Introduction & Epidemiology
Olecranon fractures are among the more common injuries of the upper extremity, accounting for approximately 1-2% of all fractures and a significant proportion of elbow fractures. The olecranon, as the most proximal extension of the ulna, forms a critical component of the trochlear notch, articulating with the trochlea of the humerus to provide elbow stability and serve as the lever arm for the powerful triceps brachii muscle. Fractures of the olecranon typically result from either direct trauma, such as a fall onto the elbow, or indirect trauma, often an avulsion injury caused by a sudden, forceful contraction of the triceps muscle against a semi-flexed elbow. These injuries primarily affect adults, with a bimodal distribution peaking in young active individuals and again in the elderly due to low-energy falls associated with osteoporosis.
The primary goal of olecranon fracture management is the restoration of a smooth, congruent articular surface, stable fixation to permit early motion, and reconstruction of the extensor mechanism of the elbow. Historically, many non-operative treatments were attempted, but the inherent instability of displaced olecranon fractures, particularly those involving the articular surface, frequently led to poor functional outcomes, including nonunion, malunion, and significant loss of elbow range of motion.
The tension band wiring technique, popularized by the Arbeitsgemeinschaft für Osteosynthesefragen (AO/ASIF) group, represents a cornerstone in the operative management of specific olecranon fracture patterns. This biomechanical principle effectively converts distracting tensile forces, primarily generated by the triceps muscle during elbow flexion, into stable compressive forces across the fracture site. This dynamic compression promotes fracture healing and allows for early, protected mobilization, minimizing the risk of post-traumatic stiffness, a notoriously debilitating complication of elbow trauma. While not universally applicable, tension band wiring remains a highly effective and widely utilized technique for transverse and short oblique olecranon fractures, particularly when combined with robust K-wire fixation.
Surgical Anatomy & Biomechanics
Surgical Anatomy
The olecranon is the prominent posterior projection of the proximal ulna, forming the superior aspect of the trochlear notch. This notch, comprising the olecranon and coronoid processes, articulates with the trochlea of the humerus, forming a highly congruent and inherently stable hinge joint. The olecranon fossa of the humerus accommodates the olecranon during elbow extension, providing bony stability.
Key anatomical considerations for olecranon fracture surgery include:
*
Bony Architecture:
The olecranon tapers distally, transitioning into the diaphysis of the ulna. Its dorsal surface provides the primary attachment for the triceps brachii tendon and its aponeurosis. The articular surface of the trochlear notch is critical for smooth elbow motion and must be anatomically restored.
*
Muscular Attachments:
The triceps brachii tendon inserts broadly onto the dorsal and proximal aspect of the olecranon. This powerful extensor muscle exerts significant tensile forces across the fracture site, which must be counteracted by fixation. The anconeus muscle, often considered part of the triceps mechanism, also originates from the lateral epicondyle and inserts onto the proximal ulna, contributing to elbow extension and posterolateral stability.
*
Neurovascular Structures:
*
Ulnar Nerve:
The ulnar nerve is the most critical neurovascular structure at risk during olecranon surgery. It courses posterior to the medial epicondyle, within the cubital tunnel, and is intimately associated with the medial aspect of the olecranon. Meticulous identification and protection or, if indicated, prophylactic decompression or anterior transposition, are paramount to prevent iatrogenic injury.
*
Posterior Interosseous Nerve (PIN):
While not directly in the surgical field for a posterior olecranon approach, understanding the PIN's location relative to the radial head and neck is important for differential diagnosis in wrist drop scenarios.
*
Brachial Artery and Median Nerve:
These structures are located anterior to the elbow joint and are generally not at risk with a posterior approach, but their overall status must be assessed pre-operatively.
*
Blood Supply:
The olecranon receives its blood supply from multiple anastomoses around the elbow, primarily from branches of the brachial and ulnar arteries.
