Comprehensive Introduction and Patho-Epidemiology
Tarsometatarsal interpositional arthroplasty represents a highly specialized, joint-sparing surgical intervention primarily targeting the lateral column of the foot—specifically the complex articulations between the cuboid and the bases of the fourth and fifth metatarsals. In the evolving realm of advanced midfoot reconstruction, the historical paradigm of pan-tarsometatarsal arthrodesis has been rigorously challenged. The contemporary orthopedic consensus now recognizes that while the medial and middle columns demand absolute rigidity to facilitate the propulsive phase of gait, the lateral column must retain its inherent mobility. Iatrogenic ablation of this mobility through arthrodesis frequently results in a rigid, non-compliant foot that is exquisitely prone to adjacent joint degeneration, altered gait kinematics, and catastrophic hardware failure.
The patho-epidemiology of lateral column degeneration is multifactorial, most frequently arising as a late sequela of traumatic injuries to the Lisfranc joint complex. High-energy axial loads applied to a plantarflexed foot, or severe crush injuries, often result in ligamentous disruption or intra-articular fractures extending into the fourth and fifth tarsometatarsal articulations. Even with meticulous open reduction and internal fixation, the sheer kinetic energy imparted to the chondral surfaces frequently precipitates post-traumatic osteoarthritis. Primary idiopathic osteoarthritis of the lateral column is comparatively rare, though it can manifest in patients with underlying biomechanical abnormalities, such as severe pes cavovarus, which abnormally loads the lateral border of the foot during the stance phase of gait.
Inflammatory arthropathies, particularly rheumatoid arthritis, also contribute significantly to the epidemiological burden of midfoot degeneration. In these systemic conditions, chronic synovitis leads to progressive destruction of the articular cartilage and attenuation of the stabilizing ligamentous complexes. For these patients, preserving whatever residual motion remains in the lateral column via interpositional arthroplasty can drastically improve their quality of life, allowing for better accommodation to uneven terrain and reducing the sheer stresses transferred to the compromised hindfoot and ankle joints.
The advent of spherical ceramic implants and refined biological interposition techniques has revolutionized the surgical management of this pathology. By replacing the arthritic, denuded joint surfaces with an inert, highly polished ceramic sphere or an autologous soft-tissue "anchovy," the surgeon effectively eradicates the bone-on-bone nociceptive pain while simultaneously preserving the critical compliance of the lateral column. This procedure, therefore, is not merely a salvage operation, but a sophisticated biomechanical restoration designed to harmonize the complex interplay between the rigid medial lever arm and the mobile lateral shock absorber.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Configuration
A profound mastery of the osteology and articular geometry of the lateral midfoot is an absolute prerequisite for executing a successful tarsometatarsal interpositional arthroplasty. The lateral column is structurally composed of the cuboid and its distal articulations with the bases of the fourth and fifth metatarsals. The distal articular surface of the cuboid is uniquely faceted; it presents a relatively flat, slightly concave facet for the fourth metatarsal and a more obliquely oriented, saddle-shaped facet for the fifth metatarsal. The base of the fourth metatarsal is roughly quadrilateral, articulating proximally with the cuboid, medially with the lateral cuneiform and third metatarsal, and laterally with the fifth metatarsal.
The fifth metatarsal base is characterized by its prominent lateral styloid process, which serves as the critical insertion site for the peroneus brevis tendon and the lateral band of the plantar fascia. The articular surface of the fifth metatarsal base is triangular and articulates exclusively with the cuboid. Understanding this intricate, interlocking osseous architecture is vital during the reaming phase of the arthroplasty, as the surgeon must create a perfectly centered hemispherical recess that respects the native joint line without violating the peripheral cortical rims or compromising the adjacent intermetatarsal articulations.
Ligamentous Anatomy and Dynamic Stabilizers
The stability of the lateral tarsometatarsal joints is governed by a robust network of static ligamentous restraints and dynamic musculotendinous stabilizers. The static restraints are divided into dorsal, plantar, and interosseous tarsometatarsal ligaments. The dorsal ligaments are relatively thin and flat, providing minimal resistance to severe plantarflexion forces. In stark contrast, the plantar ligamentous complex is exceptionally thick, dense, and biomechanically robust. It acts as the primary tension band of the midfoot, preventing dorsal subluxation of the metatarsals during weight-bearing.
