DEFINITION
Radial nerve palsy that is distal to the triceps innervation affects the forearm musculature. A lesion that does not recover results in predictable wrist, finger, and thumb extensor deficits.
ANATOMY




FIG 1 • A. Muscles of the forearm. B. Course of the radial nerve. The motor point for each nerve is fairly consistently located just proximal to the myotendinous junction. In most cases, there is one larger motor branch from the radial nerve or PIN to each muscle.The sequence of muscle innervation is an important distinction when considering the anatomy of the radial nerve. Whereas some nerves distribute their nerve branches in a tree-like fashion, the radial nerve innervates the extensor musculature in an orderly pattern, from proximal to distal. The proper radial nerve supplies the BR, the ECRL, and occasionally the ECRB.P.894The PIN innervates the ECRB, the extensor digitorum communis (EDC), the extensor carpi ulnaris (ECU), the extensor indicis proprius (EIP), and the extensor pollicis longus (EPL).The order of innervation is important in differentiating a radial nerve injury from a mechanical myotendinous injury or muscle disruption after a forearm laceration.Understanding the innervation also is helpful while observing and assessing the clinical recovery after radial nerve injury or repair.
PATHOGENESIS
Most radial nerve deficits result from traumatic injuries. Idiopathic and neoplastic etiologies are less common. Radial nerve injury is most commonly associated with midto distal shaft humerus fractures.1,5,25,26,29
NATURAL HISTORY
The type of traumatic injury is an important predictor of recovery after humerus trauma.Neurapraxic lesions typically result from low-energy injuries. Recovery can be expected over the course of 3 months. The clinical recovery can be followed by observing the advancing Tinel sign and the previously described reinnervation sequence.Conditions that persist after 3 months can be further evaluated with electrodiagnostic studies. In the clinical setting of a nonadvancing Tinel sign and electromyographic findings of axonal loss, exploration with intraoperative electrophysiologic testing is warranted. Nerve grafting across the injury is indicated in lesionsthat do not demonstrate improvement after external neurolysis.19,25,26Exploration of open and penetrating injuries is recommended. The choice of primary repair or nerve grafting depends on the injury zone. Recent evidence warrants exploration of highenergy injuries because these lesions have not demonstrated recovery. It is difficult to determine the injury at the acute setting. Interposition nervegraft is often necessary.19
PATIENT HISTORY AND PHYSICAL FINDINGS
A deficit in radial nerve innervation of the extrinsic wrist and finger extensors results in no active wrist, finger, and thumb extension.The clinical presentation of radial nerve and PIN palsies is differentiated by the fact that the BR and ECRL are preserved in PIN palsies. Thus, a patient with a PIN deficit will have some retained composite wrist radial deviation and extension, whereas a radial nerve lesion proximal to the elbow will not have a voluntary wrist extension.The BR can be palpated during resisted, neutral position elbow flexion, and the wrist assumes a radial-deviatedposition during attempted active extension.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Electrodiagnostic studies (eg, nerve conduction studies and electromyography) are used initially for assessment and for determining subsequent treatment.Axonal loss injuries are evident about 4 weeks after the injury; therefore, the initial study is obtained until at least 4 to 6 weeks after the injury.The electrodiagnostic study also can identify other nerve injuries that were not as evident on the initial evaluation.Recovery can be followed by clinical examination or with supplemental studies. Reinnervation or polyphasic waveforms are seen in the muscles of a regenerating nerve.A final study is obtained before tendon transfer at 12 to 18 months.