Biomechanics of the Tension Band Principle
The tension band principle is a fundamental concept in orthopedic trauma surgery, particularly well-suited for the olecranon due to its anatomical location and the forces acting upon it.
- Mechanism of Olecranon Fracture: When the elbow is flexed, the triceps muscle is under tension. A sudden, forceful contraction (e.g., attempting to break a fall with an outstretched arm) can cause an avulsion fracture of the olecranon. Conversely, direct impact causes a "burst" fracture.
- Forces at Play: During elbow flexion, the posterior aspect of the olecranon (the olecranon tip and its triceps attachment) is subjected to significant tensile (distracting) forces. Conversely, the anterior articular surface of the olecranon within the trochlear notch experiences compressive forces. In an olecranon fracture, the triceps muscle tends to pull the proximal fragment superiorly, causing distraction at the fracture site, especially on the posterior aspect.
-
Tension Band Conversion:
The tension band wiring construct converts these tensile forces into beneficial compressive forces across the fracture.
- The K-wires provide stable axial alignment and anti-rotation.
- The figure-of-eight wire, placed dorsally (on the tension side), creates a "tension band." As the triceps contracts and attempts to distract the fracture, the wire, being under tension, pulls the K-wires together. This pulling action, transmitted across the fracture, generates compression at the anterior articular surface (the compression side).
- This dynamic compression is maximal during elbow flexion when the triceps pull is strongest, actively promoting fracture stability and healing.
- Advantages: This load-sharing mechanism allows the bone to participate in load bearing, reducing the stress on the implants and promoting biological healing. It also permits early range of motion, which is crucial for preventing elbow stiffness.
- Limitations: The tension band principle relies on adequate bone stock for K-wire purchase and requires the presence of a "compression side" (the intact anterior cortex or articular surface) to function effectively. It is less suitable for highly comminuted fractures where stable K-wire fixation is difficult or for long oblique/spiral patterns where plate fixation provides more robust control.
Indications & Contraindications
Careful patient selection based on fracture characteristics, patient factors, and surgeon expertise is crucial for successful outcomes with tension band wiring.
Indications for Operative Management (General)
Operative intervention is generally favored for:
*
Displaced Fractures:
Displacement >2 mm, as assessed on radiographs, particularly involving the articular surface.
*
Articular Incongruity:
Any articular step-off >2 mm, which can lead to post-traumatic arthritis.
*
Unstable Fractures:
Fractures that cannot be maintained in an acceptable reduction with non-operative methods (e.g., splinting).
*
Open Fractures:
Require surgical debridement and stabilization.
*
Fractures with Neurological or Vascular Compromise:
Although rare for isolated olecranon fractures, these require immediate surgical attention.
Specific Indications for Tension Band Wiring
Tension band wiring is most effective for:
*
Transverse Fractures:
Simple transverse fractures of the olecranon metaphysis or proximal diaphysis.
*
Short Oblique Fractures:
Fractures with a short oblique component that can be reduced and stabilized with K-wires.
*
Certain Comminuted Fractures:
When the comminution primarily involves the non-articular dorsal cortex and there are still adequate, stable fragments to support K-wire purchase and construct stability.
*
Avulsion Fractures:
Where the triceps insertion has pulled off a significant piece of the olecranon.
Contraindications for Tension Band Wiring
Absolute contraindications for tension band wiring include:
*
Severe Comminution of the Proximal Fragment:
Insufficient bone stock at the olecranon tip to adequately engage the K-wires.
*
Long Oblique or Spiral Fractures:
These patterns are biomechanically less suitable for tension band wiring, as the K-wires may not provide sufficient stability against shear and rotational forces. Plate fixation is generally preferred.
*
Metaphyseal Bone Loss:
Extensive bone loss precluding distal K-wire purchase into the ulnar shaft.
*
Severely Osteoporotic Bone:
Poor K-wire purchase can lead to early construct failure.
*
Active Infection:
Requires eradication prior to definitive internal fixation.
