterior subluxation.
When sizing the prosthesis, care must be taken not to "overstuff" the radiocapitellar joint, which can lead to capitellar wear, stiffness, and lateral pain. The prosthesis should sit flush with or slightly proximal to the lateral edge of the lesser sigmoid notch.
Step 4: Lateral Collateral Ligament (LCL) Repair
After coronoid and radial head stabilization, the LCL complex and the common extensor origin must be reattached to their anatomic origin on the lateral epicondyle.
The isometric point of the LCL is located at the center of capitellar curvature. Reattachment is typically performed using robust suture anchors. Krackow or locking whipstitches are placed into the avulsed ligament and tendon complex, and the anchors are deployed into the lateral epicondyle. Reestablishment of these soft tissue restraints adds greatly to the overall posterolateral rotatory stability of the elbow joint.
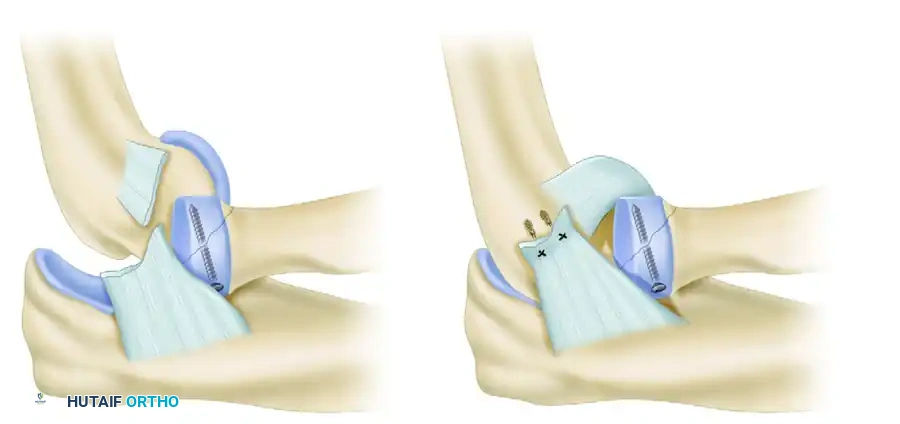
FIGURE 57-67 D: The avulsed lateral ligamentous complex is repaired directly to the bare spot on the lateral condyle using suture anchors.
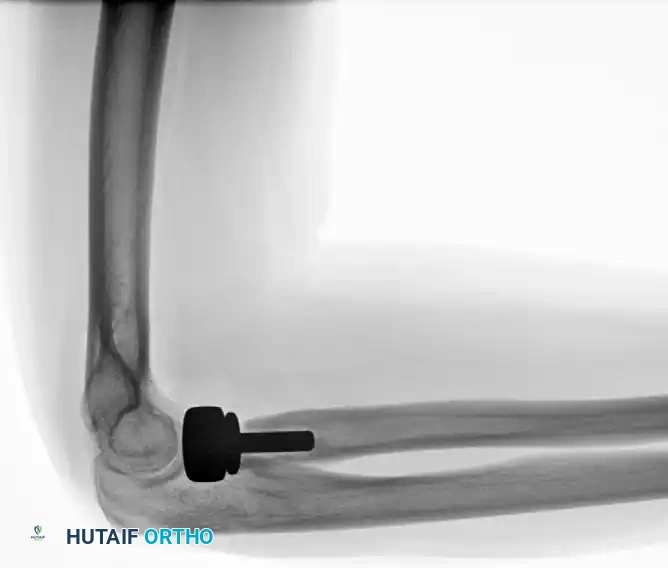
FIGURE 57-66 F: Final postoperative radiograph demonstrating concentric reduction and stability obtained following repair of the coronoid, radial head replacement, and LCL repair.
Step 5: Assessment of Stability and Medial Collateral Ligament (MCL) Repair
Once the lateral side is closed, the elbow is taken through a range of motion to assess stability. The elbow should be stable from 0 to 130 degrees of flexion.
If the elbow subluxates in extension (typically past 30 degrees of extension), the surgeon must address the medial side. A medial incision is made, and the anterior band of the MCL is repaired.
If concentric stability cannot be achieved despite adequate bony and ligamentous reconstruction, a hinged dynamic external fixator must be applied. The external fixator maintains joint congruity while allowing the early active motion necessary for cartilage nutrition and prevention of capsular contracture.
Postoperative Rehabilitation Protocol
The success of a terrible triad reconstruction relies heavily on the postoperative rehabilitation phase. The primary goal is to prevent stiffness while protecting the healing ligaments.
- Immediate Postoperative Phase (Days 1-7): The elbow is placed in a posterior splint at 90 degrees of flexion with the forearm in neutral or slight pronation (to protect the LCL repair).
- Early Active Motion (Weeks 1-6): Supervised active and active-assisted ROM begins within 3 to 7 days postoperatively. Extension is often limited initially (e.g., a 30-degree extension block) to prevent stress on the anterior capsule and coronoid, gradually increasing the extension allowed each week.
- Precautions: Shoulder abduction and internal rotation must be strictly avoided, as this position places maximum varus stress on the healing LCL complex.
- Strengthening (Weeks 8-12): Progressive strengthening begins once radiographic union of the coronoid is confirmed and the ligaments have achieved clinical stability.
Complications and Pitfalls
Despite standardized protocols, complications remain common due to the severe energy imparted to the joint during the initial trauma.
- Stiffness: The most common complication. Loss of terminal extension (10 to 15 degrees) is almost universal and is generally well-tolerated. Severe stiffness may require arthroscopic or open capsular release after 6 to 12 months.
- Heterotopic Ossification (HO): The extensive soft tissue trauma predisposes the elbow to HO. Prophylaxis with Indomethacin or single-dose radiation therapy should be considered in high-risk patients or those with delayed surgical intervention.
- Instability: Recurrent instability is a catastrophic failure usually resulting from inadequate coronoid fixation, an undersized radial head prosthesis, or failure to identify an isometric LCL repair. Revision surgery with potential external fixation is required.
- Ulnar Neuropathy: The ulnar nerve can be contused during the initial trauma or irritated postoperatively. Routine ulnar nerve decompression or transposition is not mandatory but should be performed if preoperative symptoms exist or if extensive medial work is required.
Conclusion
The "terrible triad" of the elbow remains a formidable surgical challenge. However, the historical expectation of poor outcomes has been replaced with cautious optimism. By adhering strictly to a deep-to-superficial surgical algorithm—prioritizing the coronoid buttress, restoring the radiocapitellar column, and anatomically repairing the lateral collateral ligament—orthopaedic surgeons can reliably restore joint congruity. This stable foundation permits the early active motion that is absolutely essential for achieving a functional, pain-free elbow.