DIFFERENTIAL DIAGNOSIS
Muscle or tendon laceration Closed myotendinous rupture Cervical spinal diseaseJoint or tendon subluxation (especially if there is lost digital extension)
NONOPERATIVE MANAGEMENT
Wrist and finger extension splint, especially a wrist extension splint initially after the injury, to counteract the wrist flexion position. Some finger extension can be afforded with the hand intrinsics.Active and passive motion exercises to maintain motion and prevent contracture29 while the nerve is regenerating and in event that transfers may be necessary
SURGICAL MANAGEMENT
Tendon transfer is the mainstay of treatment. Microvascular repair and nerve graft are discussed in another chapter.The goal of treatment is independent wrist, finger, and thumb extension with thumb abduction. Donor muscles include the pronator teres (PT), flexor carpi ulnaris (FCU), flexor carpi radialis (FCR), flexor digitorum superficialis (FDS) 3 and 4, and palmaris longus (PL).Timing of surgical intervention is controversial. Conventional surgical recommendations are to proceed after the patient has reached a documented clinical and electromyographic plateau of useful radial nerve regeneration.This typically occurs 1 year after the nerve lesion.26 Tendon transfer primarily for wrist extension may be performed early, at the same setting as nerve surgery, to improve function and minimize brace reliance as the nerve regenerates. In securing the tendon transfer, two methods can be used. The more traditional method is a Pulvertaft weave in which the donor tendon is passed through the recipient tendon three times at respective right angles. The tension is set with appropriate tension on the donor and recipient tendons. The weave is secured with multiple mattress and figure-8 sutures. Another method involves one pass of the donor tendon through the recipient tendon, with then a side-to-side coaptation of the two tendons over 3 to 5 cm with a running, locking suture. The side-to-side transfer has demonstrated better biomechanical characteristics butrequire greater recipient tendon for the transfer. The surgeon needs to be familiar with both methods as they can be used in specific locations as it relates to the patient anatomy.4
PREOPERATIVE PLANNING
PrerequisitesGrade 4+ or 5 median or ulnar nerve-innervated donor musculatureMaintained passive motion in wrist and finger extension with no contracture Controlled systemic disease processes
POSITIONING
The patient is positioned supine with arm table support and a tourniquet.
APPROACH
Three general exposures are used:P.895Radial incision with volar exposure for FCR and PT and dorsal exposure for the ECRB and ECRL Distal dorsal incision for EDC exposureIndividual approaches for harvest of the FCU, FCR, and FDSThe ideal tendon transfer tension is based on the individual muscle properties. In general, the optimal tension is established at the peak of the length-tension curve for the donor muscle while the wrist and fingers are maintained in the ideal position. Because this donor muscle position is difficult to determine intraoperatively without specialized equipment, this point reasonably corresponds to the midpoint of the passive muscle excursion. The ideal joint position for each transfer is discussed with the individual transfers.
TECHNIQUES
Wrist Extension Restoration through Pronator Teres to Extensor Carpi Radialis Ligament and Extensor Carpi Radialis Brevis2,9,28****






TECH FIG 1 •(continued)E,F. The PT is then woven through the ECRL and ECRB tendons.
Finger Extension through Flexor Carpi Ulnaris to Extensor Digitorum Communis Transfer8,17,20,21****


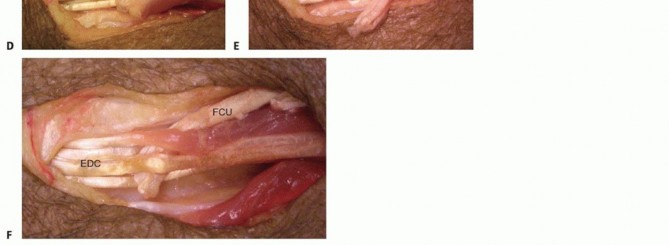






TECH FIG 3 •(continued)I,J. The transfer is secured with 3-0 nonabsorbable suture.