*
Compromised Soft Tissues:
Severe open wounds, significant degloving injuries, or impending skin necrosis may require external fixation as a temporizing measure.
| Parameter | Operative Management | Non-Operative Management |
|---|---|---|
| Displacement | >2 mm (absolute indication for most) | <2 mm displacement |
| Articular Involvement | Articular step-off >2 mm | No articular step-off or minimal |
| Stability | Unstable, unable to maintain reduction | Stable, non-displaced on imaging |
| Fracture Type | Transverse, short oblique, some avulsion/comminuted | Very low-demand patients with minimal displacement |
| Soft Tissues | Adequate for primary closure | Compromised soft tissues (relative contraindication for surgery) |
| Patient Comorbidities | Able to tolerate surgery and anesthesia | Severe medical comorbidities, high anesthetic risk |
| Patient Demand | Active, high-demand individuals | Low-demand, sedentary, often elderly and frail |
| Associated Injuries | Open fractures, neurovascular compromise | Isolated injury without neurovascular deficit |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential to ensure a successful outcome and minimize complications.
Pre-Operative Planning
-
Clinical Assessment:
- Neurovascular Status: A comprehensive neurovascular examination of the affected extremity is paramount. Special attention should be paid to the ulnar nerve, assessing sensation in the small finger and ulnar half of the ring finger, and motor function of the intrinsic hand muscles (e.g., finger abduction/adduction). Document any pre-existing deficits.
- Soft Tissue Integrity: Evaluate the skin for open wounds, abrasions, blistering, or signs of impending skin compromise. Ensure adequate soft tissue envelope for surgical incision and closure.
- Associated Injuries: Rule out other injuries to the elbow, wrist, or shoulder.
- Patient Demands and Comorbidities: Assess patient activity level, functional expectations, and medical comorbidities that may influence surgical timing, anesthetic choice, and rehabilitation.
-
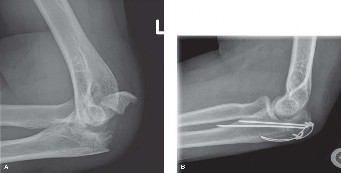
Radiographic Assessment:
- Standard Views: Antero-posterior (AP) and lateral radiographs of the elbow are mandatory. The true lateral view is crucial for assessing displacement, articular step-off, and fracture morphology.
- Oblique Views: Can be helpful to further delineate fracture lines, especially in more complex patterns.
- Computed Tomography (CT) Scan: Highly recommended for comminuted fractures, articular involvement, or suspected coronoid fractures. A CT provides detailed information regarding fragment orientation, articular congruity, and bone stock, which is invaluable for pre-operative templating and surgical strategy.
-
Fracture Classification:
- Mayo Classification: A widely used classification system for olecranon fractures, categorizing them based on displacement, comminution, and elbow stability. Type I (nondisplaced), Type II (displaced), Type III (unstable). Each type is further subdivided into A (non-comminuted) and B (comminuted). This helps guide treatment decisions.
- AO/OTA Classification: Provides a more detailed, alphanumeric classification.
-
Implant Selection and Templating:
- Determine the size and number of K-wires (typically 1.6mm or 2.0mm).
- Select the appropriate gauge of stainless steel wire (commonly 18-gauge [1.25mm] or 20-gauge [1.0mm]).
- Consider the need for ancillary fixation (e.g., small fragment plates, lag screws) in cases of comminution or very osteoporotic bone.
- Ensure all necessary instruments (reduction clamps, drill bits, wire tighteners, K-wire cutters) are available.
- Antibiotic Prophylaxis: Administer pre-operative intravenous antibiotics per institutional protocol (e.g., cefazolin) within 60 minutes of incision.
- Tourniquet Considerations: Plan for a pneumatic tourniquet on the upper arm to provide a bloodless field, typically inflated to 250-300 mmHg or 100 mmHg above systolic blood pressure.