During surgical preparation, preservation of this plantar capsuloligamentous hinge is perhaps the most critical technical mandate; aggressive reaming that breaches the plantar cortex will invariably lead to catastrophic dorsal dislocation of the implant and the metatarsal. Dynamically, the lateral column is influenced by the peroneus longus, which courses obliquely through the cuboid groove, and the peroneus brevis, which inserts on the fifth metatarsal base. These tendons exert a constant eversion and plantarflexion moment, which must be accounted for when assessing the intraoperative stability of the seated implant.
Biomechanical Imperatives of the Lateral Column
The biomechanical dichotomy of the human midfoot is a marvel of evolutionary engineering. The medial column (first metatarsal, medial cuneiform) and the middle column (second and third metatarsals, intermediate and lateral cuneiforms) are inherently rigid. They are deeply recessed and tightly bound by the Lisfranc ligamentous complex, functioning as a solid lever arm that facilitates the efficient transfer of energy during the terminal stance and push-off phases of the gait cycle. Arthrodesis of these columns is well-tolerated and frequently utilized to address midfoot arthritis.
Conversely, the lateral column is highly mobile, with biomechanical studies demonstrating approximately 10 to 15 degrees of motion in the sagittal plane, along with significant rotational compliance. This mobility is not vestigial; it is absolutely essential for shock absorption during the initial heel-strike and foot-flat phases of gait. Furthermore, lateral column compliance allows the foot to adapt to uneven, undulating terrain. When the lateral column is erroneously fused, the foot loses this shock-absorbing capacity. The kinetic energy normally dissipated by the lateral tarsometatarsal joints is instead transferred proximally to the transverse tarsal (Chopart) joint or distally to the metatarsal shafts, frequently resulting in accelerated adjacent joint arthrosis and recalcitrant stress fractures.
Exhaustive Indications and Contraindications
Indications for Lateral Column Arthroplasty
The decision to proceed with tarsometatarsal interpositional arthroplasty must be predicated on a rigorous clinical evaluation and a clear understanding of the patient's functional demands. The primary indication is symptomatic, radiographically confirmed primary or post-traumatic osteoarthritis of the fourth and/or fifth tarsometatarsal joints that has proven entirely refractory to a comprehensive regimen of conservative management. This non-operative protocol typically includes custom rigid orthotics with lateral offloading modifications, extended use of a controlled ankle motion (CAM) boot, judicious use of non-steroidal anti-inflammatory drugs (NSAIDs), and fluoroscopically guided intra-articular corticosteroid injections.
A secondary, yet highly prevalent, indication is the presence of combined midfoot degeneration where the medial and middle columns require rigid arthrodesis. In these complex reconstructions, performing a concurrent lateral column interpositional arthroplasty serves as a critical adjunct. It prevents the creation of a completely rigid, non-compliant foot ("block foot"), thereby preserving a functional degree of midfoot suppleness. Additionally, patients with inflammatory arthropathies, such as rheumatoid arthritis, who present with midfoot collapse and lateral column pain, are excellent candidates. In these patients, preserving motion helps to mitigate the stress transferred to other joints that may already be compromised by the systemic inflammatory process.
Absolute and Relative Contraindications
While highly effective in the appropriately selected patient, tarsometatarsal interpositional arthroplasty carries strict contraindications that must be respected to avoid catastrophic failure. The most absolute contraindication is the presence of Neuropathic Arthropathy, commonly known as the Charcot foot. In the setting of profound peripheral neuropathy, loss of protective sensation, and progressive structural collapse, stability absolutely supersedes motion. Attempting a motion-preserving arthroplasty in a Charcot midfoot will inevitably lead to rapid implant subsidence, massive osteolysis, and recurrent deformity. In these scenarios, rigid extended arthrodesis is the only viable surgical option.