Thumb Extension through Palmaris Longus to Extensor Pollicis Longus2,18,22****


Digitorum Superficialis to Extensor Indicis Proprius/Extensor Pollicis Longus; Ring Finger Flexor Digitorum Superficialis to Long, Ring, and Small Extensor Digitorum Communis; and Palmaris Longus to Abductor Pollicis Longus6,10**** Perform oblique palmar incisions to harvest the FDS of the long and ring fingers.Include both slips for transfer.Suture the remaining distal tendon to the volar plate or soft tissue to prevent proximal interphalangeal hyperextension.Use the volar incision to retrieve the FDS tendons and to harvest the PL.Precisely expose the IOM and make preparations for tendon transfer as discussed in the preceding section.Perform a dorsal incision and EDC exposure similar to that detailed in the preceding section. Transfer the two FDS tendons dorsally through the IOM.The long finger FDS is transferred to the EIP and the EPL. The ring finger FDS is transferred to the long, ring, and small EDC tendons.Set tension at the wrist at 30 degrees and at the MP joint at full extension. Secure the transfer with 3-0 or 4-0 suture.The PL is harvested as detailed for the EPL transfer.The radial subcutaneous route also is used to transfer the PL to the abductor pollicis longus (APL), proximal to the retinaculum.The location of this transfer is slightly more proximal to the PL than the EPL transfer due to the length available for the APL.Set tension in near-full thumb abduction at wrist 30 degrees; secure with 3-0 or 4-0 suture.5. Finger Extension and Thumb Abduction through Flexor Carpi Ulnaris to Extensor Digitorum Communis and Extensor Pollicis Longus and Palmaris Longus to Abductor Pollicis LongusAlthough one donor muscle is not typically transferred to two recipients,3 an FCU transfer to the EPL and EDC has been described. This may be combined with a wrist extension transfer.The technique is similar to that discussed for the FCU to EDC transfer along the ulnar subcutaneous route. The tension is such that the thumb and index metacarpal are parallel.PEARLS AND PITFALLS
|Donor ▪ In setting tendon transfer tension, the donor muscle length-tension properties are muscle important to consider. A good clinical approximation of a muscle at the peak of the properties length-tension curve is to place the muscle near the 50% excursion point. The distalrecipient tendon is then pulled proximally until the ideal position of the joints has been achieved.12||Pulvertaft ▪ In performing a Pulvertaft weave, a curved tendon passer is very helpful. The weaves weave should be placed at 90 degrees to each other and secured with multiple mattresssutures. The sutures should have small purchase into the donor and recipient tendons to prevent necrosis. At least three weaves should be used.Goals ▪ With finger extension transfers, it is important to determine the preoperative goals for the FCU/FCR transfers because they do not match the total EDC excursion.Preoperative assessments can determine whether the ideal working range of the transfer should be more in wrist extension or flexion because the force will be less in the opposite position.12Choice of ▪ The choice between the most common extensor transfers—FCR or FCU—is difficult. transfer Usually, the FCU generates greater force and has longer sarcomere excursion andgreater fiber length variability. It has better potential excursion than the FCR, but an extensive proximal release is necessary. Because of muscle bulk, the ulnar route is easier to do than the interosseous passage. There may be some loss of ulnar deviation and grip strength as compared to FCR, but it does not appear to havefunctional implications.17,23|------P.900
POSTOPERATIVE CARE
Postoperative splint with wrist at 30 to 40 degrees and MP joints in 0 to 10 degrees of hyperextension Proximal and distal interphalangeal active and passive motion at 3 to 5 daysStatic immobilization for 3 weeks, then tenodesis motions with activation of wrist extension transfer Integration of finger and thumb active extension as wrist motion improvesThe most difficult motion to obtain is independent finger extension with the wrist in the extended position.Passive wrist flexion exercises are determined by the recovery of wrist flexion after splint removal. The arc of flexion can be expected to be less than the preoperative level.A dynamic splint may be applied so that finger extension may begin at 1 week postoperative. An articulated splint may be used to permit dynamic wrist motion, but the patient must be very adept and have a clear understanding of the therapy regimen.24,29
OUTCOMES
Wrist extension of 40 to 50 degrees (80% M4), wrist flexion 20 to 40 degreesFinger extension: at wrist neutral, 0 to 10 degrees flexion; at wrist in 30 degrees of extension, 0 to 30 degreesFunctional scores: 80% excellent to good22; no reported disabilities of the arm, shoulder, or hand
COMPLICATIONS
If transfer adhesions occur, the therapy can be modified according to postoperative course. Tenolysis should be delayed until at least 9 to 12 months after surgery.Transfer attenuation
REFERENCES
- Amillo S, Barrios RH, Martínez-Peric R, et al. Surgical treatment of the radial nerve lesions associated with fractures of the humerus. J Orthop Trauma 1993;7:211-215.
- Boyes JH. Selection of a donor muscle for tendon transfer. Bull Hosp Joint Dis 1962;23:1-4.
- Brand PW. Biomechanics of tendon transfer. Orthop Clin North Am 1974;5:205-230.
- Brown SH, Hentzen ER, Kwan A, et al. Mechanical strength of the side-to-side versus Pulvertaft weave tendon repair. J Hand Surg Am 2010;35(4):540-545.