Patient Positioning
- General Anesthesia: Typically preferred for muscle relaxation and patient comfort during prolonged procedures. Regional nerve blocks can be a useful adjunct for post-operative pain control.
-
Positioning Options:
- Lateral Decubitus Position: The patient is positioned on their unaffected side. The operative arm is supported on a sterile padded arm board or allowed to hang free from a spar (if using a fracture table). This provides excellent access to the posterior aspect of the elbow and allows for full range of motion assessment intra-operatively.
- Supine Position: The patient is supine with the operative arm draped over the chest, across the abdomen, or supported on a hand table. A folded towel or bolster under the shoulder can protract the scapula, allowing better access to the medial elbow for ulnar nerve management. When draped across the chest, ensure the arm can be fully flexed and extended without sterile field contamination.
- Fluoroscopy: Position the C-arm to allow for AP and lateral views without repositioning the patient or the arm. This is crucial for confirming reduction and implant placement.
- Tourniquet: Apply a pneumatic tourniquet to the proximal upper arm after appropriate padding.
- Sterile Prep and Drape: A wide sterile field encompassing the shoulder to the hand is recommended to allow for full range of motion assessment and access in case of unexpected surgical needs.
Detailed Surgical Approach / Technique
The goal of olecranon fracture fixation using tension band wiring is to achieve anatomical reduction of the articular surface and provide stable fixation that converts tensile forces into compression, allowing for early rehabilitation.
Incision and Exposure
- Skin Incision: A straight posterior midline incision is typically preferred, centered over the olecranon process. This approach provides excellent exposure and minimizes the risk of injury to the cutaneous nerves, particularly the medial antebrachial cutaneous nerve, while respecting the skin tension lines. The incision should be long enough to allow for adequate visualization and instrument manipulation without excessive retraction.
-
Soft Tissue Dissection:
- Carefully incise the skin and subcutaneous tissue. Raise full-thickness skin flaps (skin and subcutaneous tissue together) medially and laterally to protect the underlying ulnar nerve and maintain adequate soft tissue coverage for closure.
- Ulnar Nerve Identification and Protection: The ulnar nerve is highly vulnerable during this approach. It typically runs within the cubital tunnel posterior to the medial epicondyle. It is imperative to identify the ulnar nerve proximally and distally to the cubital tunnel and protect it throughout the procedure. Some surgeons routinely decompress the ulnar nerve by incising the cubital tunnel retinaculum, while others perform prophylactic anterior transposition, particularly if the nerve is found to be unstable or under tension. However, routine transposition is not universally recommended unless specific indications exist. The nerve should be gently retracted medially or laterally with a vessel loop.
- Fracture Exposure: The triceps aponeurosis is incised longitudinally along the line of the fracture, or split bluntly to expose the fracture fragments. Clear any hematoma and debris from the fracture site. Irrigate copiously.
Fracture Reduction
- Visualization: Achieve direct visualization of the articular surface through the fracture gap. This is critical to ensure anatomical reduction.
- Reduction Maneuver: Use pointed reduction clamps (e.g., Verbrugge clamps, small bone clamps) or pointed reduction forceps to grasp the proximal and distal fragments and anatomically reduce the fracture. Apply gentle traction on the forearm to help disengage impacted fragments.
- Articular Congruity: Confirm articular congruity by direct visual inspection and palpation across the articular surface. The goal is a perfectly smooth articular surface, without any step-off or gap.
- Temporary Fixation: Once anatomical reduction is achieved, maintain it with temporary K-wires inserted obliquely or transversely, away from the planned definitive K-wire and tension band paths. Fluoroscopy in both AP and lateral planes is essential to confirm reduction before definitive fixation.
Definitive Fixation: Tension Band Wiring
The classical tension band wiring technique involves two parallel K-wires and a figure-of-eight stainless steel wire.
-
K-wire Placement:
- Select two K-wires (typically 1.6mm or 2.0mm diameter, depending on bone quality and fragment size).