Active local or systemic infection is an absolute contraindication to any joint arthroplasty or the implantation of foreign material (such as a ceramic sphere). Severe, uncorrectable bone loss in either the cuboid or the metatarsal bases represents a significant relative, if not absolute, contraindication. If the subchondral bone stock is insufficient to rigidly support the hemispherical implant, subsidence is guaranteed. Furthermore, uncorrected hindfoot deformities (such as severe varus or valgus malalignment) must be addressed either prior to or concurrently with the midfoot arthroplasty. Failure to correct a hindfoot varus, for example, will result in persistent eccentric lateral loading, leading to premature wear, pain, and eventual dislocation of the interpositional implant.
| Clinical Parameter | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Pathology | Post-traumatic OA, Primary OA, Rheumatoid Arthritis | Neuropathic Arthropathy (Charcot), Active Infection | Avascular Necrosis of the Cuboid |
| Biomechanics | Need for shock absorption, uneven terrain accommodation | Need for absolute structural rigidity | Uncorrected severe hindfoot varus/valgus |
| Bone Stock | Intact subchondral bone, minimal cystic changes | Massive osteolysis, active osteomyelitis | Large subchondral cysts requiring grafting |
| Concomitant Surgery | Adjunct to Medial/Middle column arthrodesis | Concomitant lateral column instability | Severe soft tissue compromise/prior flap |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Advanced Imaging
Meticulous preoperative planning begins with a comprehensive clinical examination to localize the exact source of nociception. The surgeon must carefully palpate the fourth and fifth tarsometatarsal joints, differentiating this pain from peroneal tendinopathy, cuboid syndrome, or pathology at the calcaneocuboid joint. Diagnostic, fluoroscopically guided intra-articular injections of local anesthetic (e.g., lidocaine or bupivacaine) into the 4th and 5th TMT joints are highly recommended to definitively confirm that the lateral column is the primary pain generator.
Standard weight-bearing anteroposterior, lateral, and oblique radiographs of the foot are mandatory for the initial assessment of joint space narrowing, subchondral sclerosis, and osteophyte formation. However, a multi-planar Computed Tomography (CT) scan without contrast is considered the gold standard for preoperative templating. Sagittal and coronal CT reconstructions allow the surgeon to precisely map the topography of the articular degeneration, assess the depth of subchondral cysts, and evaluate the integrity of the plantar cortical bone. This three-dimensional understanding is crucial for determining whether the bone stock is sufficient to support a ceramic implant or if a biological "anchovy" interposition will be necessary due to osseous compromise.
Implant Selection and Biological Alternatives
The surgeon must preoperatively decide between utilizing a biological soft-tissue interposition or a synthetic ceramic implant. Biological interposition typically involves harvesting the peroneus tertius tendon or a distally based slip of the extensor digitorum longus (EDL) from the fourth digit. This tissue is rolled into a dense "anchovy," sutured to itself, and interposed into the decorticated joint space. While biological options avoid the risks associated with foreign body implantation, they are prone to gradual subsidence, scarring, and eventual loss of joint space height, which can lead to recurrent impingement pain.
Contemporary orthopedic literature strongly favors the use of spherical ceramic implants (e.g., the Orthosphere, manufactured by Wright Medical/Stryker). These implants are composed of highly polished zirconia ceramic, which is biologically inert, exceptionally resistant to wear, and provides a smooth articulating surface that resists soft-tissue adherence. The ceramic spheres are available in various diameters (typically ranging from 9 mm to 14 mm). Preoperative digital templating on the CT scan helps estimate the required sphere size, ensuring that the implant will adequately tension the joint without overstuffing it, which could lead to adjacent joint subluxation or iatrogenic stiffness.
Anesthetic Considerations and Patient Positioning
Optimization of the anesthetic and positioning strategy is vital for intraoperative efficiency and postoperative patient comfort. The procedure is typically performed under general anesthesia or a robust spinal block, depending on patient comorbidities and anesthesiologist preference. To minimize the requirement for systemic opioids and facilitate a smooth transition to the postoperative phase, the administration of a regional ultrasound-guided popliteal sciatic nerve block is highly recommended. Supplementing this with a saphenous nerve block ensures complete regional anesthesia of the foot and ankle.