- Burkhalter WE. Early tendon transfer in upper extremity peripheral nerve injury. Clin Orthop Relat Res 1974; (104):68-79.
- Chuinard RG, Boyes JH, Stark HH, et al. Tendon transfers for radial nerve palsy: use of superficialis tendons for digital extension. J Hand Surg Am 1978;3:560-570.
- Gousheh J, Arasteh E. Transfer of a single flexor carpi ulnaris tendon for treatment of radial nerve palsy. J Hand Surg Br 2006;31:542-546.
- Ishida O, Ikuta Y. Analysis of Tsuge's procedure for the treatment of radial nerve paralysis. Hand Surg 2003;8:17-20.
- Kozin SH, Hines B. Anatomical approach to the pronator teres. Tech Hand Up Extrem Surg 2002;6:152-154.
- Krishnan KG, Schackert G. An analysis of results after selective tendon transfers through the interosseous membrane to provide selective finger and thumb extension in chronic irreparable radial nerve lesions. J Hand Surg Am 2008;33:223-231.
- Kruft S, von Heimburg D, Reill P. Treatment of irreversible lesion of the radial nerve by tendon transfer: indication and long-term results of the Merle d'Aubigné procedure. Plast Reconstr Surg 1997;100:610-616.
- Lieber RL, Pontén E, Burkholder TJ, et al. Sarcomere length changes after flexor carpi ulnaris to extensor digitorum communis tendon transfer. J Hand Surg Am 1996;21:612-618.
- Lim AY, Lahiri A, Pereira BP, et al. Independent function in a split flexor carpi radialis transfer. J Hand Surg Am 2004;29:28-31.
- Lowe JB III, Sen SK, Mackinnon SE. Current approach to radial nerve paralysis. Plast Reconstr Surg 2002;110:1099-1113.
- Omer GE. Tendon transfers for combined traumatic nerve palsies of the forearm and hand. J Hand Surg Br 1992;17:603-610.
- Omer GE Jr. Tendon transfers in combined nerve lesions. Orthop Clin North Am 1974;5:377-387.
- Raskin KB, Wilgis EF. Flexor carpi ulnaris transfer for radial nerve palsy: functional testing of long-term results. J Hand Surg Am 1995; 20:737-742.
- Reid RL. Radial nerve palsy. Hand Clin 1988;4:179-185.
- Ring D, Chin K, Jupiter JB. Radial nerve palsy associated with highenergy humeral shaft fractures. J Hand Surg Am 2004;29:144-147
- Riordan DC. Radial nerve paralysis. Orthop Clin North Am 1974; 5:283-287.
- Riordan DC. Tendon transfers in hand surgery. J Hand Surg Am 1983;8:748-753.
- Ropars M, Dréano T, Siret P, et al. Long-term results of tendon transfers in radial and posterior interosseous nerve paralysis. J Hand Surg Br 2006;31:502-506.
- Skie MC, Parent TE, Mudge KM, et al. Functional deficit after transfer of the pronator teres for acquired radial nerve palsy. J Hand Surg Am 2007;32:526-530.
- Skoll PJ, Hudson DA, de Jager W, et al. Long-term results of tendon transfers for radial nerve palsy in patients with limited rehabilitation. Ann Plast Surg 2000;45:122-126.
- Sunderland S. Decision making in clinical management of nerve injury and repair. In: Sunderland S, ed. Nerve Injuries and Their Repair. Edinburgh: Churchill Livingstone, 1991:413-431.
- Thomsen NO, Dahlin LB. Injury to the radial nerve caused by fracture of the humeral shaft: timing and neurobiological aspects related to treatment and diagnosis. Scand J Plast Reconstr Surg Hand Surg 2007;41:153-157.
- Tsuge K. Tendon transfer. In: Tsuge K, ed. Comprehensive Atlas of Hand Surgery. Chicago: Year Book Medical Publishers, 1989:485-544.
- Tubiana R. Problems and solutions in palliative tendon transfer surgery for radial nerve palsy. Tech Hand Up Extrem Surg 2002;6:104-113.
- Walczyk S, Pieniazek M, Pelczar-Pieniazek M, et al. Appropriateness and effectiveness of physiotherapeutic treatment procedure after tendon transfer in patients with irreversible radial nerve injury. Orthop Traumatol Rehabil 2005;7:187-197.