- Insert the K-wires from the tip of the olecranon, parallel to each other, across the fracture site, and into the distal ulnar shaft. The wires should be positioned just lateral to the ulnar ridge, equidistant from the medial and lateral cortices, and ideally, diverge slightly as they cross the fracture site to enhance rotational stability.
- Crucially, the K-wires must engage the anterior cortex of the ulna. Advance them until they just penetrate the anterior cortex. Avoid over-penetration, which can irritate the neurovascular structures or surrounding soft tissues.
- Ensure the K-wires are not placed directly in the articular surface.
- Confirm K-wire position and length with fluoroscopy in AP and lateral views.
-
Transverse Drill Hole (for the tension band wire):
- A transverse drill hole (typically 2.5mm or 3.2mm, depending on wire gauge) is made approximately 2-3 cm distal to the fracture site, crossing the ulnar cortex. This hole should be positioned on the dorsal surface of the ulna, but sufficiently distal to avoid undermining the fracture. In very proximal fractures or where the distal fragment is short, the wire may be passed directly under the triceps tendon insertion instead of through a drill hole.
-
Figure-of-Eight Wire Placement:
- Pass the stainless steel wire (18-gauge or 20-gauge) through the transverse drill hole from one side to the other.
- Loop each end of the wire around one of the K-wires proximally, creating a figure-of-eight configuration. The wire should lie superficial to the K-wires on the dorsal aspect of the olecranon.
- The wire loops around the proximal ends of the K-wires, which will later be bent and cut.
-
K-wire Bending and Impaction:
- The proximal ends of the K-wires are bent 180 degrees into a small hook, typically about 1 cm from the olecranon tip. This bend prevents migration of the K-wires and provides a stable point for the tension band wire to hook onto.
- Cut the K-wires approximately 5-7 mm from the bend.
- Impact the bent ends of the K-wires slightly into the cancellous bone of the olecranon tip, ensuring they are subcortical to minimize skin irritation and potential migration.
-
Tensioning the Figure-of-Eight Wire:
- With the elbow held in extension (which places the triceps under the least tension), gradually tighten the figure-of-eight wire. This can be done by twisting the two ends of the wire together, using a wire tightener, or a combination.
- Tighten the wire incrementally, ensuring reduction is maintained. Avoid over-tightening, which can cause K-wire bending or cut-out in osteoporotic bone.
- The twists should be uniform and create a strong knot, typically placed on the lateral side, away from the ulnar nerve to minimize irritation.
- Confirm final reduction and stability under fluoroscopy and by gently moving the elbow through a full range of motion. The construct should be stable, and the articular surface should remain congruent.
-
Adjunctive Fixation (if necessary):
- In cases of significant comminution or very osteoporotic bone, the tension band construct may be augmented with a small fragment plate (e.g., one-third tubular plate) applied laterally or a lag screw for larger, oblique fragments. This can enhance rotational stability and prevent K-wire pullout.
Closure
- Irrigation: Copiously irrigate the wound to remove any bone fragments, debris, or hematoma.
- Triceps Repair: If the triceps aponeurosis was significantly incised or disrupted, it should be repaired with absorbable sutures to reconstruct the extensor mechanism.
- Layered Closure: Close the subcutaneous tissues with absorbable sutures and the skin with non-absorbable sutures or staples.
- Dressing and Splint: Apply a sterile dressing. A posterior long arm splint, typically set at 90 degrees of elbow flexion, is applied to protect the fixation for 1-2 weeks until initial soft tissue healing occurs.