The patient is positioned supine on the operating table. A critical positioning maneuver is the placement of a large gel bump under the ipsilateral hip. This internally rotates the entire lower extremity, bringing the lateral aspect of the foot out of its naturally externally rotated resting position and into a direct, perfectly accessible dorsal-vertical view for the surgeon. Alternatively, a semilateral decubitus position utilizing a vacuum beanbag can be employed, though this makes concurrent medial column procedures more challenging. A well-padded pneumatic tourniquet is applied to the proximal thigh or calf. The limb is carefully exsanguinated with an Esmarch bandage, and the tourniquet is inflated to a standard pressure (typically 250-300 mmHg) to guarantee a pristine, bloodless surgical field.
Step-by-Step Surgical Approach and Fixation Technique
Surgical Incision and Neurological Protection
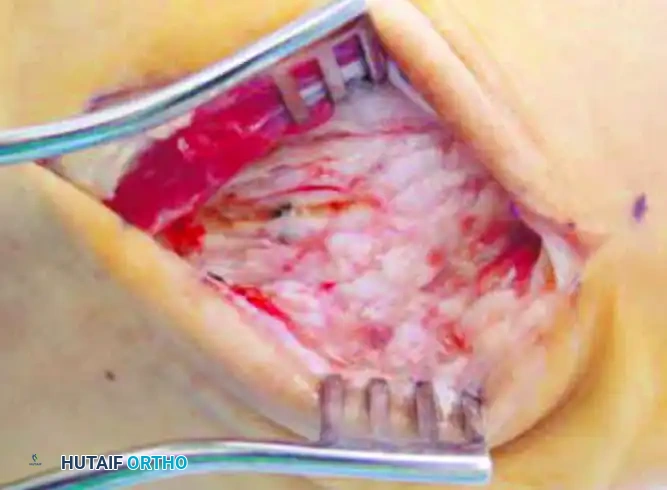
The surgical approach begins with a meticulously planned longitudinal dorsolateral incision. The incision is centered directly over the articulation of the fourth and fifth metatarsals with the cuboid, typically extending from the distal third of the cuboid to the proximal metaphyses of the lateral metatarsals.
Surgical Warning: The superficial dissection in this anatomical region is fraught with neurological hazards. The surgeon must take extreme care to identify, mobilize, and protect the intermediate dorsal cutaneous branch of the superficial peroneal nerve medially, and the terminal branches of the sural nerve laterally. Retraction of these nerves should be performed with vessel loops or blunt, atraumatic retractors. Iatrogenic transection or aggressive traction injury to these nerves will result in a debilitating postoperative neuroma, which often eclipses the pain of the original arthritis.
Once the superficial nerves are safely isolated and retracted, the dissection is deepened through the subcutaneous fat. The extensor retinaculum is incised longitudinally. The extensor digitorum longus (EDL) tendons and the peroneus tertius tendon are identified. Depending on the exact trajectory of the incision and the patient's specific anatomy, these tendons are retracted either medially or laterally to expose the underlying dorsal joint capsule of the fourth and fifth tarsometatarsal joints.
Deep Dissection and Joint Preparation
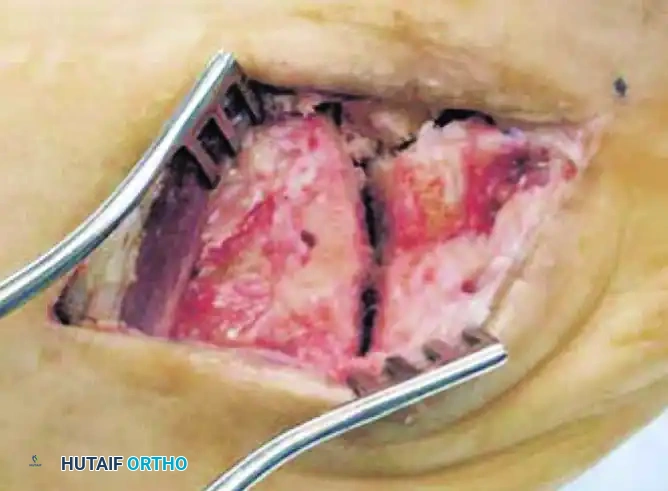
With the extensor tendons retracted, the dorsal capsule of the lateral tarsometatarsal joints is sharply incised. Full-thickness subperiosteal flaps are elevated medially and laterally to expose the dorsal articular margins of the cuboid and the metatarsal bases. At this stage, the surgeon will typically encounter significant dorsal osteophyte formation, which is a hallmark of advanced midfoot osteoarthritis.
Aggressive and meticulous débridement of these dorsal, medial, and lateral osteophytes is mandatory. This osteophyte excision is not merely performed to improve visualization; it is a critical biomechanical step required to remove the mechanical block to motion. A rongeur and a small sagittal saw are utilized to resect the overhanging bone back to the native cortical margins. Following osteophyte resection, a thorough synovectomy is performed using a pituitary rongeur and a motorized shaver to remove all inflamed, hypertrophic synovial tissue that contributes to the patient's pain and swelling.
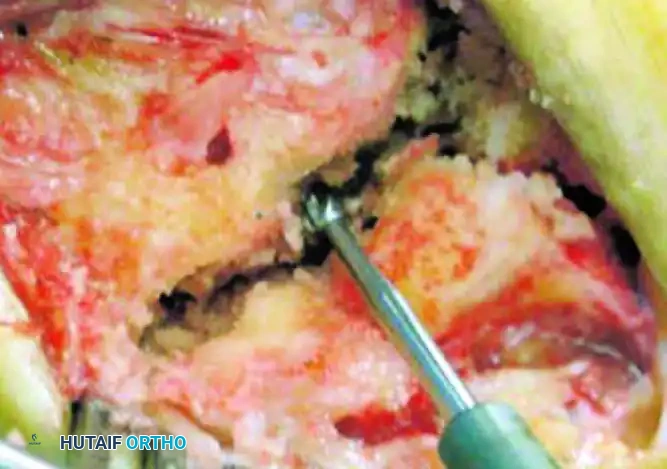
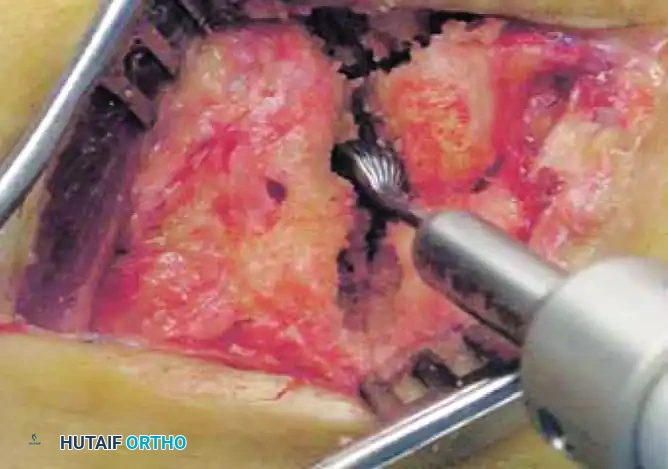
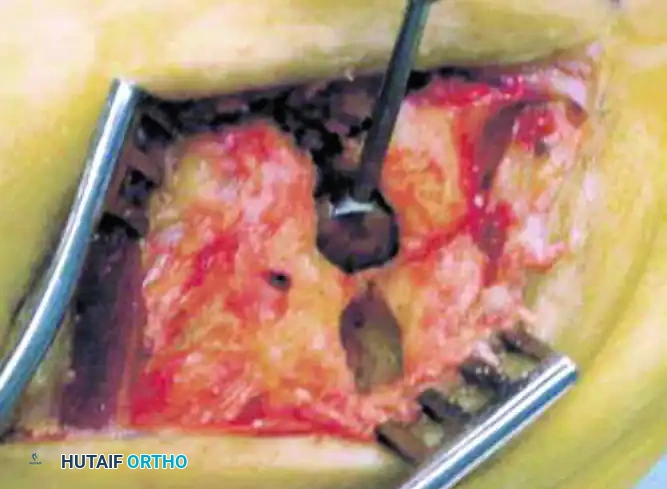
Pilot Hole Creation and Hemispherical Reaming
The preparation of the articular surfaces for the ceramic implant is the most technically demanding phase of the operation. Using a high-speed burr or a small 2.0 mm drill bit, a precise central pilot hole is created in the opposing articular surfaces of the cuboid and the respective metatarsal base. The trajectory of this pilot hole must be perfectly collinear with the anatomical axis of the metatarsal to ensure the implant sits squarely within the joint.