Complications & Management
While tension band wiring is a highly effective technique for olecranon fractures, it is not without its specific complications. Awareness of these issues and appropriate management strategies are crucial for optimal patient outcomes.
| Complication | Incidence (Approximate) | Management / Salvage Strategy |
|---|---|---|
| Hardware Prominence/Irritation | 30-80% | Most common complication. Typically managed by elective hardware removal after fracture healing (usually 6-12 months post-op). Symptomatic patients may require earlier removal, but careful consideration is given to fracture consolidation. |
| Loss of Reduction/Fixation Failure | 5-15% | Occurs due to inadequate reduction, poor bone quality, or premature aggressive rehabilitation. Management depends on the degree of displacement and time from surgery. Options include revision internal fixation (often with plate and screws), bone grafting for nonunion, or in severe cases, excision of the olecranon (for small distal fragments in low-demand elderly) or total elbow arthroplasty . |
| Nonunion/Malunion | 5-10% | Can result from fixation failure, infection, or compromised biology. Nonunion often manifests as pain and instability. Malunion can lead to limited ROM and post-traumatic arthritis. Management for nonunion typically involves revision ORIF with bone grafting (autograft or allograft). Malunion may require osteotomy and revision fixation if symptomatic and functionally limiting. |
| Ulnar Nerve Irritation/Neuropathy | 5-20% | Can occur due to direct injury during surgery, nerve compression within the cubital tunnel (especially after swelling), hardware irritation, or excessive stretch. Management ranges from observation for mild symptoms, anti-inflammatory medications , nerve decompression (cubital tunnel release), to anterior transposition if symptoms persist or are severe. Hardware removal may be indicated if directly impinging on the nerve. |
| Elbow Stiffness/Loss of ROM | 20-50% | Multifactorial, including prolonged immobilization, pain, post-traumatic capsular contracture, and heterotopic ossification. Management includes intensive physical therapy , dynamic or static progressive splinting , manipulation under anesthesia , or arthrolysis (surgical release of contractures) if conservative measures fail. Early, protected motion is key to prevention. |
| Infection | 1-5% | Can be superficial or deep. Superficial infections typically respond to oral antibiotics . Deep infections require surgical debridement , intravenous antibiotics , and potentially implant removal if the infection is persistent or jeopardizes fracture healing. Retention of hardware is sometimes attempted with debridement and prolonged antibiotics, but high-grade infections often necessitate removal. |
| Post-traumatic Arthritis | 10-30% (long-term) | Can develop due to articular incongruity, cartilage damage at the time of injury, or malunion. Management is initially conservative (NSAIDs, activity modification, injections). For severe, debilitating arthritis, surgical options include arthroplasty (hemi or total elbow) or excision arthroplasty . |
| Complex Regional Pain Syndrome (CRPS) | <1% | A severe, chronic pain condition. Management is multidisciplinary, involving pain specialists , physical therapy , pharmacotherapy (neuropathic agents), and sometimes nerve blocks or spinal cord stimulators . Early recognition and aggressive treatment are vital. |
Specific Considerations for Management
- Hardware Removal: This is the most frequently performed secondary procedure after tension band wiring. Patients often experience discomfort from the prominent K-wire ends or the overlying wire. It is typically deferred until at least 6-12 months post-injury to ensure robust fracture healing. Removal is generally straightforward and yields high patient satisfaction rates.
- Revision Surgery: For loss of reduction or nonunion, the choice of revision technique depends on the remaining bone quality, fracture pattern, and presence of infection. Often, plate fixation with lag screws provides more rigid stability for complex situations or when the tension band has failed. Bone grafting is frequently utilized for nonunions.
- Ulnar Nerve Protection: Prophylactic cubital tunnel release or anterior transposition at the time of initial fracture fixation is a point of debate. While it adds surgical time and potential morbidity, it may be warranted in cases of pre-existing ulnar nerve symptoms, severe swelling, or a very unstable nerve. Careful intraoperative identification and protection are paramount.
Post-Operative Rehabilitation Protocols
A well-structured and individualized post-operative rehabilitation protocol is crucial for maximizing functional recovery and minimizing stiffness after olecranon tension band wiring. The goal is to safely initiate early, protected range of motion to prevent adhesions and maintain cartilage health while protecting the healing fracture and fixation construct.
Phase 1: Immediate Post-Operative / Protection Phase (Weeks 0-2)
- Goal: Protect fixation, control pain and swelling, initiate gentle motion.