Clinical Pearl: When burring, the surgeon must maintain a hyper-vigilant awareness of depth. It is absolutely imperative to preserve the peripheral cortical rim and, most importantly, the robust plantar ligaments. The plantar capsuloligamentous complex is the primary tension-band stabilizer of the midfoot; violating this structure with the burr will lead to inevitable dorsal subluxation of the metatarsal and catastrophic dislocation of the ceramic implant.
Following the creation of the pilot hole, specialized hemispherical power burrs are utilized to create matching concave recesses on both sides of the joint. The reaming is performed sequentially, starting with a smaller diameter burr and progressively increasing the size. The surgeon must periodically irrigate the joint with cold saline to prevent thermal necrosis of the subchondral bone. The goal is to create a perfectly hemispherical cavity that is deep enough to capture the ceramic sphere while retaining a strong peripheral rim of bone to prevent implant migration.
Trialing, Sizing, and Final Implant Seating
Once the hemispherical recesses are prepared, a trial sizing tool is inserted into the joint space. The sizing phase is critical: the selected implant must provide adequate stability and maintain the anatomical length of the lateral column without "overstuffing" the joint. An overstuffed joint will place excessive tension on the surrounding soft tissues, leading to intractable postoperative stiffness, pain, and potential subluxation of the adjacent intermetatarsal joints. Conversely, an undersized implant will be inherently unstable and prone to dislocation.
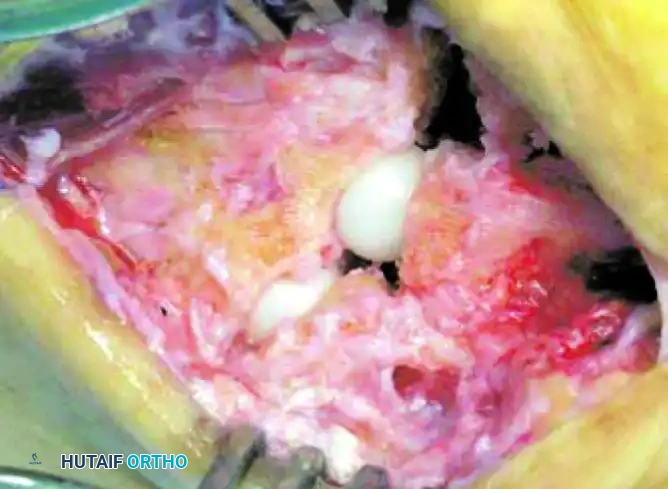
After determining the optimal size through trialing and fluoroscopic verification, the final ceramic implant is brought to the field. To insert the implant without damaging the delicate dorsal cortical rim, a specific maneuver is required. The surgeon or an assistant applies strong longitudinal distal traction to the involved metatarsal while simultaneously applying a forceful plantarflexion moment. This action opens the joint dorsally like a book, allowing the ceramic sphere to be gently dropped and seated deep within the recessed cavity.
Once seated, the traction is released, and the joint is allowed to rest in a neutral position. The surgeon must then verify the stability of the implant by taking the midfoot through a full, simulated range of sagittal and rotational motion. The implant should remain deeply seated, functioning as a smooth, stable pivot point. Final intraoperative fluoroscopy in the AP, lateral, and oblique planes is obtained to definitively confirm the concentric seating of the implant and the restoration of the lateral column length. The wound is then copiously irrigated, and layered closure is performed, prioritizing a watertight capsular closure if the tissue permits.
Complications, Incidence Rates, and Salvage Management
Intraoperative and Early Postoperative Complications
Despite meticulous surgical technique, tarsometatarsal interpositional arthroplasty carries specific inherent risks. Intraoperative complications primarily revolve around iatrogenic fracture of the metatarsal base or the cuboid during the reaming process. This usually occurs if the surgeon fails to center the pilot hole or uses an excessively large burr that breaches the thin cortical walls. If a cortical breach occurs, the ceramic implant may lack sufficient containment. In such scenarios, the surgeon must be prepared to abandon the arthroplasty and convert to a primary arthrodesis utilizing structural bone graft and rigid plate fixation.
Early postoperative complications include wound dehiscence and superficial surgical site infections, particularly in patients with compromised microvascular circulation (e.g., diabetics, smokers). Deep space infections are rare but catastrophic, as the ceramic implant acts as a foreign body nidus for biofilm formation. In the event of a deep infection, aggressive surgical irrigation and débridement, complete removal of the ceramic implant, and placement of an antibiotic-impregnated cement spacer are mandatory, followed by a prolonged course of culture-directed intravenous antibiotics.
Late Complications and Implant Failure
The most common late complication is implant subsidence or dislocation. Subsidence typically occurs secondary to unrecognized preoperative cystic degeneration of the subchondral bone, over-reaming during preparation, or premature weight-bearing by the non-compliant patient. Dislocation almost exclusively results from violation of the plantar capsuloligamentous hinge during surgery. If the implant subsides significantly, the patient will experience a recurrence of their preoperative pain due to impingement of the peripheral cortical margins.
Nerve injury, specifically to the sural or intermediate dorsal cutaneous nerves, can lead to the formation of painful neuromas. This complication is entirely technique-dependent and emphasizes the need for pristine superficial dissection. If a neuroma develops and fails conservative management (e.g., gabapentinoids, targeted steroid injections), surgical excision and burying of the proximal nerve stump into deep muscle belly may be required.
| Complication | Estimated Incidence | Preventative Strategy | Salvage/Management |
|---|---|---|---|
| Implant Subsidence | 5 - 10% | Pre-op CT to assess bone stock; avoid over-reaming | Revision to larger implant or conversion to arthrodesis |
| Implant Dislocation | < 5% | Strict preservation of the plantar ligamentous hinge | Open reduction, capsular repair, or conversion to fusion |
| Neuroma Formation | 3 - 8% | Meticulous blunt retraction of superficial nerves | Excision of neuroma, proximal stump burial |
| Persistent Stiffness/Pain | 10 - 15% | Avoid "overstuffing" the joint with an oversized implant | Physical therapy; rarely requires implant down-sizing |
| Deep Infection | < 2% | Strict sterile technique, prophylactic antibiotics | Implant removal, antibiotic spacer, delayed fusion |
Phased Post-Operative Rehabilitation Protocols
Isolated Lateral Column Arthroplasty Rehabilitation
The postoperative rehabilitation protocol is entirely contingent upon whether the tarsometatarsal interpositional arthroplasty was performed as an isolated procedure or as part of a broader midfoot reconstruction. For the rare isolated lateral column arthroplasty, the initial phase (Weeks 0-2) focuses strictly on wound healing and edema control. The patient is placed in a bulky, well-padded posterior splint in neutral dorsiflexion and is instructed to remain strictly non-weight bearing. Elevation of the limb above the level of the heart is critical during this phase to mitigate swelling and prevent wound complications.
At the 2-week postoperative mark, the splint is removed, and the surgical incision is inspected. If the wound is fully epithelialized, the sutures or staples are removed. The patient is then transitioned into a removable controlled ankle motion (CAM) boot walker. From Weeks 2 to 6, weight-bearing is progressively advanced as tolerated within the protection of the boot. Active and active-assisted range of motion exercises for the ankle and toes are initiated to prevent tendon adhesions. By Week 6, assuming clinical progress is satisfactory, the patient is transitioned from the CAM boot to a supportive, wide toe-box athletic shoe equipped with a rigid carbon-fiber insert. This insert acts to limit excessive bending stresses across the healing midfoot. Formal physical therapy is commenced to restore normal gait mechanics, enhance proprioception, and strengthen the dynamic stabilizers of the foot.