-
Immobilization:
- The elbow is typically immobilized in a posterior long arm splint at approximately 90 degrees of flexion (or a comfortable angle, generally 70-90 degrees) for the first 1-2 weeks. This provides comfort, reduces swelling, and protects the early fixation.
- Some surgeons may use a hinged elbow brace immediately, locked for the first week.
-
Pain and Edema Control:
- Elevation of the limb, cryotherapy, and prescribed analgesics are essential.
-
Early Motion:
- As soon as pain allows and wound healing permits (often within 3-7 days), the splint may be removed for supervised, gentle active and passive range of motion (ROM) exercises.
- Active ROM: Gentle active flexion/extension, forearm pronation/supination.
- Passive ROM: Gentle gravity-assisted flexion and active extension. Avoid passive forced manipulation.
- Range Restrictions: Typically limited to a safe arc, e.g., 30-90 degrees or as tolerated, gradually increasing. Avoid full extension initially, especially against resistance, to protect the triceps repair and tension band construct.
- Activity Restrictions: No lifting, pushing, pulling, or weight-bearing through the arm. No sudden movements.
Phase 2: Early Mobilization / Strengthening Phase (Weeks 2-6)
- Goal: Gradually increase ROM, initiate light strengthening, protect bone healing.
- Brace Application: Transition to a hinged elbow brace (if not already used) set to gradually increase the allowed range of motion. For example, starting at 30-100 degrees and increasing 10-15 degrees per week as tolerated.
-
ROM Progression:
- Continue active and passive ROM exercises. The focus is on regaining full extension and flexion.
- Gentle joint mobilization techniques may be initiated by a therapist.
- Dynamic or static progressive splinting may be considered for persistent ROM deficits, particularly extension.
-
Strengthening:
- Begin with gentle isometric exercises for elbow flexors and extensors, forearm pronators/supinators, and wrist/hand muscles.
- Progress to very light isotonic resistance exercises (e.g., with light resistance bands or weights, typically <1-2 lbs).
- Focus on maintaining good form and avoiding pain.
- Activity Restrictions: Continue to avoid heavy lifting, forceful movements, and impact activities.
Phase 3: Progressive Strengthening & Functional Phase (Weeks 6-12+)
- Goal: Restore full ROM, progressively increase strength, prepare for return to activity.
- ROM: Most patients should achieve near-full or full ROM by this stage. Address any remaining deficits with continued therapy.
-
Strengthening:
- Gradually increase resistance and intensity of strengthening exercises.
- Incorporate eccentric exercises for elbow musculature.
- Begin closed-chain exercises (e.g., wall push-ups) as appropriate.
- Focus on functional movements relevant to the patient's daily activities, work, or sport.
- Proprioception and Neuromuscular Control: Introduce exercises to improve joint position sense and coordination.
-
Activity Progression:
- Gradual return to light activities of daily living.
- Work-specific tasks and sport-specific training can begin under guidance, with emphasis on proper body mechanics.
- Radiographic Assessment: Regular radiographic follow-up is important to monitor fracture healing and ensure no loss of reduction.
- Hardware Removal Consideration: Discuss hardware removal with the patient once fracture healing is consolidated (typically after 6-12 months) if symptomatic.
General Considerations
- Individualization: Protocols must be tailored to the individual patient, considering fracture stability, bone quality, soft tissue healing, pain tolerance, and pre-injury activity level.
- Patient Education: Patients should be thoroughly educated on the importance of adherence to the protocol, signs of complications, and realistic expectations regarding recovery.
- Communication: Close communication between the surgeon and the physical therapist is paramount to adjust the protocol as needed based on patient progress and radiographic healing.
- Avoidance of Overuse: Emphasize a gradual progression and avoiding activities that cause pain or excessive stress on the healing fracture.