Combined Medial and Lateral Column Reconstruction Protocols
In the vast majority of clinical scenarios, the lateral column arthroplasty is performed in conjunction with a rigid arthrodesis of the medial and/or middle columns. In these complex cases, the rehabilitation timeline is entirely dictated by the biological requirements of the fusion sites, not the arthroplasty. The patient must remain strictly non-weight bearing in a short-leg cast or a locked rigid boot for a minimum of 8 to 10 weeks. Premature weight-bearing in this setting risks not only subsidence of the lateral implant but, more critically, non-union or hardware failure at the medial arthrodesis sites.
Serial radiographs are obtained at 4, 8, and 12 weeks postoperatively. Once definitive radiographic evidence of bridging trabecular bone is observed across the medial and middle column arthrodesis sites (typically around the 8-to-10-week mark), a graduated weight-bearing protocol is initiated. The patient begins partial weight-bearing in a CAM boot, slowly advancing to full weight-bearing over a 4-week period.

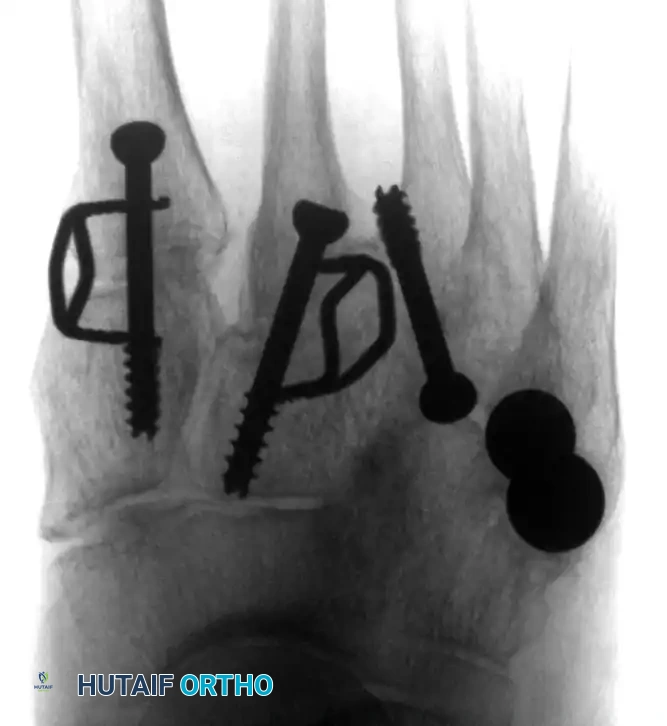
(Above: Anteroposterior and oblique radiographic appearance 10 months after a combined medial/middle column fusion with lateral tarsometatarsal ceramic interpositional arthroplasty. Note the preservation of the lateral joint space and stable seating of the spherical implants.)
The transition to standard footwear in these combined cases is often delayed until 12 to 14 weeks postoperatively. Physical therapy in this demographic is prolonged and intensive, focusing on retraining the patient to ambulate with a partially fused midfoot while maximizing the preserved compliance of the lateral column interposition.
Summary of Landmark Literature and Clinical Guidelines
The evolution of lateral column midfoot surgery from routine arthrodesis to motion-preserving arthroplasty is heavily supported by contemporary biomechanical and clinical literature. Early historical series documenting pan-tarsometatarsal fusions frequently reported high rates of patient dissatisfaction, primarily driven by intractable lateral foot pain, difficulty walking on uneven ground, and the development of adjacent joint arthritis. Biomechanical cadaveric studies, notably those by specialized foot and ankle researchers, demonstrated that fusing the fourth and fifth tarsometatarsal joints significantly increases the contact