Summary of Key Literature / Guidelines
The tension band wiring technique for olecranon fractures has a long and well-established history in orthopedic surgery, with its principles derived from the seminal work of the AO/ASIF group. The extensive literature generally supports its efficacy for appropriate fracture patterns, particularly simple transverse and short oblique fractures.
Core Principles and Outcomes:
*
AO Principles:
The primary aim of olecranon fixation, according to AO principles, is stable internal fixation allowing for early functional rehabilitation. Tension band wiring achieves this by converting distractive forces into compression at the articular surface, promoting healing and preventing stiffness.
*
Functional Outcomes:
Numerous studies report good to excellent functional outcomes, with union rates typically above 90-95%. A systematic review by Chalidis et al. (2008) highlighted favorable functional outcomes, with most patients achieving a good range of motion, albeit with a high rate of hardware removal.
*
Hardware-Related Complications:
The most frequently cited drawback of tension band wiring is hardware prominence and subsequent irritation, requiring elective hardware removal in a significant percentage of patients (30-80%). This rate is notably higher than for plate fixation. However, hardware removal is generally a minor procedure with good results.
*
Comparison with Plate Fixation:
* For simple transverse and short oblique fractures, tension band wiring offers equivalent or superior biomechanical stability to simple plate fixation and is less invasive than extensive plating. It is generally less expensive and quicker to perform.
* For comminuted fractures, especially those with multiple fragments or osteoporotic bone, locked plating constructs or precontoured olecranon plates are often biomechanically superior, providing greater stability against rotational forces and preventing K-wire cutout. Tension band wiring alone may be insufficient in these complex cases. Hybrid constructs combining a tension band with a small plate can be considered for specific comminuted patterns.
* A meta-analysis by Zeng et al. (2015) suggested that while both methods achieve good union rates, plate fixation might offer a slight advantage in preventing loss of reduction for more complex patterns, but at the cost of longer surgical time and potentially higher rates of infection, although hardware removal rates remain similar.
Key Studies and Developments:
*
Classic Studies:
Early work by Schatzker, Muller, and the AO Foundation laid the groundwork for the biomechanical understanding and surgical technique of tension band wiring. Their work emphasized the importance of anatomical reduction and stable fixation for early mobilization.
*
Biomechanical Studies:
Biomechanical comparisons have shown that tension band wiring effectively generates dynamic compression. Studies often compare the strength of tension band constructs to various plate constructs, generally concluding that for simple fractures, TBW is robust, but for complex fractures, plates offer more rigid fixation.
*
Evolution of Technique:
Refinements include using divergent K-wires for increased rotational stability, careful impaction of K-wire ends to reduce skin irritation, and the judicious use of adjunct mini-plates or lag screws for comminuted fragments. The debate regarding routine ulnar nerve transposition remains active, with most current evidence not supporting routine transposition unless specific indications exist (e.g., preoperative neuropathy, unstable nerve, or significant intraoperative tension).
Guidelines and Current Consensus:
*
Appropriate Application:
Tension band wiring remains the gold standard for simple, transverse, or short oblique olecranon fractures that can be anatomically reduced and provide sufficient bone stock for K-wire purchase.
*
Patient Selection:
Patient factors such as age, activity level, and bone quality play a significant role. In severely osteoporotic elderly patients, a tension band may not provide sufficient purchase, and a locking plate may be preferred. Conversely, in low-demand elderly patients with small distal fragments, fragment excision and triceps advancement may be considered.
*
Early Mobilization:
The overarching principle for all stable olecranon fixations is early, protected range of motion to prevent post-traumatic stiffness, which is a common and debilitating complication of elbow trauma.
In summary, tension band wiring, when applied to carefully selected olecranon fractures, offers a highly effective and biomechanically sound method of fixation. While the high rate of hardware removal is a known drawback, the technique consistently achieves excellent union rates and functional outcomes, making it a cornerstone in the orthopedic surgeon's armamentarium for treating these common injuries. Ongoing research continues to refine indications and compare its efficacy with evolving plating technologies.
